1112
The Association of Brain Functional Network Segregation with Working Memory and Negative Symptoms in Schizophrenia1Yong Loo Lin School of Medicine, National University of Singapore, Singapore, Singapore, 2Research Division, Institute of Mental Health, Singapore, Singapore, 3Lee Kong Chian School of Medicine, Nanyang Technological University, Singapore, Singapore, 4Neuropsychology and Applied Cognitive Neuroscience Laboratory, CAS Key Laboratory of Mental Health, Institute of Psychology, Beijing, China, 5Department of Psychology, University of Chinese Academy of Sciences, Beijing, China, 6Department of Electrical and Computer Engineering, National University of Singapore, Singapore, Singapore, 7Integrative Sciences and Engineering Programme, National University of Singapore, Singapore, Singapore
Synopsis
Keywords: Functional Connectivity, Brain Connectivity, Schizophrenia, negative symptom, network segregation
Motivation: Empirical findings suggest that negative symptoms of schizophrenia could be improved by cognitive training regime.
Goal(s): This study seeks to (1) understand how brain network architecture supporting task performance may be related to negative symptoms and (2) whether better task performance could be linked to differences in intrinsic functional network architecture.
Approach: Schizophrenia patients underwent resting state and dual-modality N-back task fMRI scans. Network segregation was summarised using the system segregation index for each network.
Results: Functional network segregation during both rest and task was associated with negative symptom severity and task performance.
Impact: The current study highlighted the common ground of altered network segregation between negative symptoms and task performance in schizophrenia and encouraged future study on improving negative symptoms and network communication through cognitive training interventions.
Introduction
Negative symptoms in schizophrenia refer to the diminution or loss of normal behaviours or emotional expressions 1. Despite being crucial for a favourable functional outcome, the mainstay of pharmacological treatment in schizophrenia has limited effect on negative symptoms 2. Empirical findings 3,4 suggested that cognitive training using a dual N-back working memory task might improve both task performance and anhedonia symptoms. However, it remains unclear how the underlying network architecture supporting the task performance was related to negative symptoms. Moreover, it is also unclear whether better task performance could be linked to differences in intrinsic functional network architecture.Methods
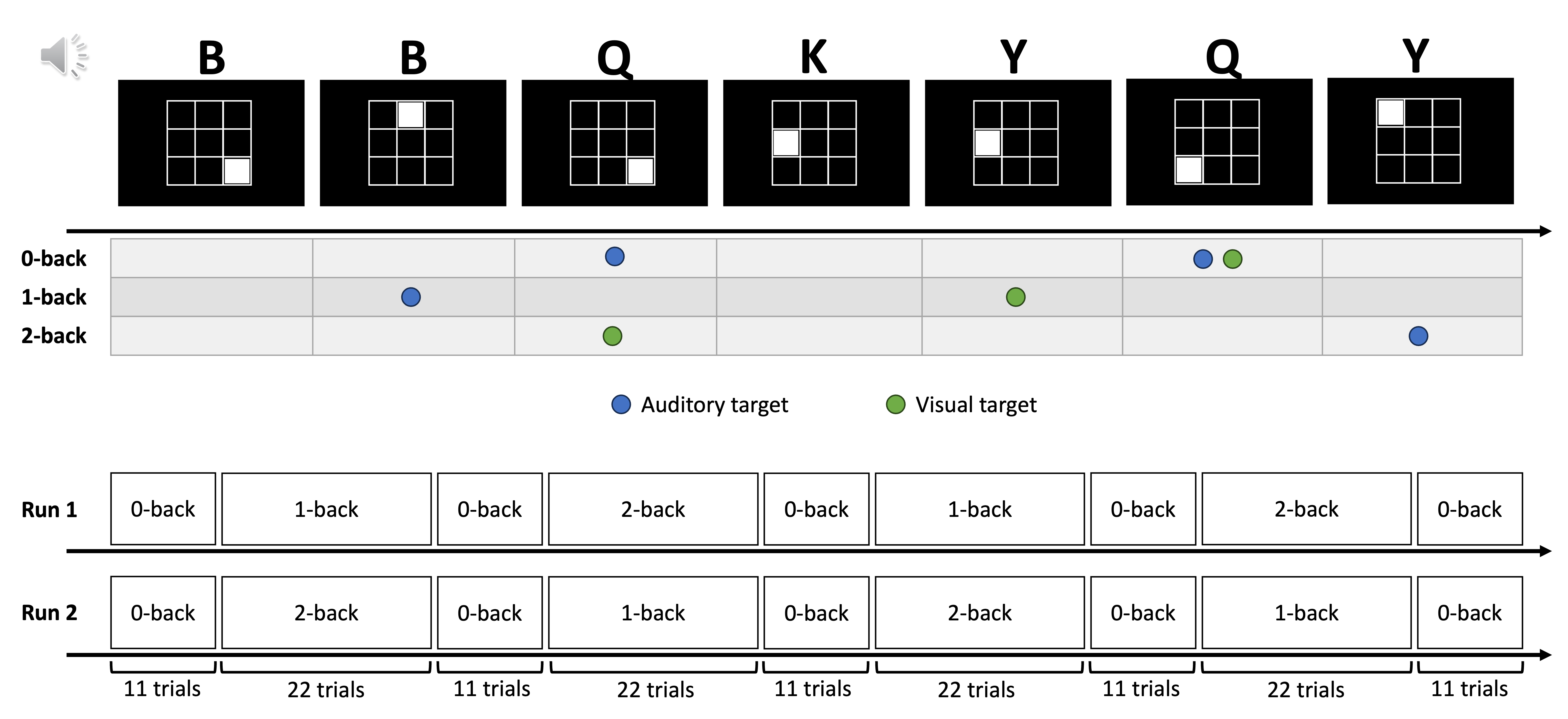
