1116
Multilevel clinical connectome fingerprinting: uncovering functional connectivity changes across the migraine cycle1ISR-Lisboa/LARSyS and Department of Bioengineering, Instituto Superior Técnico – Universidade de Lisboa, Lisboa, Portugal, 2Learning Health, Hospital da Luz, Lisboa, Portugal, 3Neurology Department, Hospital da Luz, Lisboa, Portugal, 4Center for Interdisciplinary Research in Health, Universidade Católica Portuguesa, Lisboa, Portugal, 5Centro de Estudos Egas Moniz e Instituto de Medicina Molecular João Lobo Antunes, Faculdade de Medicina da Universidade de Lisboa (FMUL), Lisboa, Portugal, 6Basque Center on Cognition, Brain and Language, Donostia, Spain
Synopsis
Keywords: Functional Connectivity, Brain, Migraine, Longitudinal, Multilevel Clinical Connectome Fingerprinting
Motivation: Case-control fMRI studies spanning the entire migraine cycle are lacking, precluding a complete assessment of brain functional connectivity in migraine. Such studies are essential for understanding the inherent changes in the brain of migraine patients as well as transient changes along the cycle.
Goal(s): Our goal was to determine the influence of the migraine cycle on individual functional connectome fingerprints.
Approach: Functional connectivity (FC) was longitudinally studied for migraine patients (across the four different cycle phases) and matched healthy controls.
Results: We observed greater heterogeneity in FC patterns of migraine patients and significant changes in FC across the cycle compared to controls.
Impact: This work represents the first case-control fMRI longitudinal study across the whole migraine cycle. Building upon clinical connectome fingerprinting, applied for the first time to migraine, it tackles a major cause of disability worldwide, contributing to developing connectome-based disease biomarkers.
Introduction
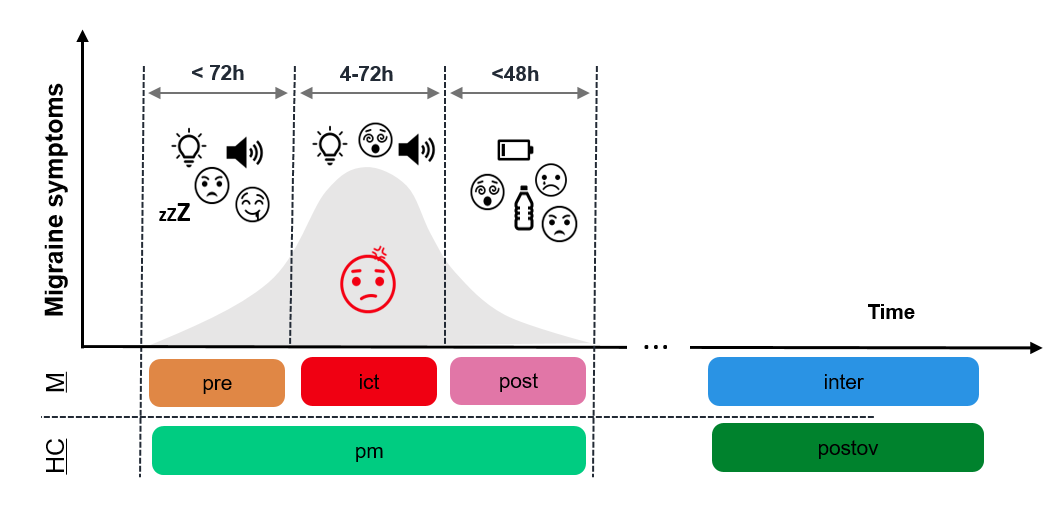
Migraine is a cyclic condition characterized by recurrent headache attacks (ictal phase), accompanied by sensory, and cognitive disruptions, alternated with headache-free periods1. Changes in brain functional connectivity (FC) have been observed in migraine patients, mostly during headache-free periods2. Studying the phases surrounding the attack is more challenging due to logistical hurdles, such as unpredictability and patient discomfort. Consequently, these are not thoroughly investigated despite their critical role in gaining a complete understanding of the migraine cycle.Recently, FC has been shown to provide distinctive fingerprints of individual subjects3. However, connectome fingerprinting in the course of disease is still limited4. Clinical connectome fingerprinting5 has primarily been used in neurodegenerative diseases, typically based on two sessions only6,7,8,9. Here, we adopt a novel multilevel approach to investigate whether the migraine cycle influences individual FC fingerprints, relative to controls, with a complete longitudinal assessment.
