1119
Disrupted functional connectivity architectures of neural circuits in obsessive-compulsive disorder1Department of Radiology and Huaxi MR Research Center (HMRRC), Functional and Molecular lmaging Key Laboratory of Sichuan Province, Frontiers Science Center for Disease-related Molecular Network, West China Hospital, Sichuan University, Chengdu, China, 2Mental Health Center, West China Hospital of Sichuan University, Sichuan Clinical Medical Research Center for Mental Disorders, Chengdu, China
Synopsis
Keywords: Functional Connectivity, Brain Connectivity
Motivation: The mechanistic understanding of dysfunctional neural circuits involved in obsessive-compulsive disorder (OCD) is incomplete.
Goal(s): To replicate previous findings in an independent data set and replenish mechanisms of changes in functional connectivity architectures within neurocircuitry of OCD using resting-state fMRI.
Approach: Network-based statistical analysis on a brain network incorporating functionally parcellated regions of interest defined by clustering technique was used.
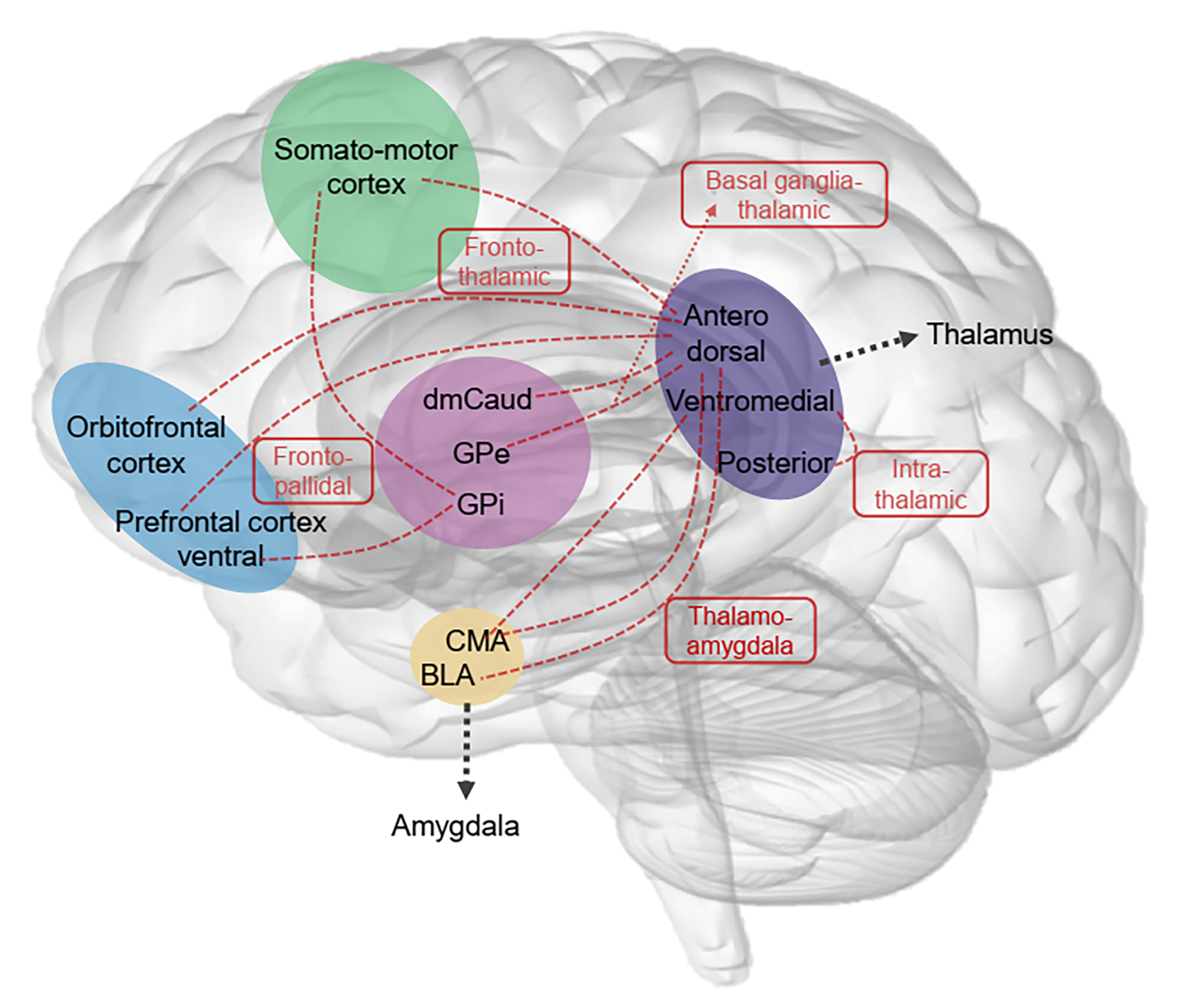
Results: Hyperconnectivity were detected in the fronto-pallidal, fronto-thalamic, basal ganglia-thalamic, intra-thalamic, and thalamo-amygdala connections in OCD patients compared with healthy controls.
