1099
PET-MR compatible CEST method for imaging of Alzheimer’s Disease.1Biomedical Engineering and Imaging Institute, Icahn School of Medicine at Mount Sinai, New-York, NY, United States, 2Center for Advanced Imaging Innovation and Research (CAI2R), New York University Grossman School of Medicine, New-York, NY, United States, 3Department of Neurology, Massachusetts General Hospital, Harvard Medical School, Boston, MA, United States, 4Department of Neurology, Icahn School of Medicine at Mount Sinai, New-York, NY, United States
Synopsis
Keywords: CEST / APT / NOE, CEST & MT
Motivation: Current methods of assessing Alzheimer's disease, such as PET scans, are expensive, involve exposure to radiation and have limited resolution.
Goal(s): We aim to demonstrate the applicability a novel CEST MRI method to measure the relayed Nuclear Overhauser effect, which may be sensitive to amyloid-β aggregates.
Approach: We have developed and tested a radially sampled CEST sequence (ssGraspCEST) that can be acquired on hybrid PET-MRI systems.
Results: MCI and AD patients appeared to have narrower distributions of LDNOE and ∆ST(-3.6) and higher values. However, due to the limited sample size at this time, no significant differences were observed between the two groups.
Impact: We demonstrated the implementation of a fast, motion-robust CEST method, fully compatible with hybrid PET-MRI systems and particularly suitable for imaging elderly participants who cannot hold still during the scan, which may be useful in future for detecting pathological aggregates.
Introduction
Alzheimer’s disease (AD) is associated with complex pathological processes that begin many years before the onset of clinical symptoms. One of the defining features of AD is the accumulation of abnormal protein aggregates, such as beta-amyloid (Aβ), in the brain. The gradual and chronic build up of these proteins is strongly associated with the progression of AD1. Currently, Aβ burden is typically assessed using radiotracers in positron emission tomography (PET)2. However, the use of PET and PET tracers is costly, entails radiation exposure which limits frequent longitudinal assessments and is of moderate resolution. Addressing these limitations is essential for