Methods
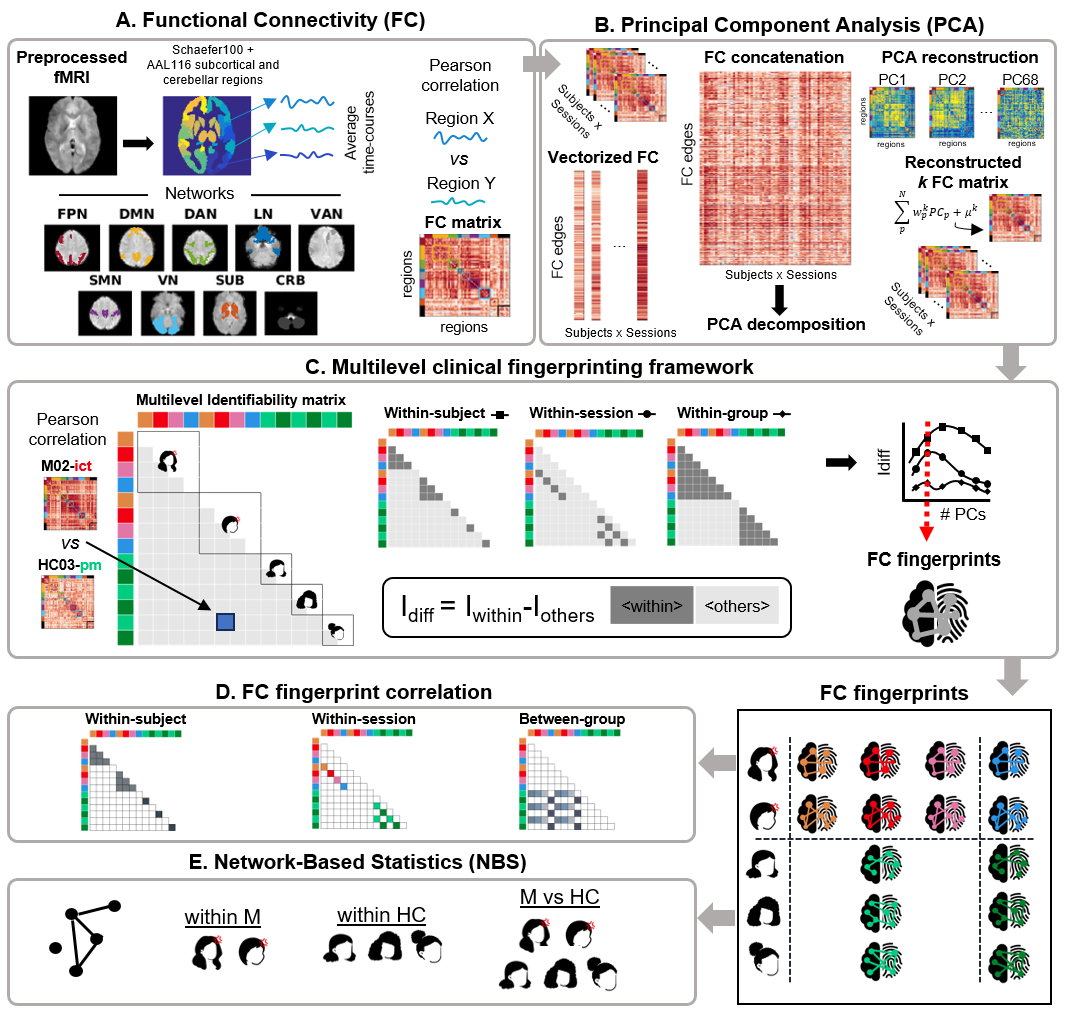
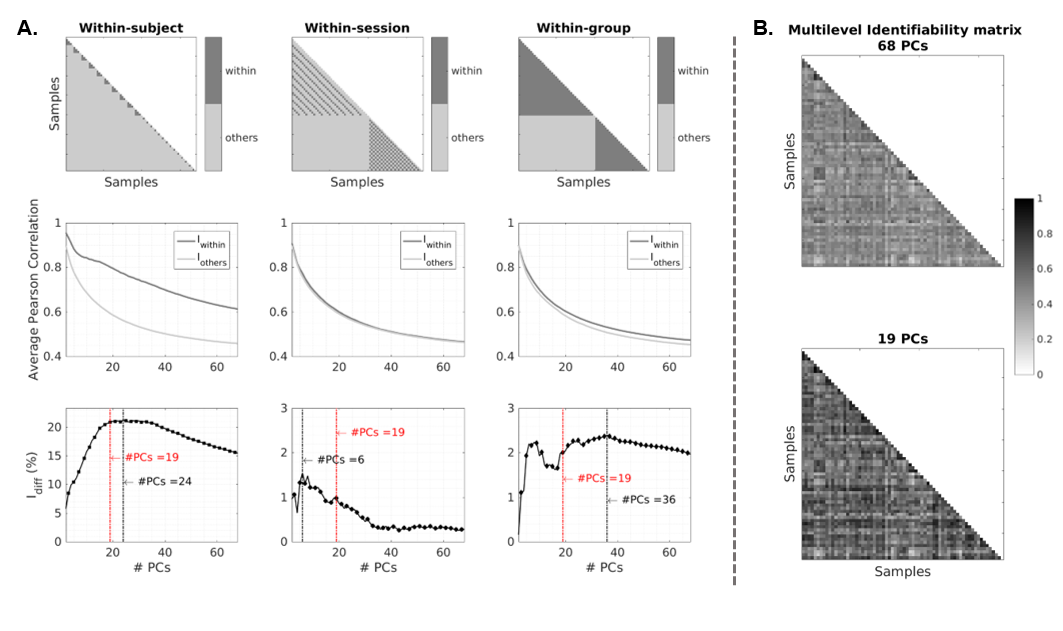
Resting-state fMRI data was acquired from 10 female patients suffering from low-frequency episodic migraine without aura (M), with attacks often linked to the menses, in the 4 phases of the migraine cycle: preictal (M-pre), ictal (M-ict) and postictal (M-post); and interictal (M-inter). We also collected data from 14 matched healthy controls (HC) in two corresponding phases of the menstrual cycle for peri-ictal (perimenstrual, HC-pm) and interictal phases (post-ovulation, HC-postov). Thus, we collected 4 and 2 timepoints for each subject in M and HC (Fig1), respectively, with a total of 68 samples. The fMRI analysis pipeline is represented in Fig2. After preprocessing10 (motion and susceptibility distortion reduction, temporal high-pass filter, regression of motion and physiological confounds and spatial smoothing), we performed a parcellation with the 100-parcels Schaefer atlas (direct correspondence to intrinsic networks11), to which 12 subcortical and 16 cerebellar regions from the AAL116 were added. We used Pearson correlation to compute individual FC matrices and concatenated them across samples, to perform principal component analysis (PCA) reconstruction with a varying number of PCs (2-68). For each reconstruction, a multilevel identifiability matrix was generated, as the correlation between the FC matrices of all pairs of samples.The proposed multilevel clinical connectome fingerprinting approach combines the differential identifiability12 (Idiff) of subjects, sessions and group, to define the number of PCs for dimensionality reduction. For each level, Idiff=Iwithin-Iothers, where Iwithin corresponds to the average correlation among equivalent samples and Iothers among non-equivalent samples (ex. within-session, Iwithin: M-pre sessions of different subjects; Iothers: M-pre and other sessions of the same/different subjects). The higher the Idiff, the more pronounced the FC fingerprint along that specific level. Individual FC fingerprints were obtained for the multilevel-informed selection of PCs. Then, for each subject, we computed the average correlation within-subject (with other sessions of that subject), within-session (with other M in the same session) and between-group (only for M, with HC in the matching session). Finally, Network-Based Statistics (NBS)13 was employed to identify significant variations in FC within-group and between-group.
