1098
Assessment of neoadjuvant immunochemotherapeutic response for bladder carcinoma using amide proton transfer weighted MRI: a feasibility study1The First Affiliated Hospital, Sun Yat-Sen University, Guangzhou, China
Synopsis
Keywords: CEST / APT / NOE, Bladder
Motivation: To accurately predict bladder cancer patient neoadjuvant treatment responses is essential and urgent.
Goal(s): To investigate the feasibility of amide proton transfer weighted (APTw) and diffusion weighted MRI in evaluating the response of neoadjuvant therapy for bladder cancer.
Approach: Histogram analysis features were extracted from pre- and post-treatment APTw and apparent diffusion coefficient (ADC) map.
Results: Several imaging biomarkers derived from pretreatment imaging were statistical significant between pathological complete response (pCR, no residual tumor) and non-pCR group (P < 0.05 for all). For the pCR group, APTw values markedly decreased while ADC values noticeably increased at post-treatment MRI (P < 0.05 for all).
Impact: This work establishes that APTw MRI holds promise to evaluate bladder cancer tumor responses to neoadjuvant immunochemotherapy and may be used to guide personalized precision therapy in future.
Introduction
At present, only few bladder cancer (BCa) patients would benefit from neoadjuvant immune-chemotherapy while others suffered delay of treatment, chemotherapy- or immunotherapy-related side effects and high economic burden1-3. To accurately predict patient treatment responses is essential and urgent. As a subtype of chemical exchange saturation transfer imaging, amide proton transfer-weighted (APTw) imaging can detect the transfer of magnetization of labeled amide protons located at a chemical shift of 3.5 ppm4, which mainly were reported in clinical utilities for cancer assessment, including diagnosis, staging, and treatment response monitoring, in several malignancies5-8. To the best of our knowledge, the clinical utility of amide proton transfer weighted (APTw) MRI in evaluating tumor response in BCa has not yet been reported. Therefore, we hypothesized that noninvasive imaging biomarkers derived from pre- and post-treatment APTw and diffusion weighted MRI would be useful indicators of BCa patient outcomes.Methods
Participants with pathologically confirmed BCa were prospectively recruited to undergo MRI examination, including APTw MRI, before and after neoadjuvant treatment. Neoadjuvant therapy was a combination of platinum-based chemotherapy and immune checkpoint blockade of the programmed death 1 receptor. Two radiologists performed the measurements of pre- and post-treatment APTw and apparent diffusion coefficient (ADC) values, respectively. Histogram analysis features were also extracted. Participants were categorized into pCR (pathological complete response, no residual tumor) and non-pCR groups based on histologic evaluation of posttreatment cystectomy specimens. The diagnostic efficacy of parameters in predicting tumor responsiveness was evaluated by calculating the area under ROC curve (AUC).Results
A total of 47 participants were enrolled (mean age, 63 ± 9 [SD] years; 38 were men) and 20 participants achieved pCR. Significant differences were found in several imaging biomarkers derived from pretreatment APTw and diffusion weighted MRI (P < 0.05 for all). The baseline APTw mean yielded the highest diagnostic performance (AUC: 0.88-0.90) for evaluating tumor responsiveness. For the pCR group, APTw values markedly decreased while ADC values noticeably increased at post-treatment MRI (P < 0.05 for all).Discussion
APTw imaging has been proved to be a valuable metabolic MRI technique. Contrast is due to exchangeable backbone amide protons of endogenous mobile macromolecules, such as proteins and peptides, as well as tissue pH4,6,7. In this study, we found noticeably higher APTw values and significantly lower ADC values in pCR groups. High APTw values may represent high protein concentrations, high cell density, and high proliferative activity, which are more sensitive to immunochemotherapy and result in better patient outcomes9,10. Furthermore, APTw values are positively related to pH, which indirectly reflects tumor perfusion and the degree of hypoxia within the tumor microenvironment9,11. Better-perfused tumors not only have higher proliferative capacity, but also provide better chemotherapy access and less hypoxia-mediated resistance. In addition, blood flow generates sufficient chemical exchange saturation transfer (CEST) contrast12,13. Therefore, all of these factors may contribute to higher APTw values in pCR groups.To comprehensively interpret the tumor microenvironment, histogram analysis was also used. Our results showed that multiple APTw and diffusion weighted histogram parameters were associated with tumor response in addition that the AUC of APTw values (corresponding to the mean and median of APTw values, respectively) were significantly higher than the AUC of ADC values, indicating that APTw MRI may be a more promising application for clinical practice. Entropy was considered to measure the randomness and homogeneity of the distribution of quantitative parameters and reflect tumor heterogeneity, which is reported to be a key factor that influences the immunochemotherapeutic effect14,15. Consistent with previous study reported16, our study also found that more homogenous tumors were good responders. This might be explained that tumor with increased entropy values represents a greater tumor heterogeneity and more aggressive biology with more differences in angiogenesis and proteosynthesis within proliferating tumor cells and resistant to neoadjuvant therapy.
