1110
Functional MRI test-retest reliability during deep brain stimulation in Parkinson’s disease1Radiology and Biomedical Imaging, University of California San Francisco, San Francisco, CA, United States, 2Neurology and Neurological Sciences, Stanford University, Stanford, CA, United States, 3Neurology, University of California San Francisco, San Francisco, CA, United States, 4Neurological Surgery, University of California San Francisco, San Francisco, CA, United States
Synopsis
Keywords: Task/Intervention Based fMRI, fMRI, Deep Brain Stimulation (DBS); Neuromodulation; Reliability; Reproducibility; Test-retest
Motivation: fMRI studies are advancing DBS biomarker development, but data reproducibility is unclear.
Goal(s): To evaluate resting-state fMRI reliability in 16 patients with DBS for Parkinson’s disease.
Approach: fMRI was repeated for DBS-ON and DBS-OFF conditions. Test-retest connectomes were correlated to measure reproducibility and compared across DBS conditions and clinical parameters. Signal reproducibility around the leads was also explored.
Results: Stimulation reduced reproducibility around the leads and across multiple networks, differing by brain target. Patients with less tremor and/or more rigidity and bradykinesia, and relative lower symptom and brain response to DBS had more reproducible functional connectivity.
Impact: The results enhance our understanding of the reliability of resting-state fMRI derivatives in the presence of DBS leads and during stimulation. Realizing the reliability of these data is critical to clinical translation of fMRI-based biomarkers to improve the DBS strategy.