Impact: We depict the neurocircuitry model of OCD pathophysiology through the functional network connectivity perspective and extend it by providing the importance of intra-thalamic and thalamo-amygdala connections in OCD. These findings add mechanistic insights to the dysfunctional neural circuits in OCD.
Introduction
The prevailing pathophysiological model of obsessive-compulsive disorder (OCD) has emphasized on the involvement of five parallel, segregated circuits including the sensorimotor, ventral cognitive, dorsal cognitive, ventral affective, and fronto-limbic circuits1,2. Despite substantial efforts to reveal the circuitry mechanism of OCD3, our understanding covers a fragment (i.e. individually altered connections) of the neurocircuitry. Besides, previous investigations define network nodes use a homogeneous, gross structure (i.e. the basal ganglia, thalamus, and amygdala), disregarding the separable functions and connectivity profiles of its distinct subregions. We address this gap by performing network-based statistic (NBS) analysis, an approach has substantially greater power to detect subnetworks of interest, on a brain network incorporating functionally parcellated regions of interest defined by clustering technique in OCD.Methods
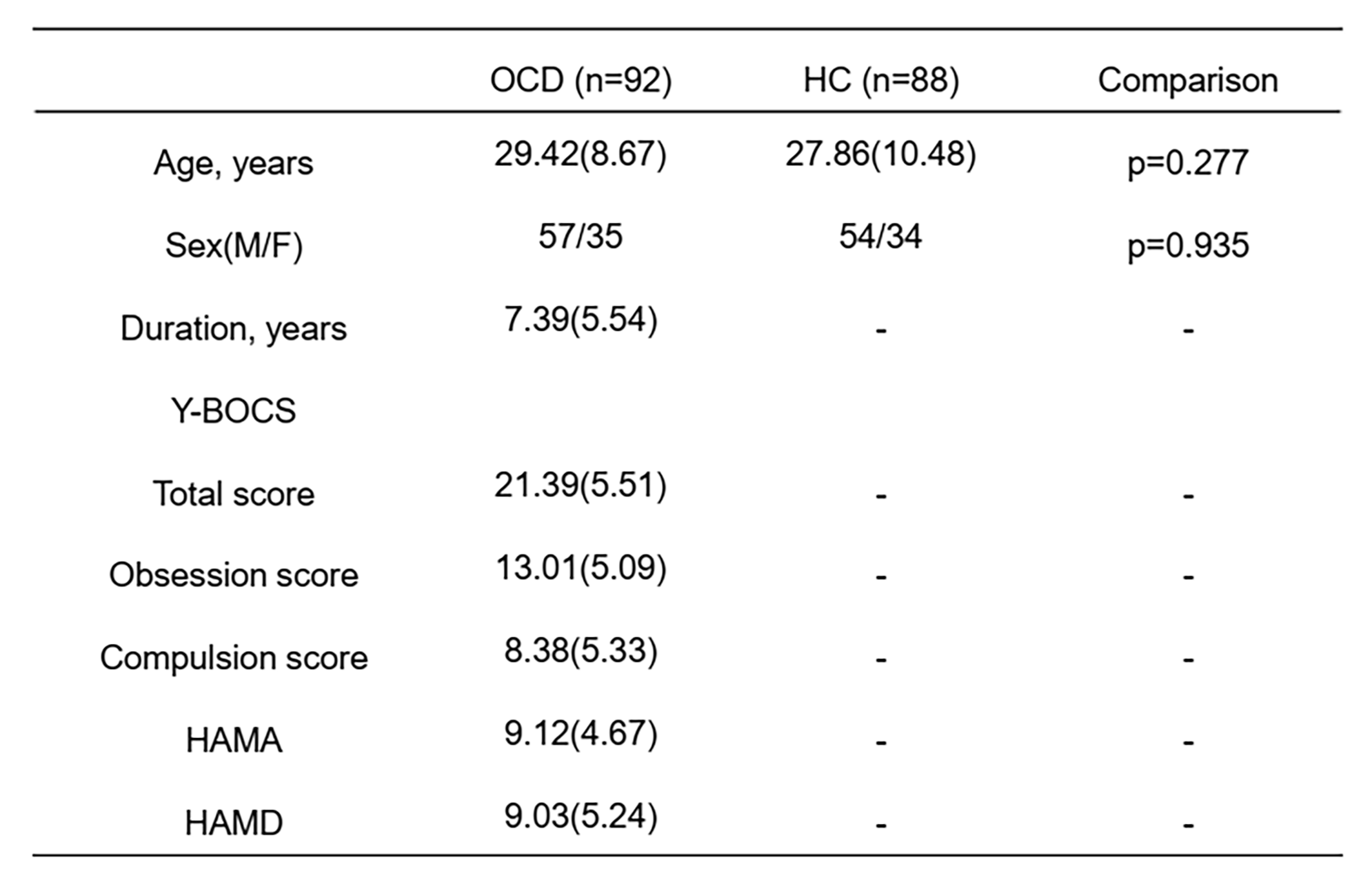
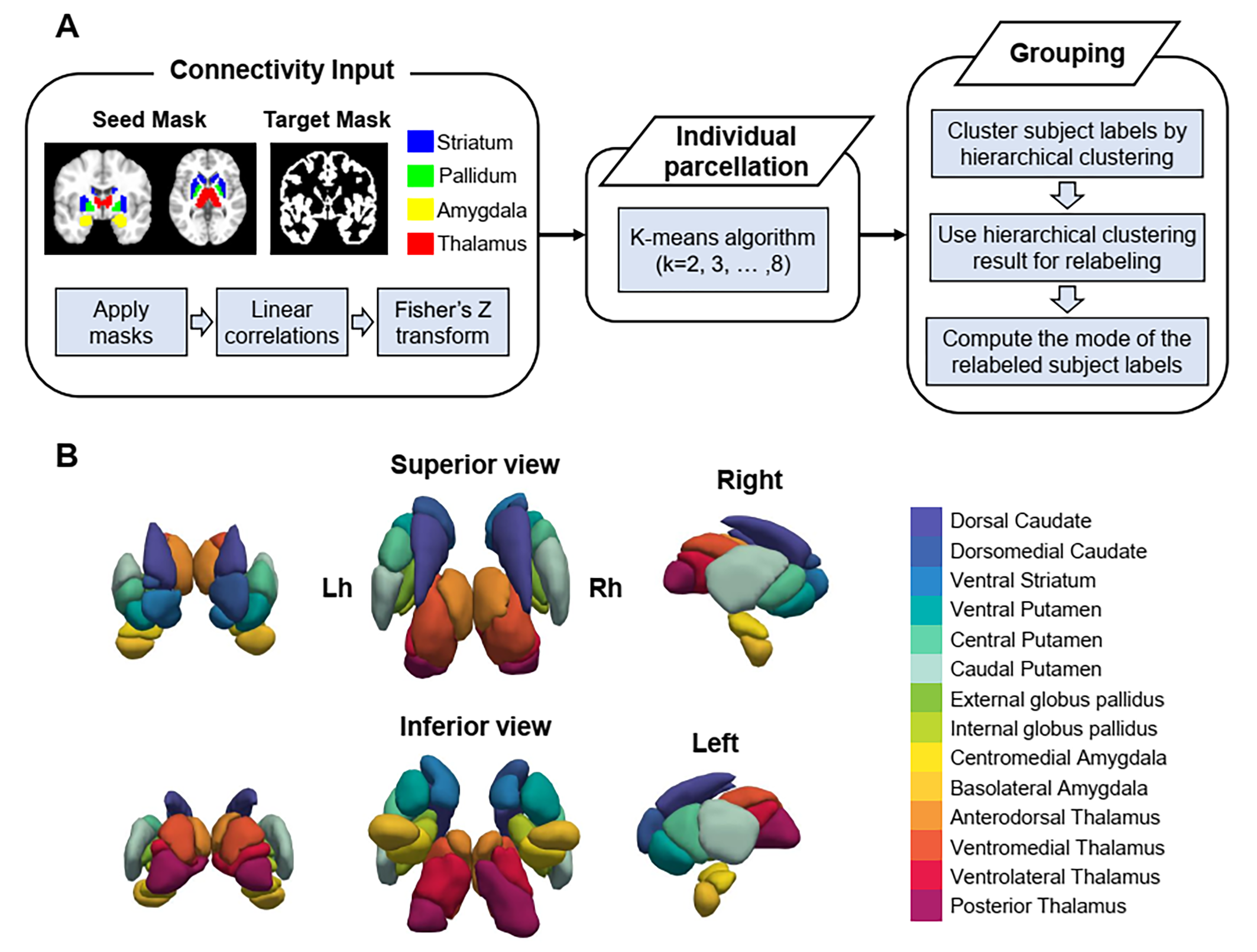
A total of 92 DSM-Ⅳ criteria diagnosed medication-free OCD patients and 88 age- and sex-matched healthy controls (HC) were included in this study after giving written informed consent. All subjects were scanned using 3-Telsa GE MRI to acquire resting-state functional MRI data and high-resolution structural MRI data. We used fMRIPrep version 20.2.1 for anatomical and functional data preprocessing. The post-processing step of fMRIPrep included denoising (ICA-AROMA), covariates removal (WM and CSF signal), smooth (6mm FWHM), and filtering (0.01-0.08Hz).We conducted connectivity-based parcellation4 of the striatum, pallidum, amygdala, and thalamus to define functionally distinct subregions of the main subcortical structures in the neurocircuitry of OCD (Figure 1A). Briefly, we established functional connectivity patterns of voxels in the subcortical regions with whole brain for each subject. Then, we conducted k-means clustering on the connectivity matrix to assign each voxel of subcortical regions to a cluster, effectively grouping similar voxels based on their connectivity profiles and obtaining subject-level parcellations. Finally, the individual clusterings were relabeled and the mode of the relabeled subject-wise clustering was computed and served as the group-level clustering that complemented the high heterogeneity of subject-level clustering to facilitate group comparisons.
Prior to the network analysis, we constructed 46 × 46 connectivity matrix for each subject using Pearson correlation. The nodes consisted of 19 frontal regions generated by matching frontal regions in five nuerocircuitries of OCD described in Shephard et al.2 to the cortical parcels defined by Schaefer atlas and 28 parcellated subregions of the striatum, pallidum, amygdala and thalamus. We utilized NBS approach5 (t>3.1, 5000 permutations, p<0.05), a non-parametric method that controls the family-wise error rate in a mass univariate hypothesis test, to identify altered connectivity patterns within the neurocircuitry of OCD. To explore clinical associations, spearman correlation analyses were conducted between functional connectivity and measures of Y-BOCS, HAMA and HAMD, with age, sex and FD adjusted as covariates.