advancing AD research and improving patient care. We developed a novel steady-state CEST MRI method, fully compatible with the PET-MR scanner, that allows CEST imaging to be acquired during PET sessions. The radially sampled sequence (ssGraspCEST) is particularly suitable for imaging elderly participants who cannot hold still during the scan. We show initial results using the new method to measure the relayed Nuclear Overhauser effect (rNOE), which may be sensitive to pathological aggregates, such as Aβ, in the AD pathology.Methods
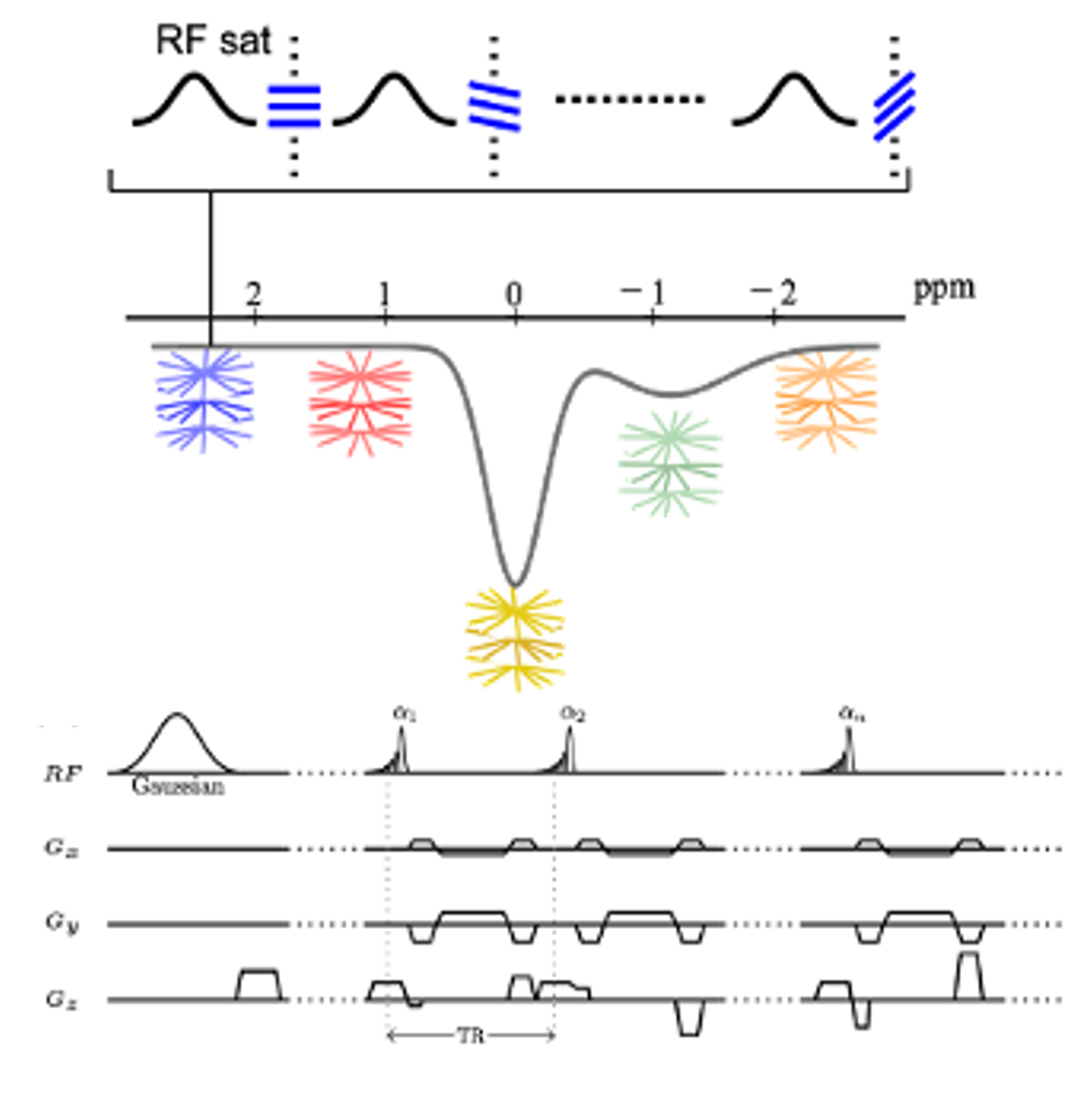
Our CEST sequence (Fig. 1) incorporates steady-state RF saturation with stack-of-stars golden-angle radial sampling3. There is no delay between the acquisitions, ensuring the attainment of a steady-state saturation condition. Acquisition parameters: TR/TE = 3.0/1.12 ms, Flip angle = 5º, slice thickness = 6 mm, 16 slices, FOV = 256x256 mm2, matrix size = 128x128. Gaussian pulses were used for CEST labeling with a B1 = 0.5 µT, duration of 50 ms, followed by a spoiling period (20 mT/m, 5 ms). Images were acquired at 32 saturation frequency offsets between -8.1 to 3.0 ppm, along with two reference images. 100 radial stacks were acquired at each frequency offset, corresponding to a total scan time of 5.5 min.Experiments were performed in 10 cognitively normal, amyloid-negative (HC) adults (9 females, age of 75.2 ± 6.9 yrs.) and in four amyloid-positive adults of whom three had mild cognitive impairment (MCI) (1 female, age 75.7± 7.2 yrs.) and one with AD (male, 74 yrs.).
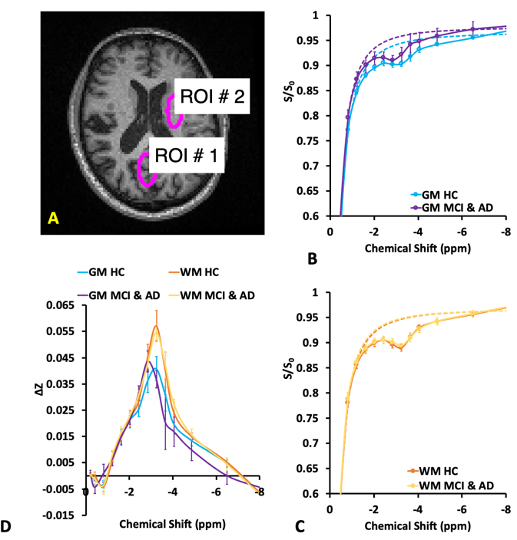
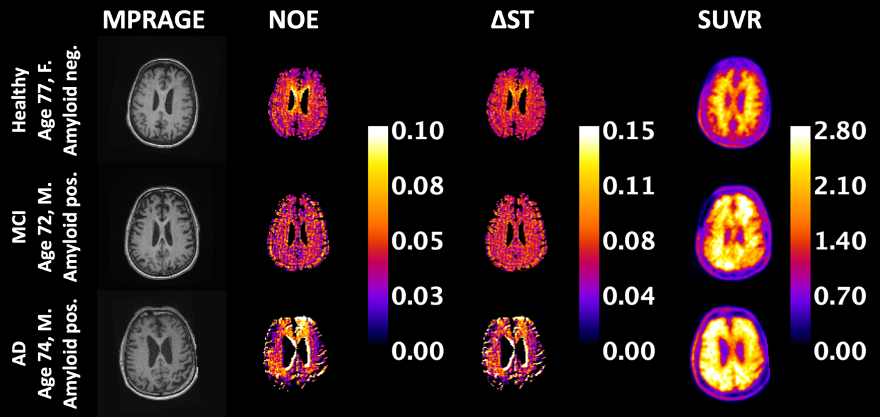
GRASP-Pro technique was performed to reconstruct the dynamic images4. Two ROIs were delineated, representing the white matter (WM) and the gray matter (GM) areas, as shown on Fig. 2A. After B0 correction, a Lorentzian line was fitted to the negative side the z-spectrum (dotted line in Fig. 2B and C) rNOE Lorentzian difference (LDNOE) maps were generated by computing Lorentzian difference between the Lorentzian fitted and the acquired Z-spectra within the range of -3.2 to -3.8 ppm. The ∆ST(-3.6 ppm) maps5 were calculated by taking the relative change between the signal at -8 and -3.6 ppm (Fig. 3).