Results
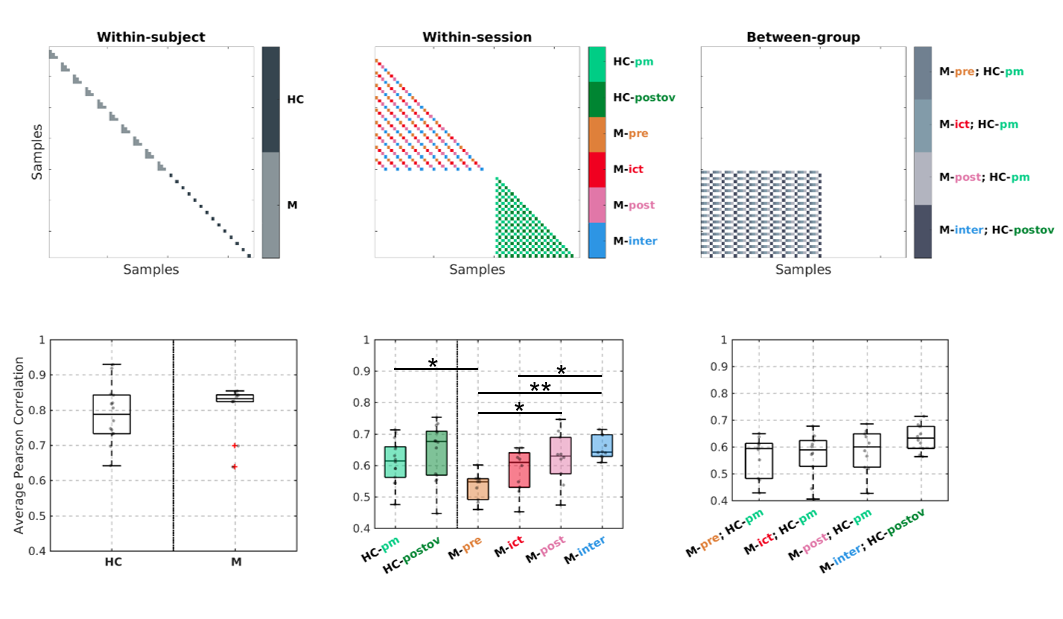
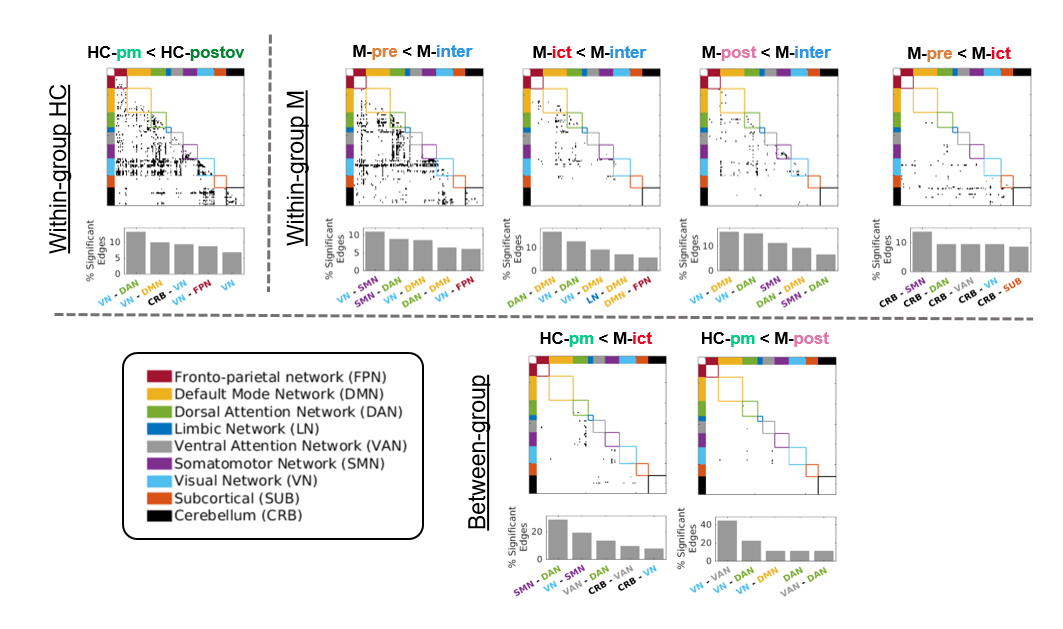
Based on the multilevel Idiff, we selected 19 PCs (80% variance explained) as the best trade-off between Idiff within-subject, -session and -group (Fig3). Comparing the FC fingerprints regarding their correlation (Fig4), within-subject and between-group there are no significant differences. However, within-session, the similarity within M-pre is significantly lower than within M-post and M-inter, as well as HC-pm. For M-ict, it is only lower when compared to M-inter. Regarding the FC analysis with NBS (Fig5), FC is significantly lower in HC-pm compared to HC-postov, but also compared to M-ict and M-post. Across the migraine cycle, all the peri-ictal phases show decreased FC compared to M-inter. Additionally, main alterations occur within and between VN, DAN, DMN and SMN, though the involvement of networks differs across the migraine/menstrual cycles.Discussion
The multilevel fingerprinting approach allowed to capture representative FC fingerprints, by excluding redundant/artifactual information. We observed increased FC heterogeneity in the preictal/ictal phases, which decreased with the progression of the attack. When not experiencing symptoms, patients were more homogeneous, and this homogeneity did not differ from the one presented by controls. Regarding FC, there were differences between HC phases. However, since HC-pm was also decreased compared to M-pre and M-ict, we consider that the peri-ictal phases FC decrease in relation to M-inter cannot solely be attributed to menstrual variations.Conclusions
