1155
Higher Overall Pulsatile CSF flow Variance in Congenital Heart Disease Predict Poor Executive Function1Department of Bioengineering, University of Pittsburgh, Pittsburgh, PA, United States, 2Department of Radiology, University of Pittsburgh School of Medicine, Pittsburgh, PA, United States, 3Department of Biomedical Informatics, University of Pittsburgh School of Medicine, Pittsburgh, PA, United States, 4Learning and Development Center, Child Mind Institute, New York, NY, United States, 5Department of Developmental Biology, University of Pittsburgh, Pittsburgh, PA, United States
Synopsis
Keywords: Adolescents, Pediatric, Congenital Heart Disease Neurodevelopment Cerebrospinal Fluid Flow
Motivation: Examine cerebrospinal fluid (CSF) flow abnormalities in congenital heart disease (CHD) and develop an evaluation method to measure the CSF flow variance over the entire CSF flow cycle.
Goal(s): Determine CSF flow difference between CHD and healthy controls. Evaluate effectiveness of new method to measure CSF flow variance.
Approach: Use phase contrast MRI to acquire CSF flow velocity over the pulsatile flow cycle. Model consensus CSF flow of study cohort and calculate each participant’s flow variance using root mean square deviation.
Results: CHD had greater pulsatile CSF flow variance, especially in CHD with single ventricle. Higher flow variance predicted poor working memory outcomes.
Impact: This study expands our understanding of CSF flow abnormality in CHD and its potential for predicting executive function deficit. A new method measuring CSF flow variance over the entire flow cycle offers an evaluation of CSF flow abnormalities more comprehensively.
INTRODUCTION