Amyloid PET was acquired using18F-labeled florbetaben (Neuraceq). The SUVR map was calculated using cerebellum gray matter as reference region. To align the data between the PET and the CEST sessions, both CEST and PET images were co-registered to the anatomical T1 images.
Results and Discussions
Averaged Z-spectra and Lorentzian fitted background between -8.0 and 0 ppm are shown in Fig. 2 B and C for healthy subjects (Aβ-) and MCI and AD patients (Aβ+) in GM and WM regions, respectively. Using the current sequence and parameter combination, 5.5-6% rNOE weighted signal can be observed in the WM and 4-4.5% rNOE signal in the GW.The reasonable contrast allowed us to compute LDNOE and ∆ST maps. Fig. 3. shows T1-weighted, LDNOE, ∆ST(-3.6) and Aβ SUVR maps of representative HC, MCI and AD subjects, respectively. The LDNOE, ∆ST(-3.6) values were calculated from a mask that encompasses cortical regions that typically subject to Aβ deposition6.
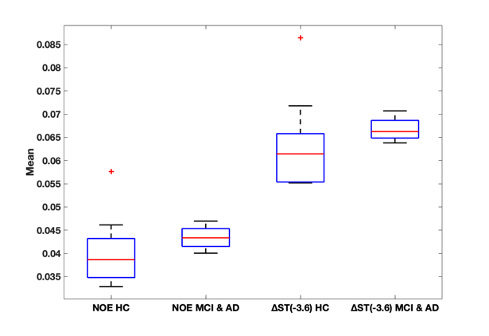
Fig. 4. Shows the comparison of mean NOE, ∆ST(-3.6) between amyloid negative HC and amyloid positive MCI and AD subjects. Compared to healthy controls, the AD/MCI patients appeared to have narrower distributions of LDNOE and ∆ST and a trend for higher values. However, due to the limited sample size at this time, no significant difference was observed between the two groups.
Conclusions
We demonstrated the implementation of a steady-state, radially acquired imaging sequence that is fully compatible to the hybrid PET-MR system. The method can provide excellent rNOE contrast, potentially sensitive to beta-amyloid aggregates. These methods could be used to identify participants with high amyloid burden at risk of MCI/AD from healthy controls, without the need of costly and invasive PET scans. Importantly, given the limited sample size, the study was not powered to detect significant and robust effect sizes. Future work includes increase subject accrual and correlation of the CEST and the PET measurements.Acknowledgements
The study team thank Ms. Sarah Binder and Ms. Nancy Andrew-Jaja for assisting with participant recruitments.
Grant support: R00EB026312
References
1. Tarawneh R, Holtzman DM. The clinical problem of symptomatic Alzheimer disease and mild cognitive impairment. Cold Spring Harbor perspectives in medicine 2012;2(5).
2. Vallabhajosula S. Positron emission tomography radiopharmaceuticals for imaging brain Beta-amyloid. 2011. Elsevier. p 283-299.
3. Ma S, Wang N, Xie Y, Fan Z, Li D, Christodoulou AG. Motion‐robust quantitative multiparametric brain MRI with motion‐resolved MR multitasking. Magnetic resonance in medicine 2022;87(1):102-119.
4. Feng L, Wen Q, Huang C, Tong A, Liu F, Chandarana H. GRASP-Pro: imProving GRASP DCE-MRI through self-calibrating subspace-modeling and contrast phase automation. Magnetic resonance in medicine 2020;83(1):94-108.
5. Chen L, Wei Z, Chan KW, Cai S, Liu G, Lu H, Wong PC, van Zijl PC, Li T, Xu J. Protein aggregation linked to Alzheimer's disease revealed by saturation transfer MRI. Neuroimage 2019;188:380-390.
6. Palmqvist S, Schöll M, Strandberg O, Mattsson N, Stomrud E, Zetterberg H, Blennow K, Landau S, Jagust W, Hansson O. Earliest accumulation of β-amyloid occurs within the default-mode network and concurrently affects brain connectivity. Nature communications 2017;8(1):1214.
Figures