The data in our study have also indicated noticeable increases in ADC values and decreases in APTw values were correlated with better treatment response and survival outcome. Possible explanations include a decreasing cellular density and metabolic rate when there was no residual tumor, and treatment-related effect, such as necrosis, fibrosis and oedema et al. Meanwhile, both ADC and APTw entropy increased aftertreatment. The infiltration of effector immune cells in the stromal tissue triggered by immunochemotherapy is considered as one potential cause.
Conclusion
MRI parametrics derived from APTw and diffusion weighted MRI can both serve as valuable non-invasive imaging biomarkers for evaluating the efficacy of neoadjuvant therapy. Moreover, the molecular imaging technique of APTw MRI was superior to DWI for tumor response prediction, which needs further validation by future research.Acknowledgements
NoneReferences
1. Hu J, Chen J, Ou Z, Chen H, Liu Z, Chen M, et al. Neoadjuvant immunotherapy, chemotherapy, and combination therapy in muscle-invasive bladder cancer: A multi-center real-world retrospective study. Cell Rep Med 2022;3:100785.
2.Funt SA, Lattanzi M, Whiting K, Al-Ahmadie H, Quinlan C, Teo MY, et al. Neoadjuvant Atezolizumab With Gemcitabine and Cisplatin in Patients With Muscle-Invasive Bladder Cancer: A Multicenter, Single-Arm, Phase II Trial. J Clin Oncol 2022;40:1312-1322.
3.Rose TL, Harrison MR, Deal AM, Ramalingam S, Whang YE, Brower B, et al. Phase II Study of Gemcitabine and Split-Dose Cisplatin Plus Pembrolizumab as Neoadjuvant Therapy Before Radical Cystectomy in Patients With Muscle-Invasive Bladder Cancer. J Clin Oncol 2021;39:3140-3148.
4. Zhou J, Lal B, Wilson DA, Laterra J, van Zijl PC. Amide proton transfer (APT) contrast for imaging of brain tumors. Magn Reson Med. 2003;50(6):1120-1126.
5. Wang HJ, Cai Q, Huang YP, et al. Amide Proton Transfer-weighted MRI in Predicting Histologic Grade of Bladder Cancer. Radiology. 2022:211804.
6. Park JE, Kim HS, Park KJ, Choi CG, Kim SJ. Histogram Analysis of Amide Proton Transfer Imaging to Identify Contrast-enhancing Low-Grade Brain Tumor That Mimics High-Grade Tumor: Increased Accuracy of MR Perfusion. Radiology. 2015;277(1):151-161.
7. Guo Z, Qin X, Mu R, et al. Amide Proton Transfer Could Provide More Accurate Lesion Characterization in the Transition Zone of the Prostate. J Magn Reson Imaging. 2022;56(5):1311-1319.
8. Meng N, Fu F, Feng P, et al. Evaluation of Amide Proton Transfer-Weighted Imaging for Lung Cancer Subtype and Epidermal Growth Factor Receptor: A Comparative Study With Diffusion and Metabolic Parameters. J Magn Reson Imaging. 2022;56(4):1118-1129.