Increased cerebrospinal fluid (CSF) volumes are frequently observed in congenital heart disease (CHD) neurodevelopmental studies.1-5 However, from glymphatic system studies, the CSF circulation is shown to play an important role in nutrient distribution, waste removal, and neurogenesis.6,7 Prolonged interference with this homeostatic function may lead to neuroinflammation and neurodevelopmental deficits.8 The flow of CSF through the ventricles and cisterns of the brain are pulsatile, driven mainly by cardiopulmonary circulation9 with arterial pulsations as one of the primary drivers.10 Given the etiology of heart defects and subsequent repairs, this circulatory mechanism in CHD might be impaired with resultant perturbation on the CSF circulation, especially in complex heart defects such as hypoplastic left heart syndrome (HLHS) that result in hypoxia and cyanosis. CSF flow has yet to be studied in CHD. Additionally, current MRI based measurements for flow such as average or peak velocity and flow volumes, developed for assessing hemodynamics, might be inadequate to study CSF flow variance in CHD. In this study we determined whether there were CSF flow abnormalities in pediatric and young adult CHD population compared to healthy controls. Additionally, we developed a new evaluation method to measure the flow difference over the entire pulsatile CSF flow cycle and identify any potential associations with abnormal hemodynamics. Lastly, we assessed whether altered CSF flow dynamics predicted poor executive cognitive function in CHD.METHODS
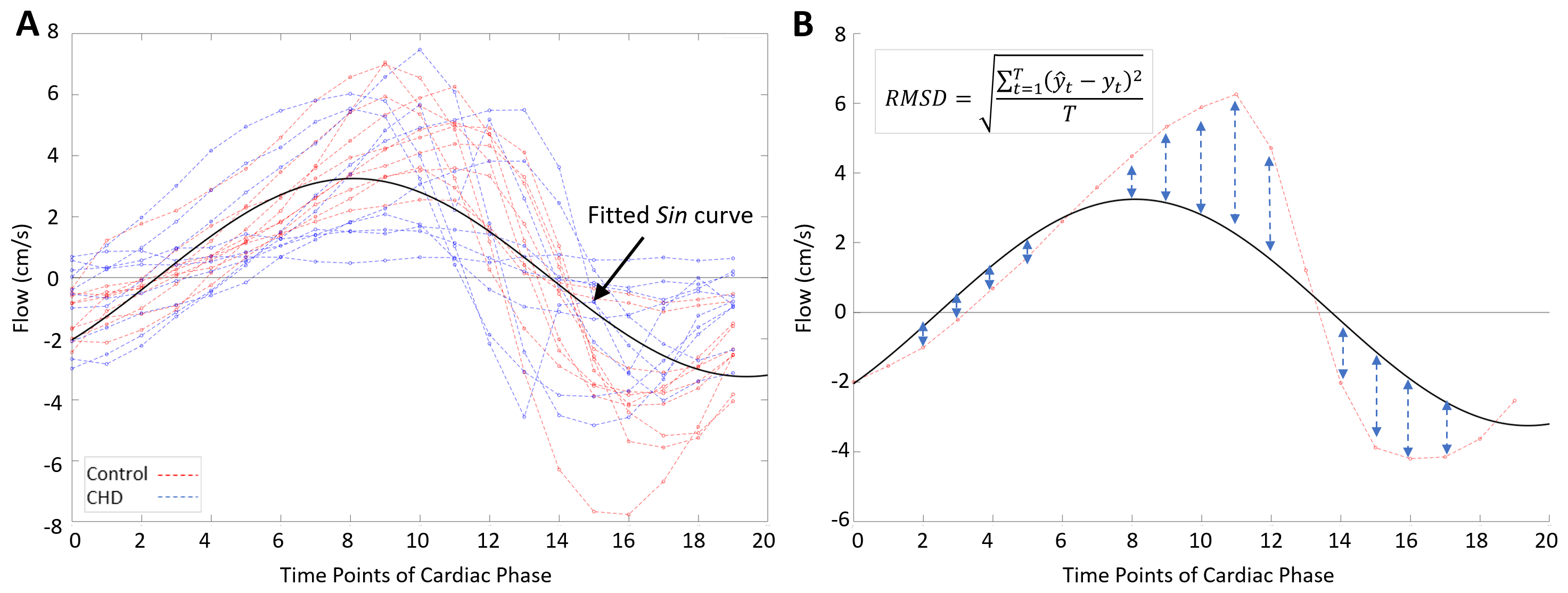
A total of 64 child and young adult participants (CHD=24, female=9, 15.21±7.56 years; healthy controls=40, female=21, 13.84±4.18 years) were scanned on a 3T Skyra scanner (Siemens Healthcare, Erlangen, Germany) with 32-channel head coil. The CSF flow was measured across the lumen of the Aqueduct of Sylvius using cardiac-gated phase contrast gradient echo sequence with the following parameters: velocity encoding=12.5 cm/s; TR/TE=9.66/30.40ms; flip-angle=15°; matrix=256 