We found FC fingerprint variations across the migraine cycle that could potentially pave the way for tailoring treatment strategies based on individual patterns. The fingerprinting approach enabled the detection of increased variability among patients, beyond menstrual effects, especially around migraine attacks, when patients also differ more from controls.Acknowledgements
We acknowledge the Portuguese Science Foundation: Grants PD/BD/150356/2019, PTDC/EMD-EMD/29675/2017, LISBOA-01-0145-FEDER-029675 and UIDB/50009/2020References
1. Goadsby, P. J., Holland, P. R., Martins-Oliveira, M., Hoffmann, J., Schankin, C., & Akerman, S. (2017). Pathophysiology of Migraine: A Disorder of Sensory Processing. Physiological Reviews, 97(2), 553–622. https://doi.org/10.1152/physrev.00034.201
2. Schramm, S., Börner, C., Reichert, M., Baum, T., Zimmer, C., Heinen, F., Bonfert, M. V., & Sollmann, N. (2023). Functional magnetic resonance imaging in migraine: A systematic review. Cephalalgia, 43(2), 03331024221128278. https://doi.org/10.1177/033310242211282783.
3. Finn, E. S., Shen, X., Scheinost, D., Rosenberg, M. D., Huang, J., Chun, M. M., Papademetris, X., & Constable, R. T. (2015). Functional connectome fingerprinting: Identifying individuals using patterns of brain connectivity. Nature Neuroscience, 18(11), Article 11. https://doi.org/10.1038/nn.41354.