Introduction
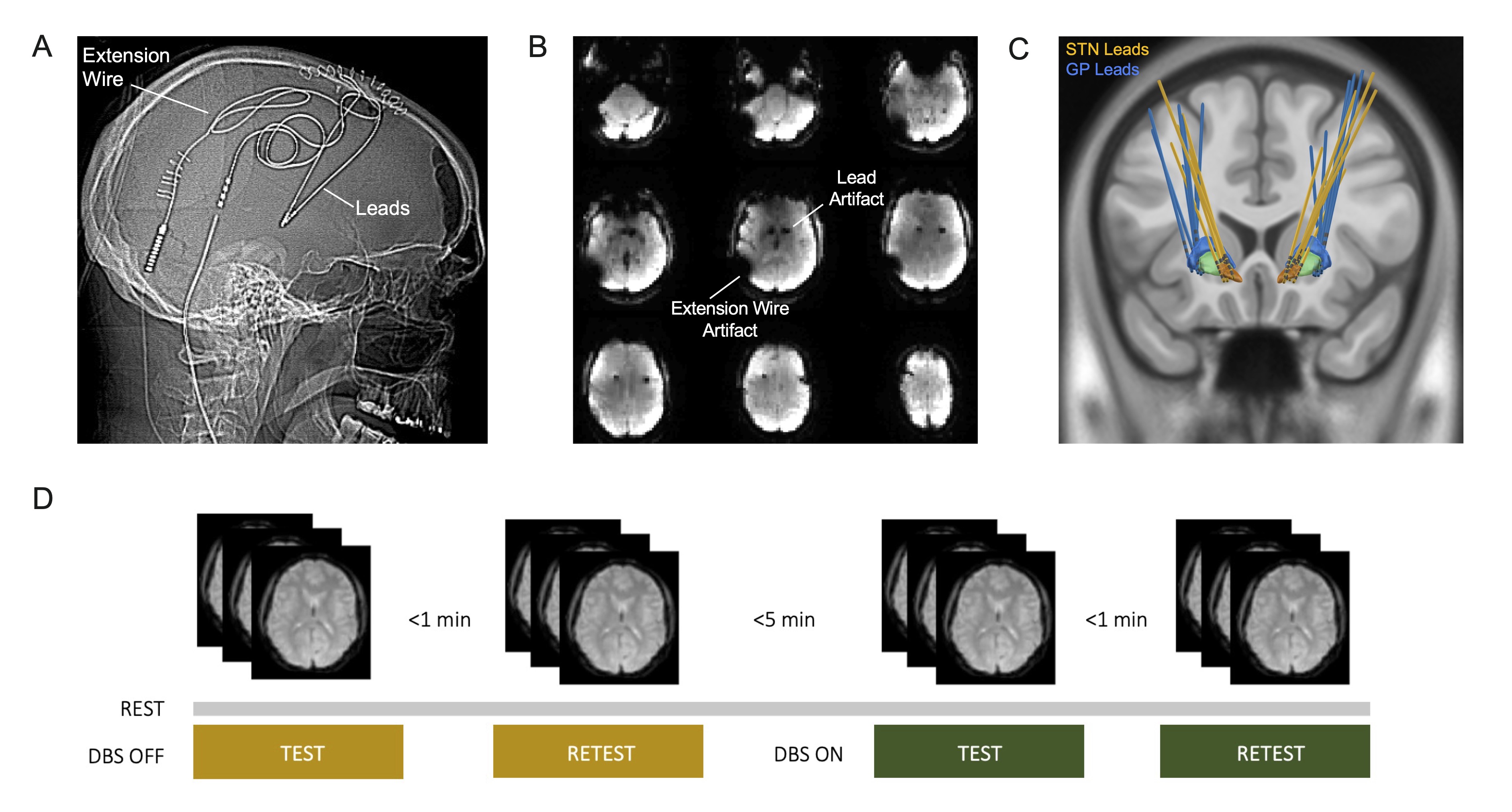
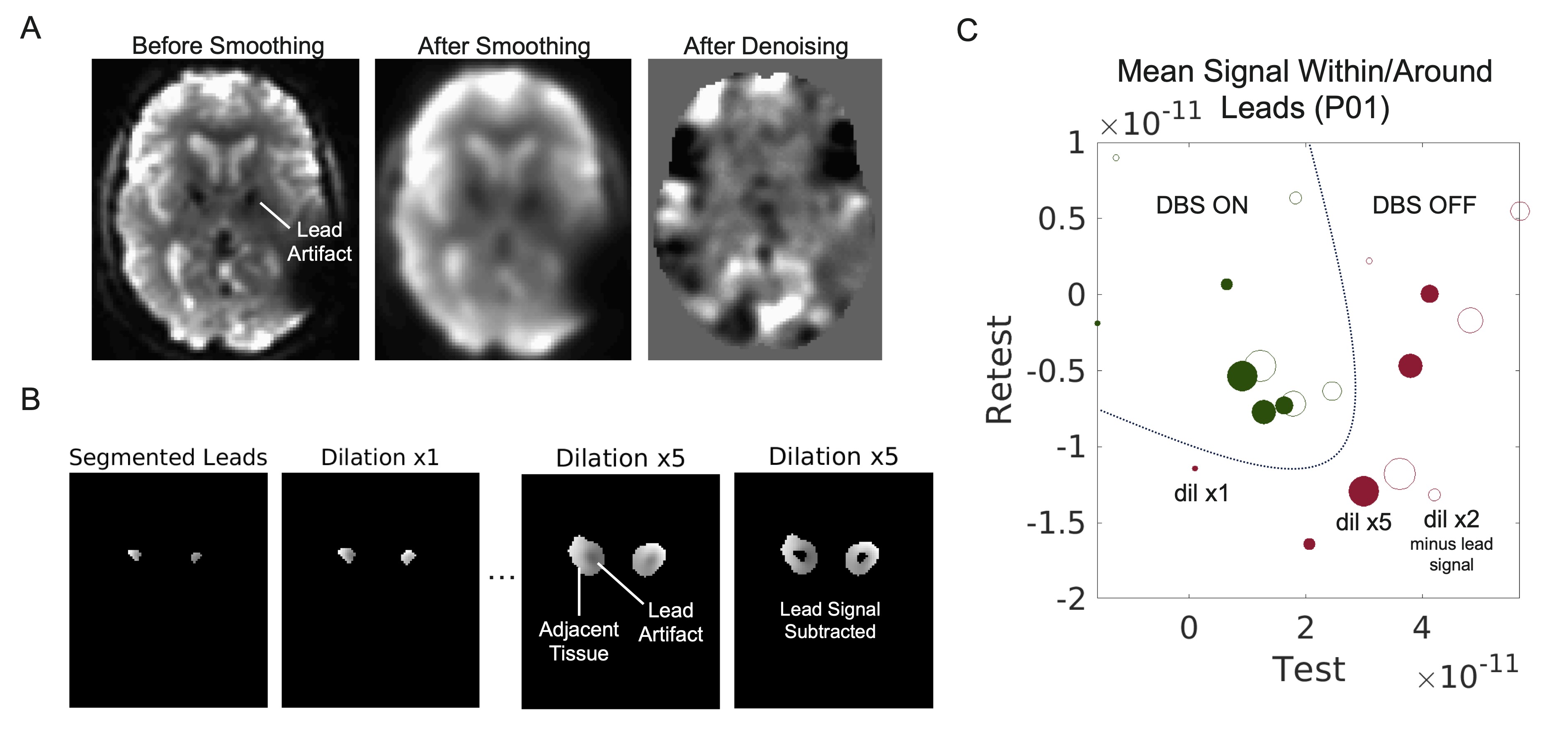
Advances in deep brain stimulation (DBS) hardware now enable patients with certain devices to undergo MRI with stimulation.1 With this, fMRI is emerging as a promising research tool for investigation of stimulation effects on brain networks in relation to clinical response.2 Researchers have begun translating early findings into clinical use cases to predict optimal individualized stimulation settings.3 As the DBS practice continues to grow, successful clinical implementation of much-needed streamlined approaches will depend heavily on their reliability.The validity of fMRI data has long been a focus of research efforts due to concerns about signal reliability in the presence of noise sources.4,5 Implanted DBS leads and wires contribute additional noise sources that degrade fMRI signal contrast. This degradation stems from susceptibility artifacts that increase with field strength, presenting as local signal dropouts and image distortion (Fig 1A-B). Acquisition and preprocessing strategies can improve image quality and likely reliability;6 however, stimulation causes time-varying modulatory effects on brain networks that are not easily predictable.7 The impact of DBS-specific noise sources on the reproducibility of fMRI metrics, is an important unanswered question that holds significant implication for future fMRI-DBS applications. Toward this, we conducted an fMRI test-retest study in patients with DBS for Parkinson’s disease.
Methods
IRB approval was obtained to scan sixteen patients with Parkinson’s disease (agemean=65, female=19%) implanted with a Medtronic Percept PC DBS system in the sub-thalamic nucleus (STN, N=7) or globus pallidus (GP, N=9) 5-66 months prior (Fig 1C). All patients consented to 30-min of scanning including four, 6-min resting-state fMRI scans acquired on a 3T GE system in low-SAR mode with a 32-channel head-coil: two with DBS off, followed by two with DBS on (Fig 1D). Right before scanning, a neurologist programmed patient devices into MR-safe bipolar configurations that best matched monopolar clinical settings. Motor testing was performed in the bipolar research configuration with DBS on, then off, to measure degree of acute symptom improvement. The T1 and gradient-echo fMRI sequences were acquired with the following parameters: TR/TE=2.15s/29ms, voxel size=3.75x3.75x4cm, flip angle=84, and FOV=24cm.Time-series data were preprocessed in CONN using default pipelines.6 In MATLAB we evaluated reproducibility of patient connectomes derived from atlas parcellation across the whole-brain, motor, limbic, and associative networks, as a function of DBS target, clinical parameters, and symptom response. In one patient, we also conducted preliminary investigation of local fMRI signal reproducibility within and around segmented lead profiles.