x 256; resolution=0.6mm x 0.6mm; slice thickness=5mm). The scans were processed using an in-house MATLAB program (validated with Siemens ARGUS software) to calculate anterograde and retrograde peak velocities and flow volumes, average velocity, and net flow volume that passed through the lumen. To evaluate CSF flow variance throughout the entire pulsatile CSF cycle, we employed twenty velocity measurements sampled over the cycle from each participant and modeled a sinusoidal function representing the consensus CSF flow (Figure 1A). Subsequently, we determined the degree of difference of each participant’s CSF flow from the consensus CSF flow by calculating root mean squared deviation (RMSD) (Figure 1B). The RMSD quantifies the degree of difference with higher values indicating greater dissimilarity.The participants completed executive function evaluations for the following domains with corresponding tests: (1)Inhibition - Delis-Kaplan Executive Function System (D-KEFS) Color-Word-Interference Test; (2)Mental Flexibility - D-KEFS Verbal Fluency Test; (3)Working Memory - Wechsler Adult Intelligence Scale 4th Edition (WAIS-IV) Letter-Number Sequencing.
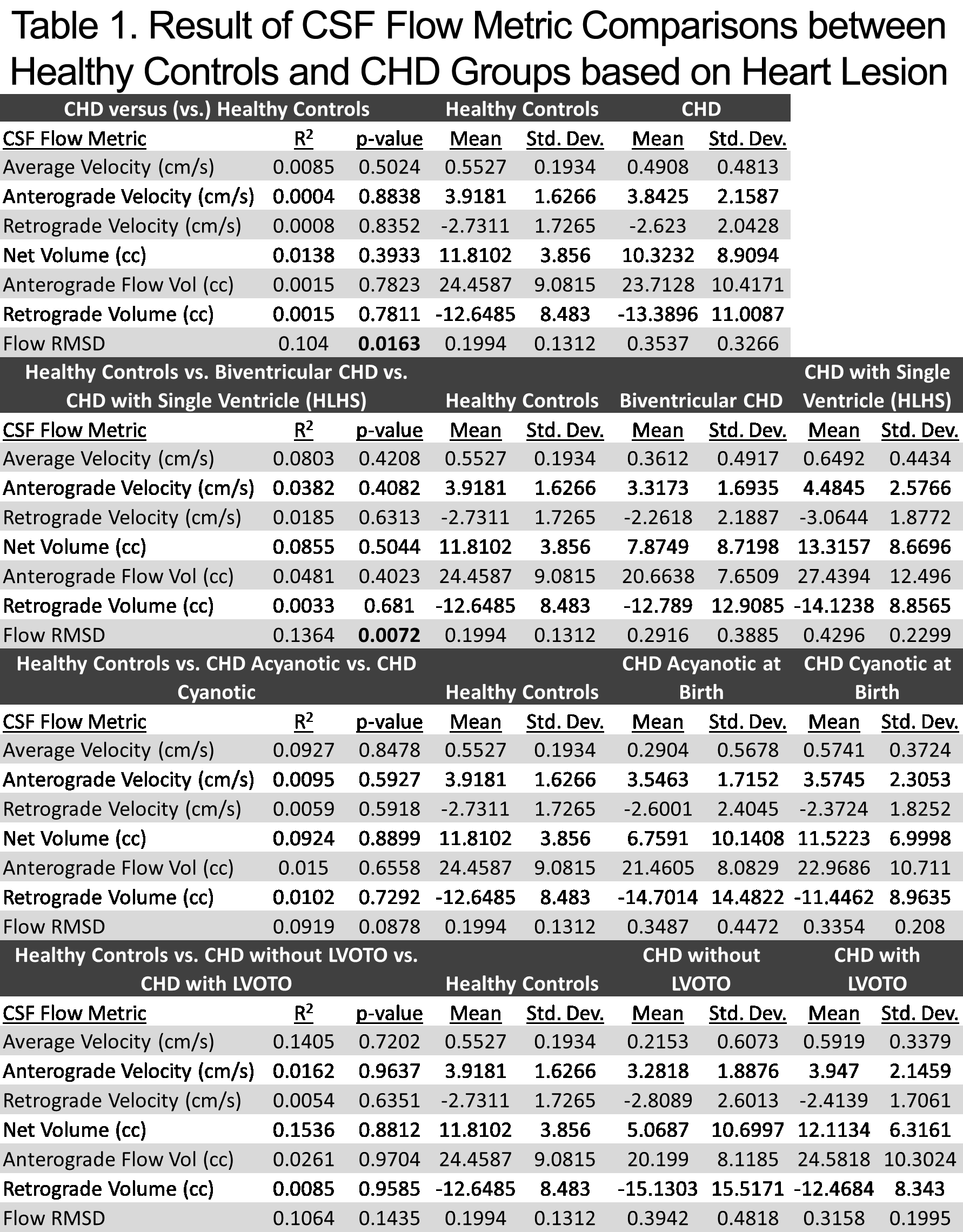
The flow velocities, flow volumes, and the overall flow variance (Flow RMSD) were compared between CHD and healthy control groups using Student’s T-Test. This was followed by quantifying differences in these CSF flow metrics between healthy controls and CHD subgrouping based on the type of heart defect at birth – HLHS, cyanotic, or left ventricular outflow tract obstruction (LVOTO) – using analysis of variance (ANOVA). Lastly, a multivariable regression was performed comparing executive function outcomes with CSF flow metrics as primary exposure – and maternal education, socioeconomic status, and number of cardiac ventricles as covariates.
