1133
Neuroimaging of Serotonergic and Psychedelic Agonist Drug Challenges in Non-Human Primates1Radiology, Athinoula A. Martinos Center for Biomedical Imaging, Harvard Medical School, Massachusetts General Hospital, Boston, MA, United States, 2Neurobiology Research Unit, Copenhagen University Hospital, Rigshospitalet, Copenhagen, Denmark, 3Department of Medicine, Faculty of Health and Medical Sciences, University of Copenhagen, Copenhagen, Denmark, 4Department of Drug Design and Pharmacology, University of Copenhagen, Copenhagen, Denmark
Synopsis
Keywords: Pharmacology, Translational Studies, Psychedelics; phMRI; fMRI; Pharmacology; 5-HT2AR
Motivation: Acute effects of psychedelic drugs are under-reported in neuroimaging studies, warranting further investigation of their immediate pharmacology to explore the potential to monitor treatment response with imaging.
Goal(s): Our goal was to assess acute impacts of serotonergic (psychedelic and non-psychedelic) agonists on hemodynamics in non-human primates (NHP).
Approach: Pharmacological-MRI (phMRI) was used to measure cerebral blood volume (CBV) changes by psilocybin, lisuride and 25CN-NBOH.
Results: Psilocybin and lisuride induced bi-phasic hemodynamic response, whereas 25CN-NBOH was monophasic. Bi-phasic phenomena may be due to non-selectivity of agonist drugs. Elevated CBV at higher psilocybin doses persists longitudinally, while lisuride and 25CN-NBOH modulations trend toward baseline.
Impact: Bi-phasic signal profiles and downstream impacts to cerebral hemodynamics may reflect non-selective targeting of psilocybin and lisuride, highlighting the sensitivity of phMRI in drug evaluation.
Introduction
Classical psychedelic substances like psilocybin act as agonists to the serotonin 2A receptor (5-HT2AR) and have received enormous attention for positive effects on disorders such as depression1 and alcoholism.2 Neuroimaging studies on the effects induced by these drugs typically report on functional connectivity,3–5 but key gaps in the pharmacology of these substances remain. Specifically, the immediate effects of psychedelic drugs on hemodynamics in the acute phase are under-investigated. This novel work evaluates partial agonists to 5-HT2AR with psilocybin (non-selective, psychedelic), lisuride (non-selective, non-psychedelic) and 25CN-NBOH (selective, psychedelic) on cerebral hemodynamics with pharmacological MRI (phMRI).Methods
3T Siemens TIM-Trio with a custom 8-channel head coil was used for neuroimaging. Anesthetized NHP were maintained at 1.0-1.2% isofluorane. An anatomical 1mm isotropic T1-weighted MPRAGE (TE1/TE2/TE3/TE4 = 1.64/3.5/5.36/7.22 ms, TR = 2530 ms, TI = 1200 ms, flip angle = 7°) was acquired. For fMRI, NHP were injected with Ferumoxytol (MION; 10mg/kg) to improve SNR. EPI (TE/TR=22/3000ms, 1.3mm isotropic resolution) was acquired for 100 minutes (2000 repetitions). NHP received an i.v. solution of Psilocybin (30μg/kg, N=2; 60μg/kg, N=3; 90μg/kg, N=2), Lisuride (5μg/kg, N=2), and 25CN-NBOH (30μg/kg, N=3). Preprocessing included slice-timing correction, motion-correction, brain extraction, registration to a brain template, bias-field correction, and 4mm spatial smoothing. Data were fit to a bi-phasic gamma function (γ1, γ2) corresponding to drug injection time (t0), time to first peak (τ2) of signal change for γ1 and time to second peak (τ2) of signal change for γ2. A monophasic gamma function was used for 25CN-NBOH. Estimations of cerebral blood volume (CBV) changes for γ1 and γ2 were calculated as:ΔCBV(%) = ln(Sτ1,2/Spost)/ln(Spost/Spre) * 100
Sτ1,2 is the signal measured at τ1, τ2, Spre is the average signal prior to MION injection, and Spost is the average signal after to MION injection before the drug injection.