Results
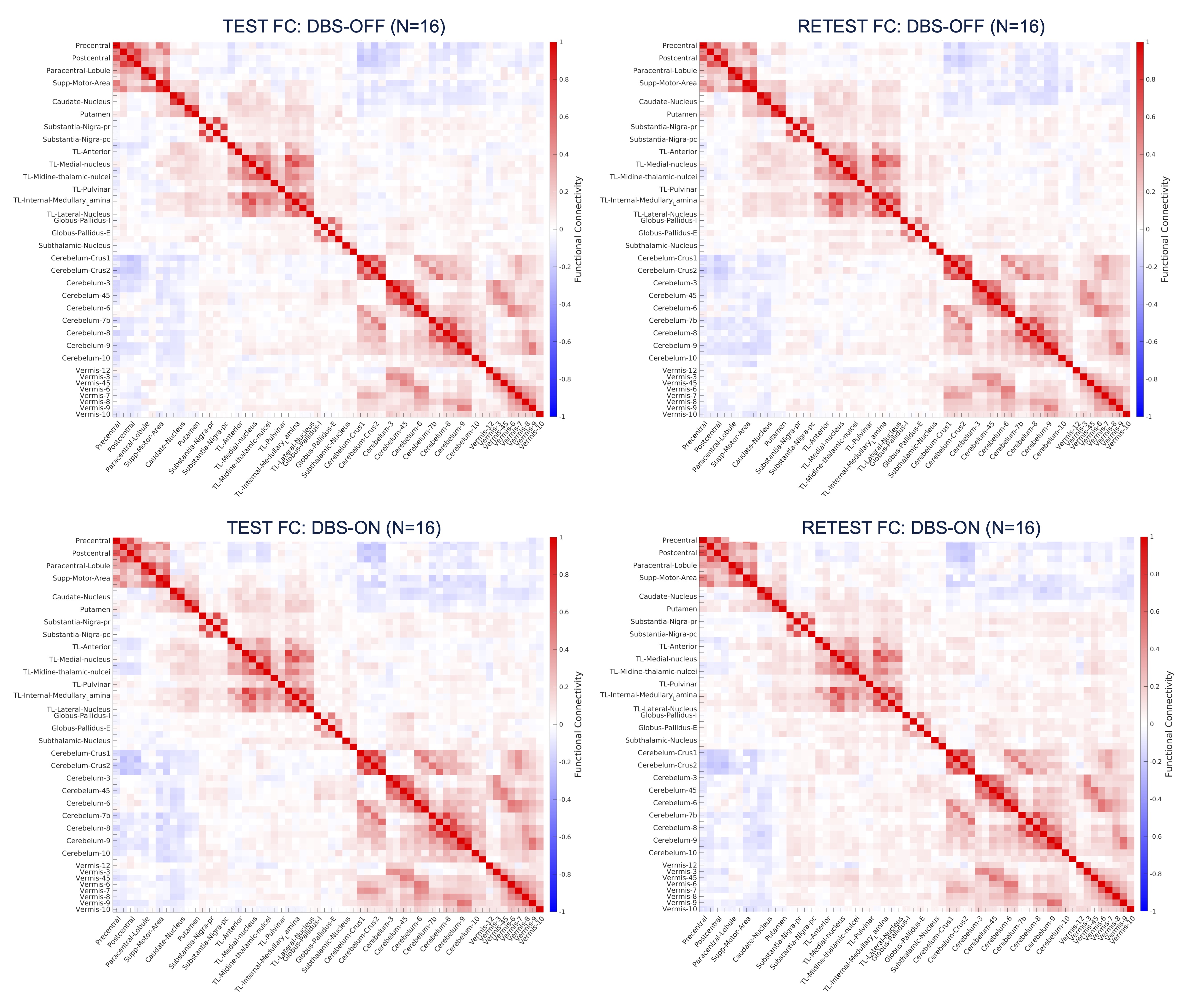
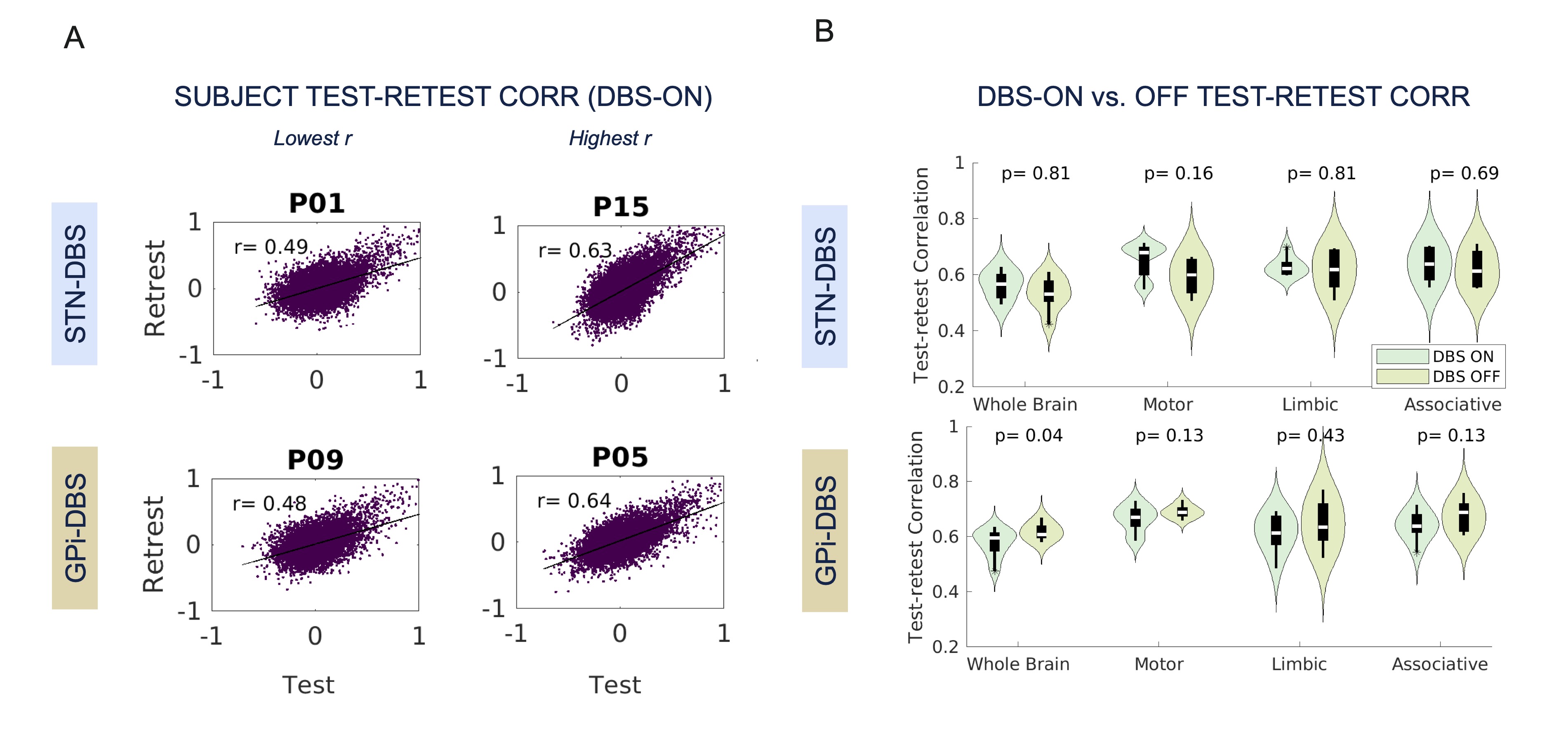
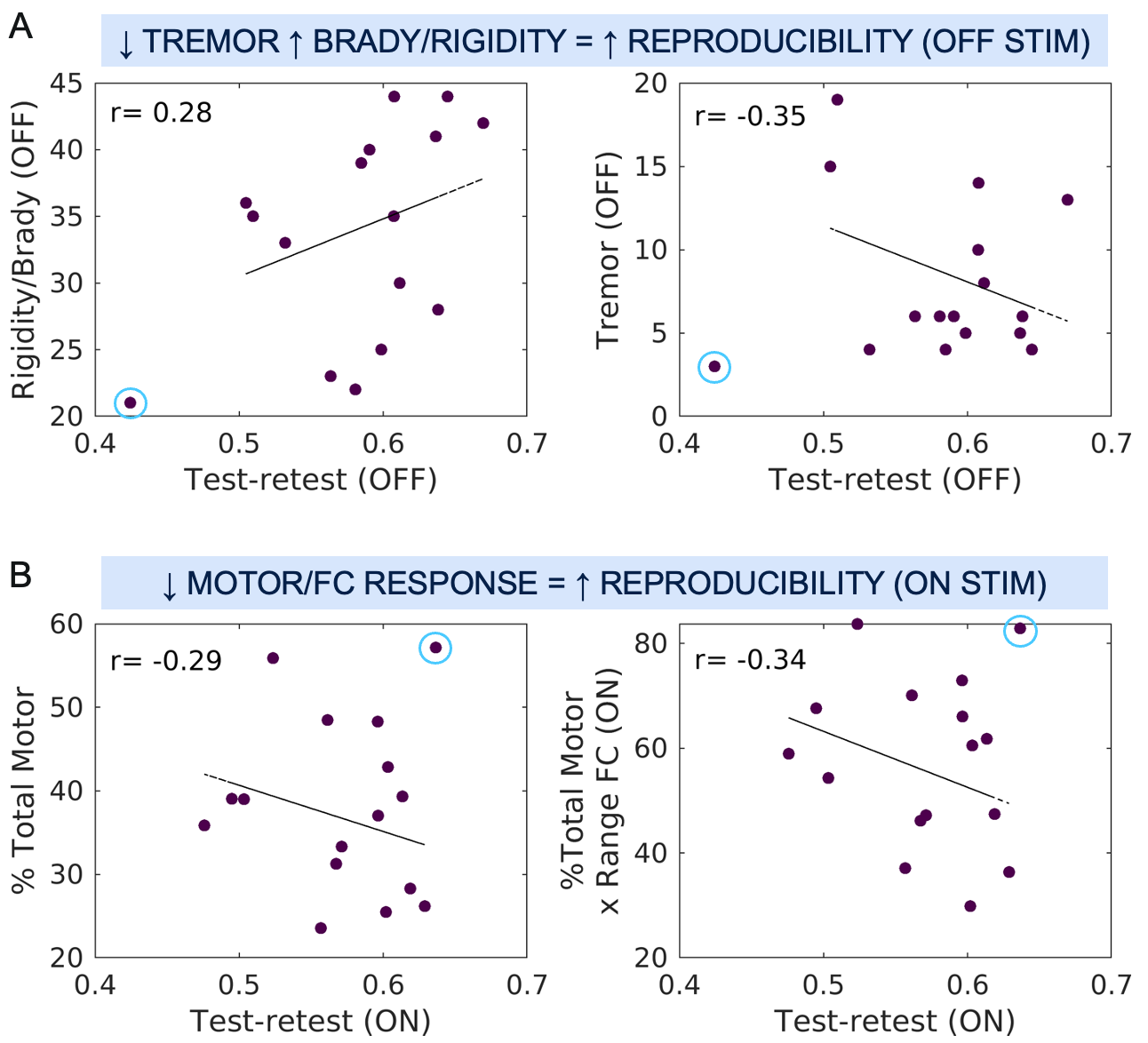
Group-averaged connectomes were visually similar; there were more noticeable differences between DBS-ON/OFF conditions than test-retest pairs (Fig 2). Subject-level correlations between vectorized test and retest connectomes ranged 0.49-0.63 and 0.48-0.64 respectively for data acquired during STN- and GPi-DBS (Fig 3A). When DBS was off, test-retest correlations ranged 0.42-0.67 across all subjects. Contrasting group-averaged test-retest agreement for DBS-ON/OFF conditions revealed opposite target trends whereby STN-DBS increased, and GPi-DBS decreased reproducibility (Fig 3B). This pattern was consistent across networks but only significant for GPi-specific whole-brain connectomes (p<0.05). When removing three outlier patients (2 STN, 1 GPi), GPi-specific trends persisted and there was a reversal of trend observed for STN cases within the limbic and associative networks. Exploration of between-subject sources of variance revealed