Results
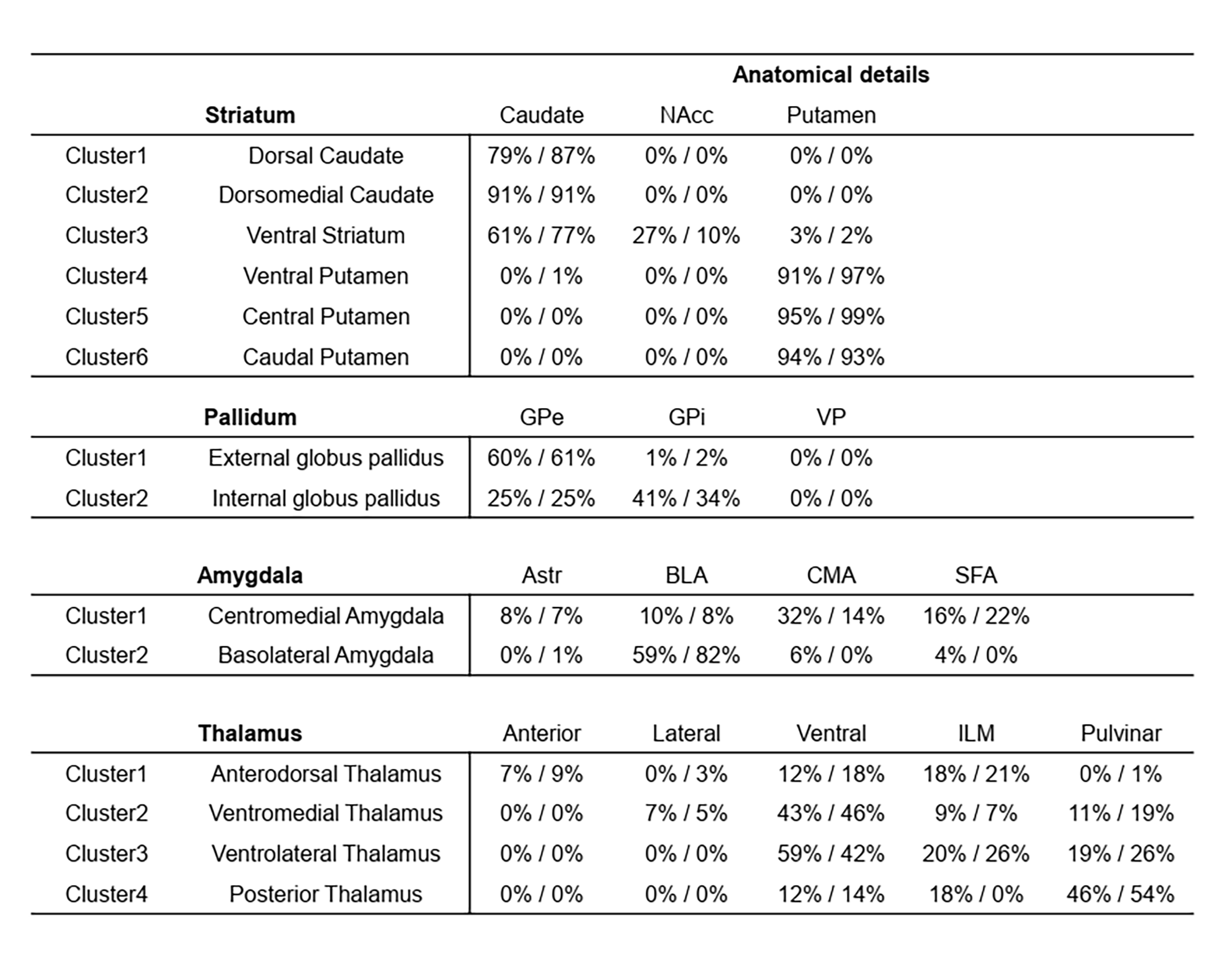
The demographic information and clinical characteristics of the subjects are shown in Table 1.We found that simpler solutions (i.e. fewer clusters) had the higher silhouette value. After consulting prior literatures on subcortical regional functional connectivity and inspecting parcellation results at each solution candidates, we determined each optimal cluster solution at kstriatum=6, kpallidum=2, kamygdala=2, kthalamus=4 (Figure 1B). We provide the anatomical details of each cluster in Table 2.