Results
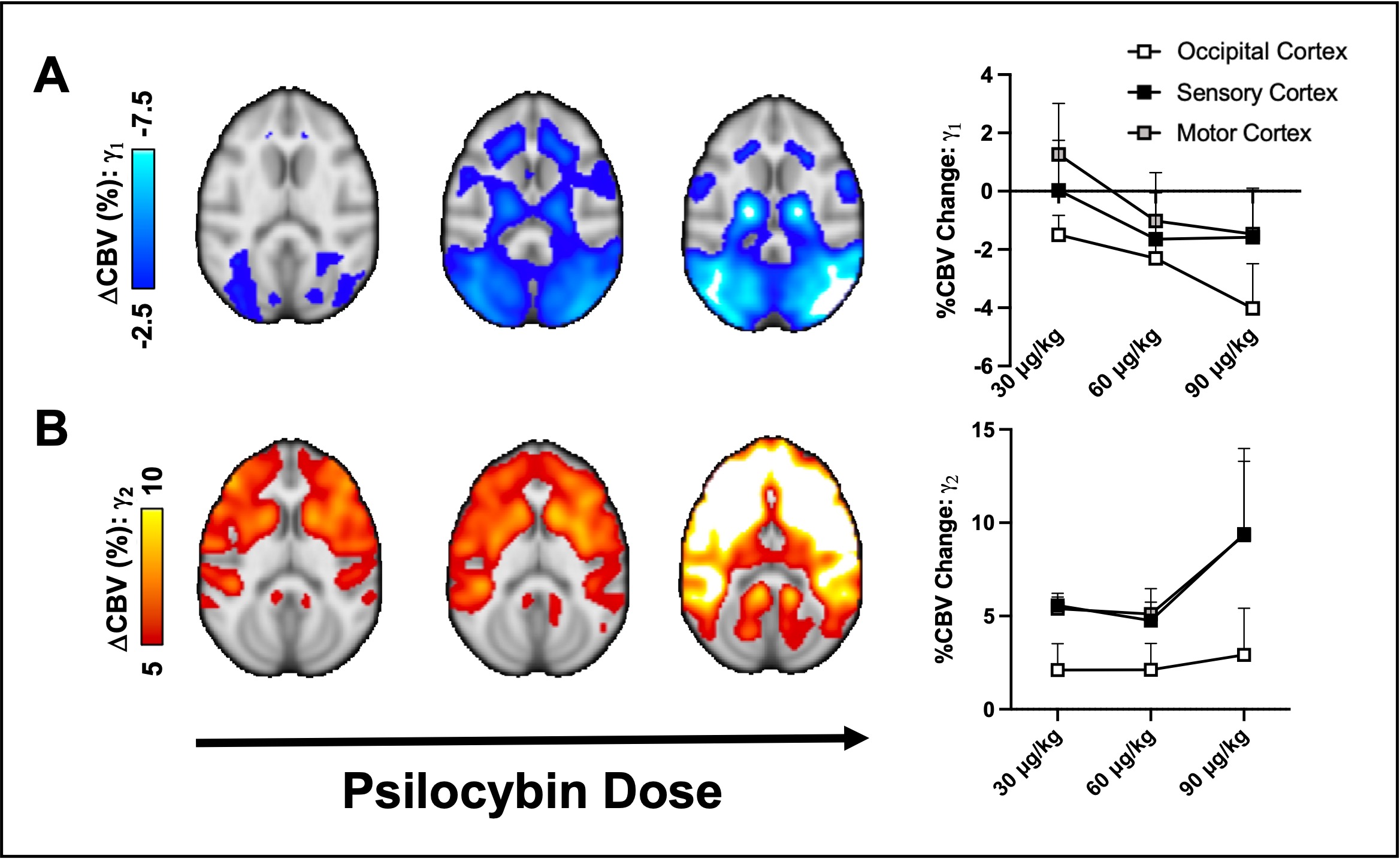
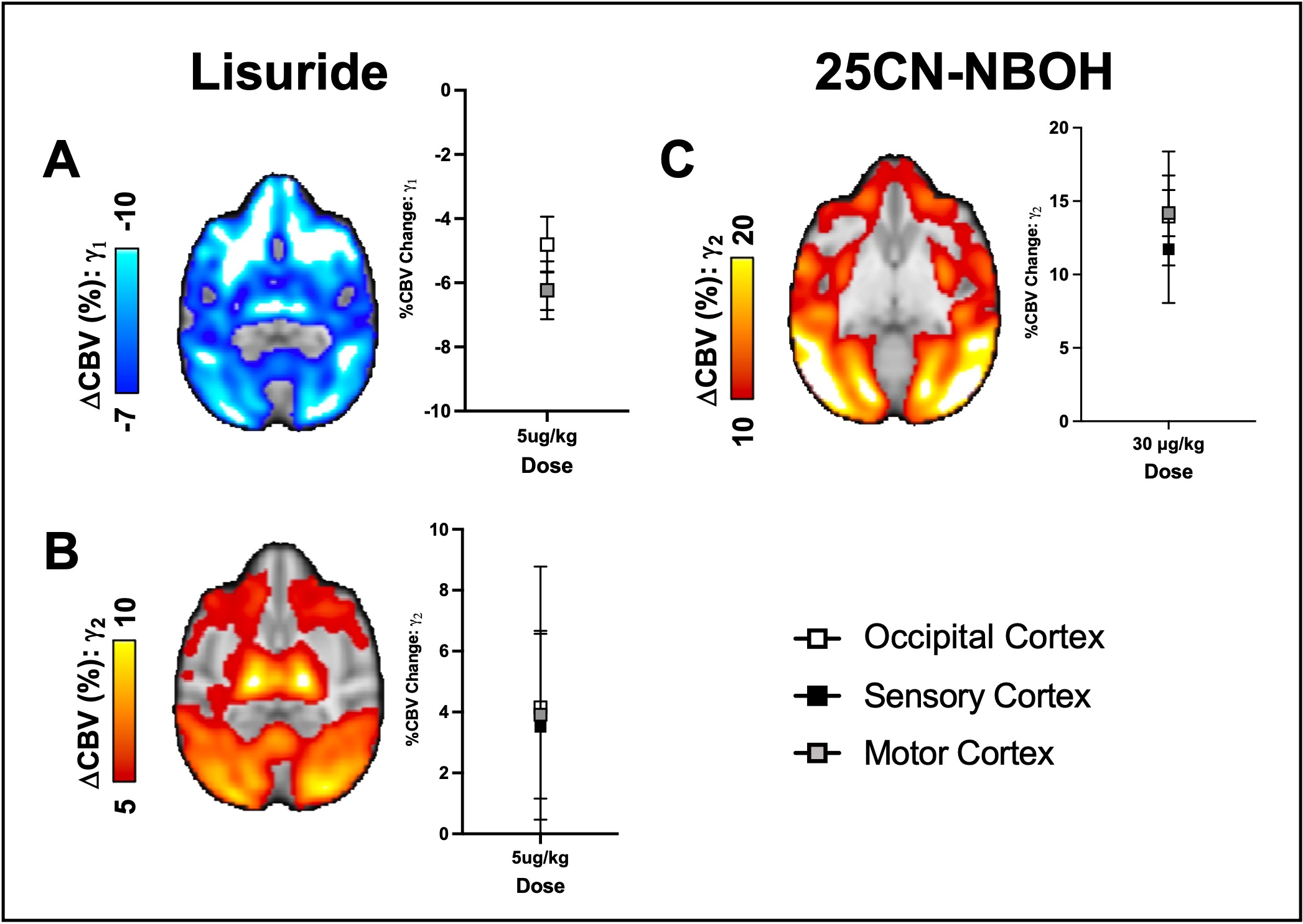
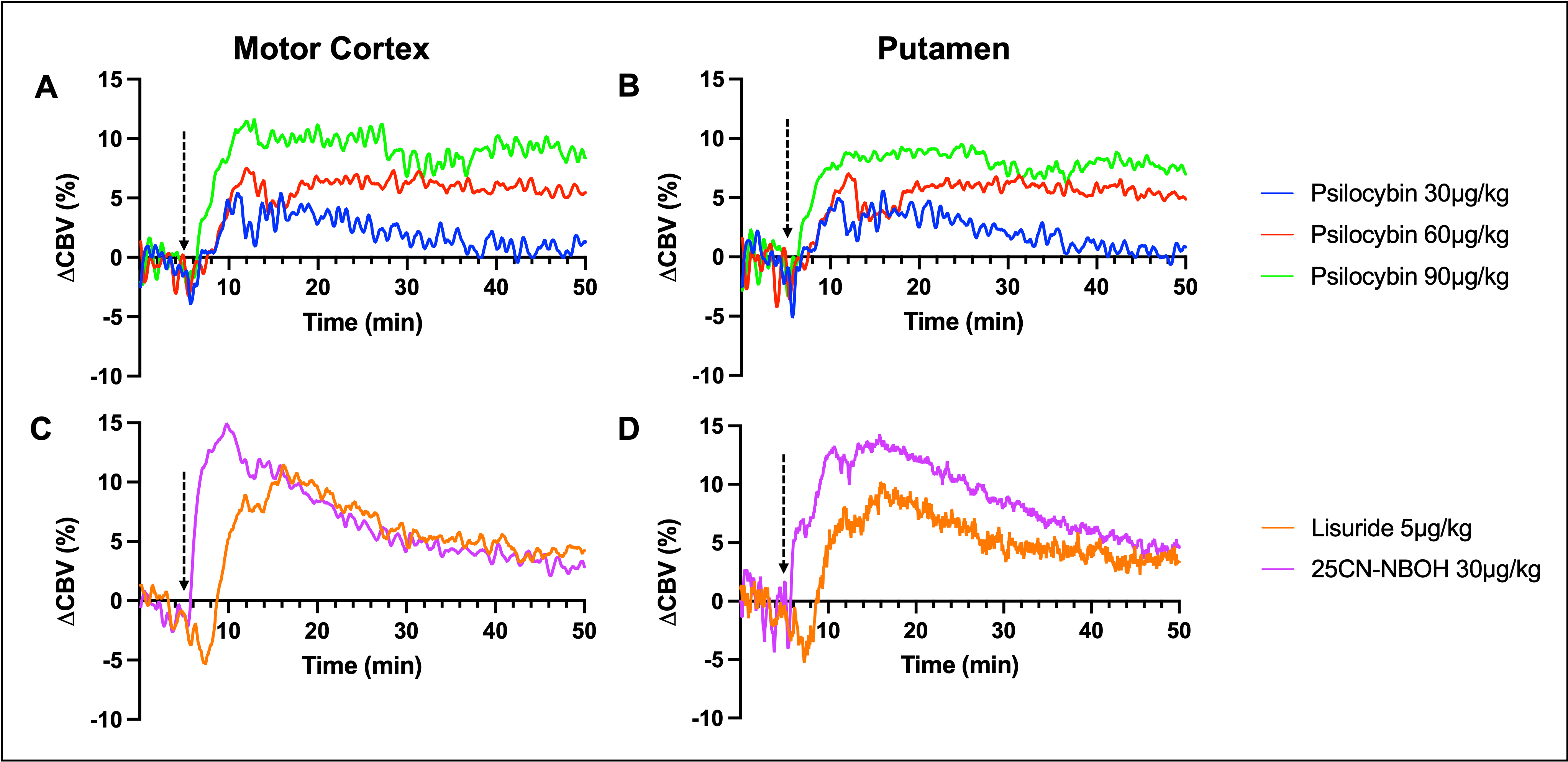
A bi-phasic phMRI response was observed for psilocybin (Fig. 1) and lisuride (Fig 2A,B). For psilocybin, 30, 60μg/kg doses resulted in similar ΔCBVγ1 and ΔCBVγ2 responses, while more pronounced ΔCBVγ1 and ΔCBVγ2 (~-4% in occipital regions and ~+10% in sensorimotor areas, respectively) were observed at 90μg/kg. Distributions in negative and positive changes in CBV were evident in both cortical and subcortical areas. Lisuride (Fig. 2A, B) had different ΔCBV spatial distributions than psilocybin, but still included cortical and subcortical domains with a bi-phasic response. 25CN-NBOH (Fig. 2C) at 30μg/kg was unique as it had only an observed increase (monophasic) in CBV, between +10-15% largely in sensorimotor and occipital regions. Temporal profiles of ΔCBV were also generated for each drug (Fig. 3). Psilocybin typically exhibited dose-dependent and longitudinally elevated CBV over the full time-course of scanning, particularly