RESULTS
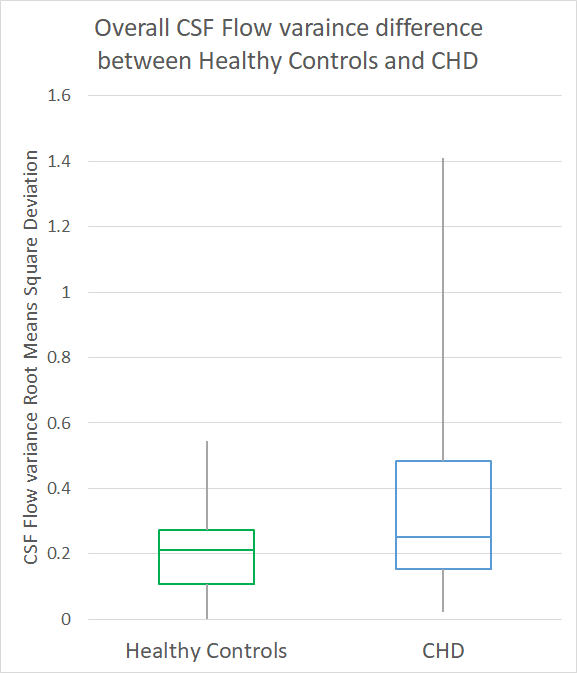
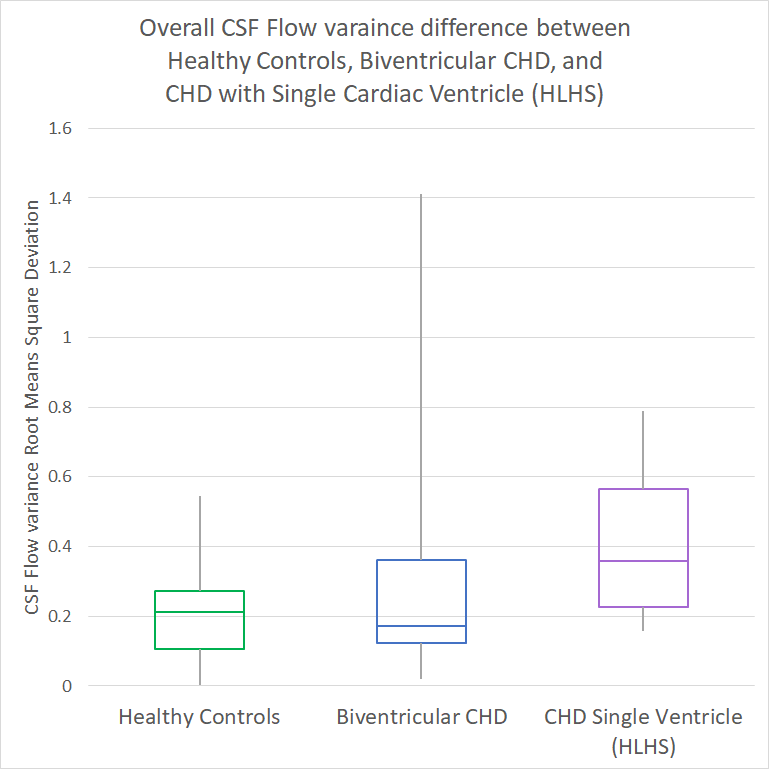
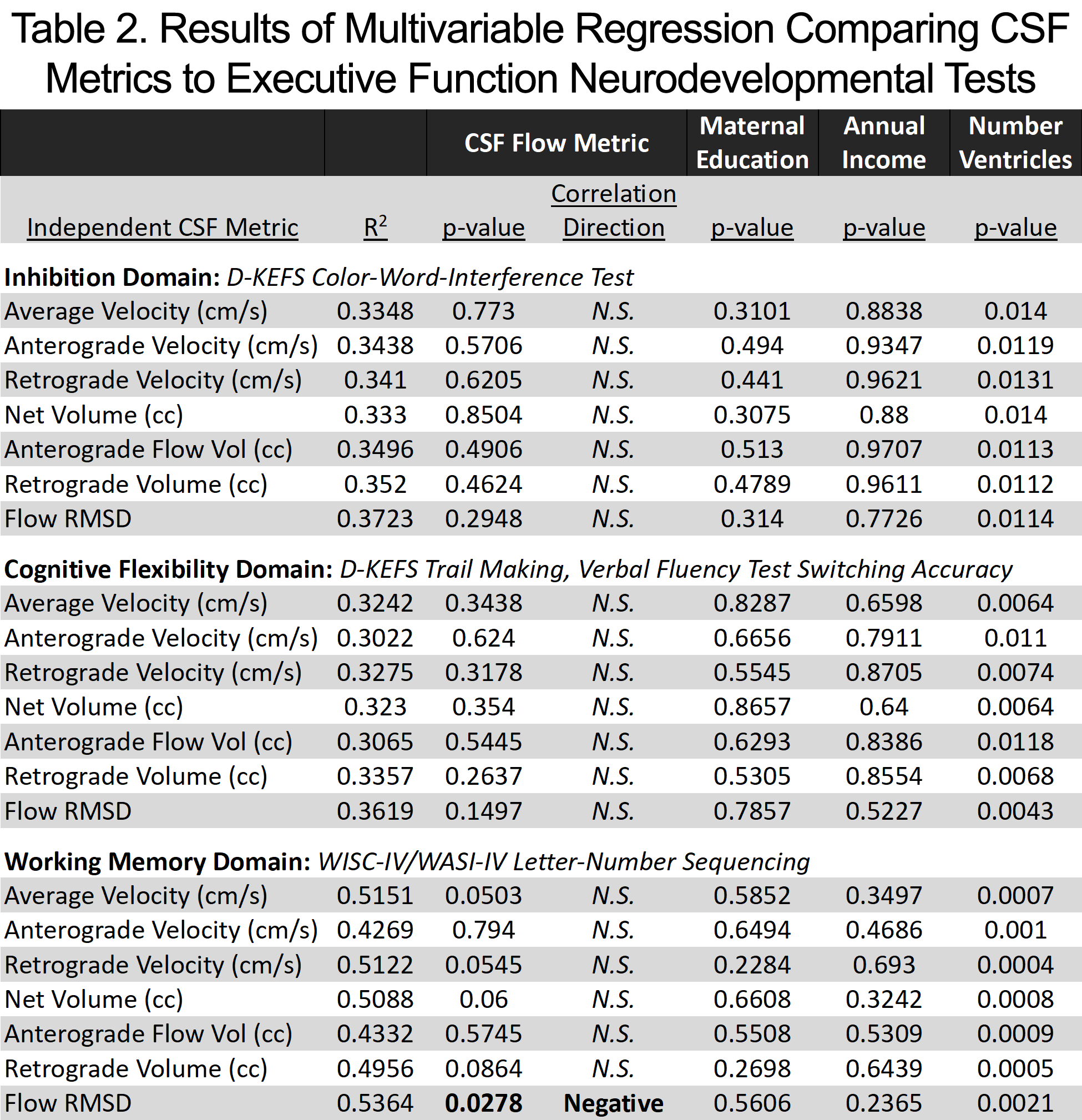
The CHD group demonstrated higher overall Flow RMSD over the entire CSF flow cycle compared to controls (p=0.0163) as shown in Table 1 and Figure 2. In the ANOVA analysis, CHD group with HLHS demonstrated higher overall flow variance compared to both controls and CHD group born with both ventricles (p=0.0072), and the latter two groups were not significantly different (p=0.0925).Higher flow RMSD predicted poorer working memory outcome (p=0.0278) but not inhibition or mental flexibility (Table 2). In contrast, there were no significant differences in velocities or flow volumes between CHD and controls, nor did these variables predict outcomes.DISCUSSION
The CHD group exhibited higher overall CSF flow variance over the entire CSF flow cycle, and it is the group with HLHS that demonstrated the highest variance. Correspondingly, higher overall CSF flow variance also predicted poorer executive functioning, specifically working memory. These findings suggest that impaired CSF flow dynamics in CHD patients may be characterized by quantitative metrics that account for cardiac cycle dynamics and may be related to aberrant CSF pulsatility. These flow aberrations may also be linked to neurodevelopmental deficits. Further studies are needed to investigate possible mechanistic etiologies of aberrant CSF pulsatility (i.e. vascular stiffness, altered visco-elastic properties of tissue, or glial-lymphatic disturbances), which might result in evolving small vessel disease (including microbleeds).Acknowledgements
Grant Support from: Department of Defense [Grant reference: W81XWH-16-1-0613], University of Pittsburgh Clinical and Translational Science Institute (CTSI UL1 TR0018570), and National Institutes of Health, National Heart, Lung, and Blood Institute [Grant reference: F31 HL165730-01]References