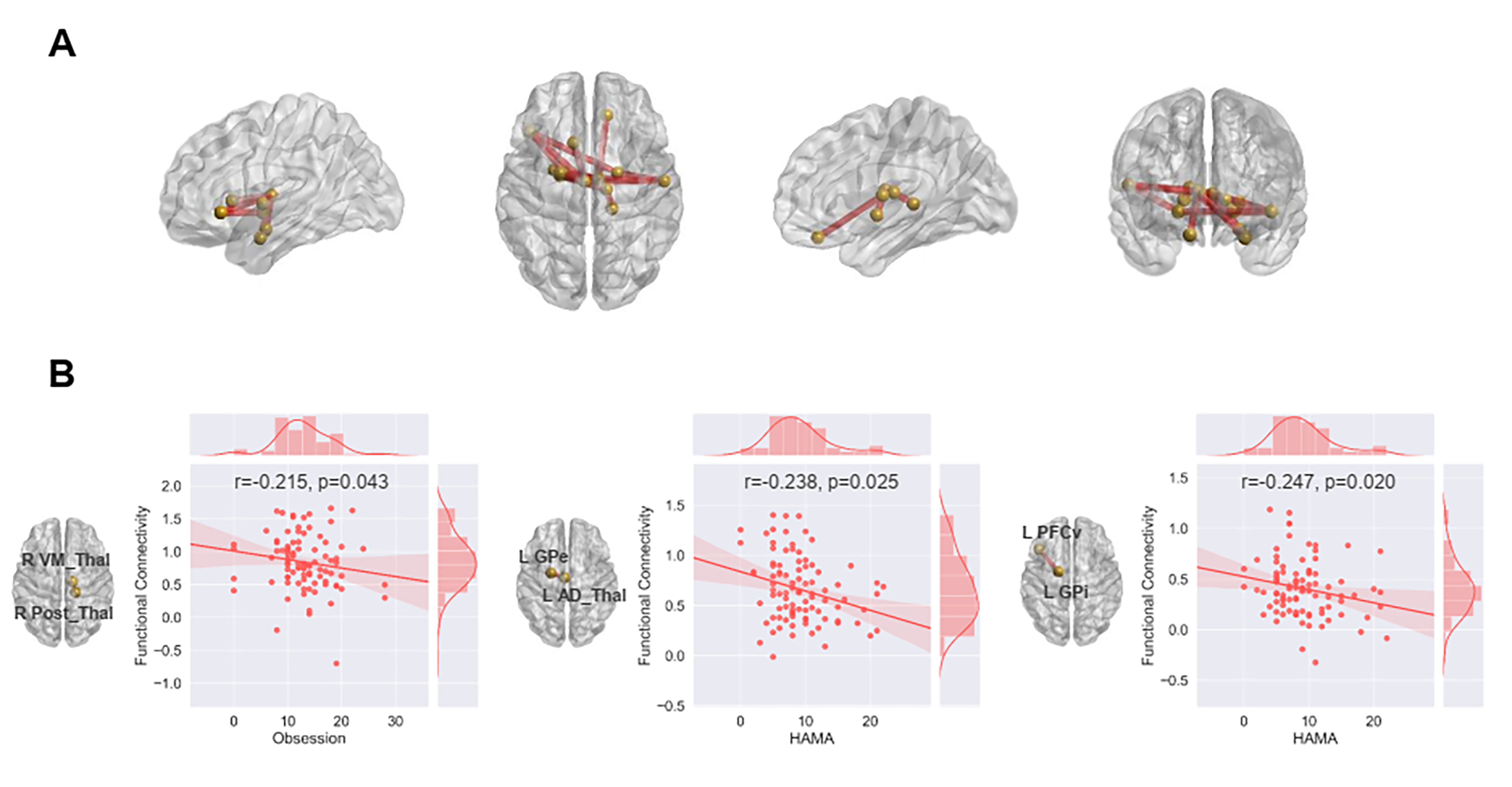
NBS analysis revealed a single connected component with 13 nodes and 16 connections that showed higher functional connectivity in OCD compared with HC (Figure 2A). Heightened connectivities within this single component were composed of fronto-GPi, fronto-thalamic, intra-thalamic, and inter-subcortical connections. Functional connectivities were negatively correlated with measures of Obsession subscale and HAMA within the OCD group (Figure 2B).