that patients with: 1) less tremor and/or more rigidity and bradykinesia had more reproducible data when DBS was off and 2) greater symptom and brain response to stimulation had less reproducible data when DBS was on (Fig 4). Averaging the test and retest fMRI signal within and around segmented leads of one patient revealed better local signal reproducibility with STN-DBS off (Fig 5). Interestingly, datapoints corresponding to repeat measurements at increasing volumes centered on (and including or excluding) the leads, were more clustered when DBS was stimulating (Fig 5C).Discussion
Overall, connectome reproducibility in the presence of DBS lead(s) was fair to moderate, within the range of previous investigations in healthy controls.8 Symptoms that lead to more excess movement while DBS is off could be expected to reduce test-retest reliability in the DBS-OFF condition, while active stimulation can have unpredictable time-varying modulatory effects on the brain7 thereby also reducing test-retest reliability but in the DBS-ON condition (Fig 4). Clustering of datapoints in Fig 5C directly demonstrates that stimulation influences the signal of tissue adjacent the leads, likely reflecting local signal synchronicity. Next steps include a more thorough investigation of these patterns across the entire cohort and longitudinal analysis of patients with serial test-retest scans.Conclusion
In patients with DBS implants, preliminary findings show that reliability of resting-state fMRI data is reduced during stimulation and influenced by individual brain response and symptom profiles.Acknowledgements
The authors would like to acknowledge MR staff at the Surbeck Laboratory for advanced imaging, patients, and their caregivers for participating in this study.References
1. Boutet, A. et al. Functional MRI Safety and Artifacts during Deep Brain Stimulation: Experience in 102 Patients. Radiology 293, 174–183 (2019).
2. Loh, A. et al. Probing responses to deep brain stimulation with functional magnetic resonance imaging. Brain Stimulation 15, 683–694 (2022).
3. Boutet, A. et al. Predicting optimal deep brain stimulation parameters for Parkinson’s disease using functional MRI and machine learning. Nat Commun 12, 3043 (2021).
4. Birn, R. M. et al. The Influence of Physiological Noise Correction on Test–Retest Reliability of Resting-State Functional Connectivity. Brain Connectivity 4, 511–522 (2014).
5. Taxali, A., Angstadt, M., Rutherford, S. & Sripada, C. Boost in Test–Retest Reliability in Resting State fMRI with Predictive Modeling. Cerebral Cortex 31, 2822–2833 (2021).
6. In, M.-H. et al. Correction of metal-induced susceptibility artifacts for functional MRI during deep brain stimulation. NeuroImage 158, 26–36 (2017).
7. Sinclair, N. C. et al. Deep brain stimulation for Parkinson’s disease modulates high-frequency evoked and spontaneous neural activity. Neurobiology of Disease 130, 104522 (2019).
8. Tozzi, L., Fleming, S. L., Taylor, Z. D., Raterink, C. D. & Williams, L. M. Test-retest reliability of the human functional connectome over consecutive days: identifying highly reliable portions and assessing the impact of methodological choices. Network Neuroscience 4, 925–945 (2020).
Figures