4. Tepper, Á., Vásquez Núñez, J., Ramirez-Mahaluf, J. P., Aguirre, J. M., Barbagelata, D., Maldonado, E., Díaz Dellarossa, C., Nachar, R., González-Valderrama, A., Undurraga, J., Goñi, J., & Crossley, N. (2023). Intra and inter-individual variability in functional connectomes of patients with First Episode of Psychosis. NeuroImage: Clinical, 38, 103391. https://doi.org/10.1016/j.nicl.2023.1033915.
5. Sorrentino, P., Rucco, R., Lardone, A., Liparoti, M., Troisi Lopez, E., Cavaliere, C., Soricelli, A., Jirsa, V., Sorrentino, G., & Amico, E. (2021). Clinical connectome fingerprints of cognitive decline. NeuroImage, 238, 118253. https://doi.org/10.1016/j.neuroimage.2021.1182536.
6. Svaldi, D. O., Goñi, J., Abbas, K., Amico, E., Clark, D. G., Muralidharan, C., Dzemidzic, M., West, J. D., Risacher, S. L., Saykin, A. J., & Apostolova, L. G. (2021). Optimizing differential identifiability improves connectome predictive modeling of cognitive deficits from functional connectivity in Alzheimer’s disease. Human Brain Mapping, 42(11), 3500–3516. https://doi.org/10.1002/hbm.254487.
7. Troisi Lopez, E., Minino, R., Liparoti, M., Polverino, A., Romano, A., De Micco, R., Lucidi, F., Tessitore, A., Amico, E., Sorrentino, G., Jirsa, V., & Sorrentino, P. (2023). Fading of brain network fingerprint in Parkinson’s disease predicts motor clinical impairment. Human Brain Mapping, 44(3), 1239–1250. https://doi.org/10.1002/hbm.261568.
8. Cipriano, L., Liparoti, M., Lopez, E. T., Sarno, L., Lucidi, F., Sorrentino, P., & Sorrentino, G. (2023). Brain fingerprint changes across the menstrual cycle correlate with emotional state (p. 2023.05.21.23290292). medRxiv. https://doi.org/10.1101/2023.05.21.232902929.
9. Romano, A., Trosi Lopez, E., Liparoti, M., Polverino, A., Minino, R., Trojsi, F., Bonavita, S., Mandolesi, L., Granata, C., Amico, E., Sorrentino, G., & Sorrentino, P. (2022). The progressive loss of brain network fingerprints in Amyotrophic Lateral Sclerosis predicts clinical impairment. NeuroImage: Clinical, 35, 103095. https://doi.org/10.1016/j.nicl.2022.10309510.
10. Jenkinson, M., Beckmann, C. F., Behrens, T. E. J., Woolrich, M. W., & Smith, S. M. (2012). FSL. NeuroImage, 62(2), 782–790. https://doi.org/10.1016/j.neuroimage.2011.09.01511.
11. Thomas Yeo, B. T., Krienen, F. M., Sepulcre, J., Sabuncu, M. R., Lashkari, D., Hollinshead, M., Roffman, J. L., Smoller, J. W., Zöllei, L., Polimeni, J. R., Fischl, B., Liu, H., & Buckner, R. L. (2011). The organization of the human cerebral cortex estimated by intrinsic functional connectivity. Journal of Neurophysiology, 106(3), 1125–1165. https://doi.org/10.1152/jn.00338.201112.
12. Amico, E., & Goñi, J. (2018). The quest for identifiability in human functional connectomes. Scientific Reports, 8(1), Article 1. https://doi.org/10.1038/s41598-018-25089-113.
13. Zalesky, A., Fornito, A., & Bullmore, E. T. (2010). Network-based statistic: Identifying differences in brain networks. NeuroImage, 53(4), 1197–1207. https://doi.org/10.1016/j.neuroimage.2010.06.041
Figures