Discussion & Conclusion
Using resting-state fMRI network analysis, we identified a network-level pathophysiological profile of OCD (Figure 3). Specifically, we demonstrated hyperconnected fronto-GPi, fronto-thalamic and basal ganglia-thalamic subnetworks in OCD patients, which are in accordance with ventral affective and sensorimotor circuit involved in OCD1,2. Regarding somewhat paradoxical relationship between hyperconnected fronto-GPi and GPe-thalamic subnetworks and less severe anxiety in patients, we supposed that fronto-GPi and GPe-thalamic hyperconnectivity may help control the direct-indirect balance of cortico-striato-thalamo-cortical circuits3 to mediate clinical symptoms. We also found hyperconnected thalamo-amygdala subnetworks affected in OCD in addition to the known neurocircuitry of OCD, verifying a previous animal study that OCD-like behavior is caused by dysfunction of thalamo-amygdala circuits6. Additionally, functionally parcellated subregions enabled us to characterize intra-thalamic hyperconnectivity in OCD patients, which may facilitate transmission of the regulatory signals and further help to regulate obsessive and compulsive symptoms in OCD7. Taken together, these findings depict the neurocircuitry model of OCD pathophysiology through the functional connectivity perspective and extend it by providing the importance of intra-thalamic and thalamo-amygdala connections in OCD.Acknowledgements
This study was supported by National Key R&D Program of China (Grant No. 2022YFF1202400).References
- Stein DJ, Costa DLC, Lochner C, et al. Obsessive-compulsive disorder. Nat Rev Dis Primers. 2019;5(1):52.
- Shephard E, Stern ER, van den Heuvel OA, et al. Toward a neurocircuit-based taxonomy to guide treatment of obsessive-compulsive disorder. Mol Psychiatry. 2021;26(9):4583-4604.
- Goodman WK, Storch EA, Sheth SA. Harmonizing the Neurobiology and Treatment of Obsessive-Compulsive Disorder. Am J Psychiatry. 2021;178(1):17-29.
- Reuter N, Genon S, Kharabian Masouleh S, et al. CBPtools: a Python package for regional connectivity-based parcellation. Brain Struct Funct. 2020;225(4):1261-1275.
- Zalesky A, Fornito A, Bullmore ET. Network-based statistic: identifying differences in brain networks. Neuroimage. 2010;53(4):1197-1207.
- Ullrich M, Weber M, Post AM, et al. OCD-like behavior is caused by dysfunction of thalamo-amygdala circuits and upregulated TrkB/ERK-MAPK signaling as a result of SPRED2 deficiency. Mol Psychiatry. 2018;23(2):444-458.
- Kim T, Kim M, Jung WH, et al. Unbalanced fronto-pallidal neurocircuit underlying set shifting in obsessive-compulsive disorder. Brain. 2022;145(3):979-990.
Figures