- Panigrahy A, Lee V, Ceschin R, et al. Brain dysplasia associated with ciliary dysfunction in infants with congenital heart disease. The Journal of pediatrics. 2016;178:141-148. e1.
- Heye KN, Knirsch W, Latal B, et al. Reduction of brain volumes after neonatal cardiopulmonary bypass surgery in single-ventricle congenital heart disease before Fontan completion. Pediatric research. 2018;83(1):63-70.
- Reich B, Heye KN, Tuura ROG, et al. Interrelationship between hemodynamics, brain volumes, and outcome in hypoplastic left heart syndrome. The Annals of thoracic surgery. 2019;107(6):1838-1844.
- Kelly CJ, Makropoulos A, Cordero-Grande L, et al. Impaired development of the cerebral cortex in infants with congenital heart disease is correlated to reduced cerebral oxygen delivery. Scientific reports. 2017;7(1):1-10.
- Ng IH, Bonthrone AF, Kelly CJ, et al. Investigating altered brain development in infants with congenital heart disease using tensor-based morphometry. Scientific reports. 2020;10(1):1-10.
- Ueno H. MOTOR PROTEINS OF CILIA. Integrated Nano-Biomechanics. 2018:155.
- Louvi A, Grove EA. Cilia in the CNS: the quiet organelle claims center stage. Neuron. 2011;69(6):1046-1060.
- Iliff JJ, Wang M, Liao Y, et al. A paravascular pathway facilitates CSF flow through the brain parenchyma and the clearance of interstitial solutes, including amyloid β. Science translational medicine. 2012;4(147):147ra111-147ra111.
- Battal B, Kocaoglu M, Bulakbasi N, Husmen G, Tuba Sanal H, Tayfun C. Cerebrospinal fluid flow imaging by using phase-contrast MR technique. The British journal of radiology. 2011;84(1004):758-765.
- Mestre H, Tithof J, Du T, et al. Flow of cerebrospinal fluid is driven by arterial pulsations and is reduced in hypertension. Nature communications. 2018;9(1):1-9.
Figures