Forty-five schizophrenia patients were recruited from the Institute of Mental Health in Singapore and were identified using the Scale for the Assessment of Negative Symptoms 5 and the Clinical Assessment Interview for Negative Symptoms 6 as showing higher or lower negative symptoms. T1 weighted images (TR/TE/TI=2200/2.45/900ms, 1mm isotropic, FoV=256mm, 192 slices), 10-minute eye-open resting state fMRI and 2 runs of dual-modality n-back task (Figure 1) fMRI (CMRR 7, multiband factor 6, TR/TE=719/30ms, 2.5mm isotropic, FoV=220mm, 60 slices) were acquired at the National University of Singapore (SIEMENS 3T PrismaFit, 32 channel head coil). After quality control, the final sample comprised 41 patients for the resting state (19 higher and 22 lower symptom groups; age mean/SD = 43.99/9.47; 22 males) and 40 patients for the task (16 higher and 24 lower symptom groups; age mean/SD = 44.63/9.32; 24 males) were included. No significant group differences were found in age, sex or education.We constructed whole-brain functional connectivity matrices using 400 Schaefer atlas cortical regions 8 and 30 AAL subcortical regions as nodes before summarizing each matrix into 7 cortical networks 9 and 1 subcortical network. For each patient, one matrix was computed for the resting state and for each task condition. The system segregation index 10 measuring network segregation was calculated for each network. For resting state connectivity, mean relative motion and number of volumes remaining after motion scrubbing were not significantly different between groups. The network-symptom association was tested using linear regression. For the task, we used linear mixed modelling (lmerTest in R) with participants as random effects to test 1) group difference in task performance (d prime), 2) association between network segregation and task performance, and 3) association between task network segregation and negative symptoms. Mean relative motion was higher in the lower symptom group during the task (p=0.036). Mean relative motion during the task was added as a covariate in 2) and 3). For all analyses on the Positive and Negative Syndrome Scale (PANSS) negative symptoms, the PANSS positive symptom score was added as a covariate. False discovery rate (FDR) correction across networks (at threshold q=0.05) was applied.
Results
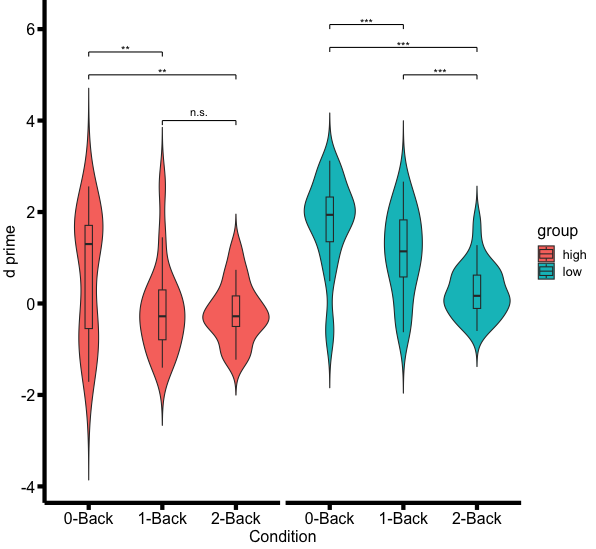
For N-back task performance, the lower symptom group performed better than the higher symptom group (p<0.001). While performance gradually declined in the lower symptom group with increasing difficulty (all p<0.010), performance of the higher symptom group during 1-back declined to a similar level as in the 2-back condition (Figure 2).For the network-performance association, patients with more segregated cognitive (transmodal) networks at rest had better performance in the N-back task (control network, FDR q=0.026; default mode and salience networks, uncorrected p=0.015 and 0.032 respectively). In contrast, patients with more segregated visual (unimodal) network in task tended to perform worse in task (uncorrected p=0.047).