at the 60 and 90μg/kg doses. In contrast, both lisuride and 25CN-NBOH CBV peaked and exhibited measurable decreases in CBV towards baseline (ΔCBV at or near 5% from baseline).Discussion
The bi-phasic profiles induced by non-selective agonists psilocybin and lisuride are likely reflective of action at multiple receptors corresponding to cascading and downstream effects on vasculature. 25CN-NBOH had only a monophasic response and is one of the most selective 5-HT2AR agonists, supporting this notion. Additionally, previous works have suggested bi-phasic signal response to drug challenge may be due to a combination of inhibitory and excitatory action induced by agonists.6 It is also possible that varying signal profiles could be influenced by mixed serotonin receptor subtype expression in the vasculature directly. Future studies utilizing selective antagonists, in combination with psilocybin and lisuride, may help support our hypothesis. Notwithstanding the local minima/maxima CBV changes, the durations at which psilocybin perturbs CBV longitudinally must also be considered.Conclusions
The bi-phasic phenomenon (1) highlights the importance of phMRI techniques to provide insights of the acute stages of drug challenges and (2) may assist in the interpretation of underlying mechanisms of psilocybin, among other drugs, and induced activation of individual or multiple serotonergic-receptor subtypes. Study in larger cohorts and additional non-selective agonist and psychedelic substances (e.g., LSD) is warranted to identify potential imaging signatures of psychedelic-specific mechanisms using these methods.Acknowledgements
AB is supported by the NIH training grant 5T32AG66592-2. HDH: BBRF Young Investigator grant and Lundbeck Foundation (R293-2018-738) supported the Psilocybin work. Additional Pilot Funding from the Athinoula A. Martinos Center for Biomedical Imaging, Department of Radiology, Massachusetts General Hospital. NIH Shared Instrument Grants: S10RR017208, S10RR026666, S10RR022976, S10RR019933, and S10RR023401, S10OD023517.References
1. Griffiths, R. R. et al. Psilocybin produces substantial and sustained decreases in depression and anxiety in patients with life-threatening cancer: A randomized double-blind trial. J Psychopharmacol 30, 1181–1197 (2016).
2. Krebs, T. S. & Johansen, P. Ør. Lysergic acid diethylamide (LSD) for alcoholism: Meta-analysis of randomized controlled trials. Journal of Psychopharmacology 26, 994–1002 (2012).
3. Carhart-Harris, R. L. et al. Functional connectivity measures after psilocybin inform a novel hypothesis of early psychosis. Schizophr Bull 39, 1343–1351 (2013).
4. Daws, R. E. et al. Increased global integration in the brain after psilocybin therapy for depression. Nat Med 28, 844–851 (2022).
5. Madsen, M. K. et al. Psilocybin-induced changes in brain network integrity and segregation correlate with plasma psilocin level and psychedelic experience. European Neuropsychopharmacology 50, 121–132 (2021).
6. Hansen, H. D. et al. Functional characterization of 5-HT1B receptor drugs in non-human primates using simultaneous PET-MR. The Journal of Neuroscience 44, 10671–10678 (2017).
Figures