For the network-symptom association, more segregated limbic network at rest was related to higher PANSS negative symptom scores (uncorrected p=0.031). For the task connectivity, PANSS negative symptom scores were associated with more segregated networks in general (p=0.004). Higher PANSS negative symptom scores were related to higher segregation in not only the limbic network (uncorrected p=0.043), but also in the goal-directed network (dorsal attention, FDR q=0.041) and the sensory networks (visual, FDR q=0.039, and somatomotor, uncorrected p=0.028).
Discussion
Our findings suggested that the severity of negative symptoms was associated with higher network segregation, in the limbic network during both at-rest and task-based scanning. The severity of negative symptoms was also related to more segregated networks in general during the task. Moreover, while more segregated cognitive (transmodal) networks at rest may predict better task performance, a more segregated visual (unimodal) network during this dual-modality task was associated with poor performance.Conclusion
These preliminary findings suggest alterations in network communication may underpin both negative symptoms and task performance. These findings also highlight the important role of cognitive training in improving negative symptoms and network communication in schizophrenia patients.Acknowledgements
This study is supported by the LKCMED-NUSMED-NHG Collaborative Mental Health Research Pilot Grant, Singapore. The authors also acknowledge the funding support from the National Research Foundation, Singapore (NRF SOL 2016–002-001) and Yong Loo Lin School of Medicine, National University of Singapore, Singapore.References
1. Administration SA and MHS. Table 3.22, DSM-IV to DSM-5 Schizophrenia Comparison. https://www.ncbi.nlm.nih.gov/books/NBK519704/table/ch3.t22/. Published June 2016. Accessed March 18, 2023.
2. Cerveri G, Gesi C, Mencacci C. Pharmacological treatment of negative symptoms in schizophrenia: update and proposal of a clinical algorithm. Neuropsychiatr Dis Treat. 2019;15:1525-1535. doi:10.2147/NDT.S201726
3. Li X, Xiao YH, Zou LQ, et al. The effects of working memory training on enhancing hedonic processing to affective rewards in individuals with high social anhedonia. Psychiatry Research. 2016;245:482-490. doi:10.1016/j.psychres.2016.09.006
4. Li X, Chu M yi, Lv Q yu, et al. The remediation effects of working memory training in schizophrenia patients with prominent negative symptoms. Cognitive Neuropsychiatry. 2019;24(6):434-453. doi:10.1080/13546805.2019.1674644
5. Andreasen NC. Negative Symptoms in Schizophrenia: Definition and Reliability. Archives of General Psychiatry. 1982;39(7):784-788. doi:10.1001/archpsyc.1982.04290070020005
6. Rekhi G, Ang MS, Yuen CKY, Ng WY, Lee J. Assessing negative symptoms in schizophrenia: Validity of the clinical assessment interview for negative symptoms in Singapore. Schizophrenia Research. 2019;206:177-182. doi:10.1016/j.schres.2018.11.029
7. Auerbach EJ, Xu J, Yacoub E, Moeller S, Uğurbil K. Multi-band accelerated spin-echo echo planar imaging with reduced peak RF power using time-shifted RF pulses. Magn Reson Med. 2013;69(5):1261-1267. doi:10.1002/mrm.24719
8. Schaefer A, Kong R, Gordon EM, et al. Local-Global Parcellation of the Human Cerebral Cortex from Intrinsic Functional Connectivity MRI. Cereb Cortex. 2018;28(9):3095-3114. doi:10.1093/cercor/bhx179
9. Yeo BTT, Krienen FM, Sepulcre J, et al. The organization of the human cerebral cortex estimated by intrinsic functional connectivity. J Neurophysiol. 2011;106(3):1125-1165. doi:10.1152/jn.00338.2011
10. Chan MY, Park DC, Savalia NK, Petersen SE, Wig GS. Decreased segregation of brain systems across the healthy adult lifespan. PNAS. 2014;111(46):E4997-E5006. doi:10.1073/pnas.1415122111
Figures