9.Zhou JY, Payen JF, Wilson DA, Traystman RJ, van Zijl PCM. Using the amide proton signals of intracellular proteins and peptides to detect pH effects in MRI. Nature Medicine 2003;9:1085-1090. 10.Adams J. The proteasome: a suitable antineoplastic target. Nat Rev Cancer 2004;4:349-360.
11. Ray KJ, Simard MA, Larkin JR, Coates J, Kinchesh P, Smart SC, et al. Tumor pH and Protein Concentration Contribute to the Signal of Amide Proton Transfer Magnetic Resonance Imaging. Cancer Res 2019;79:1343-1352.
12.Chen W, Mao L, Li L, Wei Q, Hu S, Ye Y, et al. Predicting Treatment Response of Neoadjuvant Chemoradiotherapy in Locally Advanced Rectal Cancer Using Amide Proton Transfer MRI Combined With Diffusion-Weighted Imaging. Front Oncol 2021;11:698427.
13.Zheng S, van der Bom IM, Zu Z, Lin G, Zhao Y, Gounis MJ. Chemical exchange saturation transfer effect in blood. Magn Reson Med 2014;71:1082-1092.
14.De Robertis R, Maris B, Cardobi N, Tinazzi Martini P, Gobbo S, Capelli P, et al. Can histogram analysis of MR images predict aggressiveness in pancreatic neuroendocrine tumors? Eur Radiol 2018;28:2582-2591.
15.Just N. Improving tumour heterogeneity MRI assessment with histograms. Br J Cancer 2014;111:2205-2213.
16.Perucho JAU, Wang M, Tse KY, Ip PPC, Siu SWK, Ngan HYS, et al. Association between MRI histogram features and treatment response in locally advanced cervical cancer treated by chemoradiotherapy. Eur Radiol 2021;31:1727-1735.
Figures
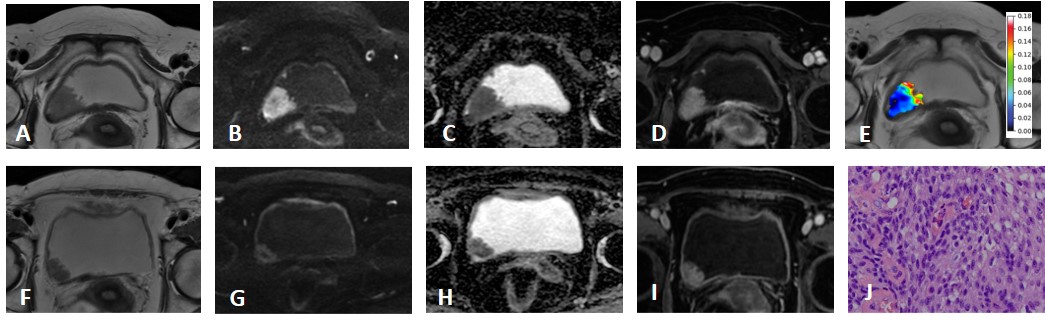
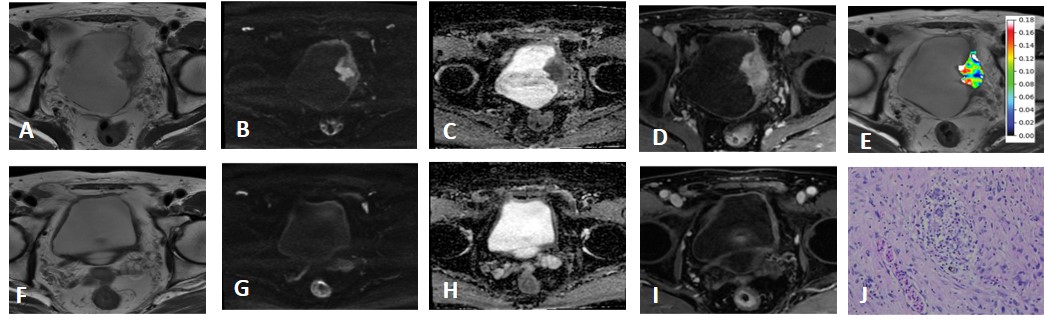
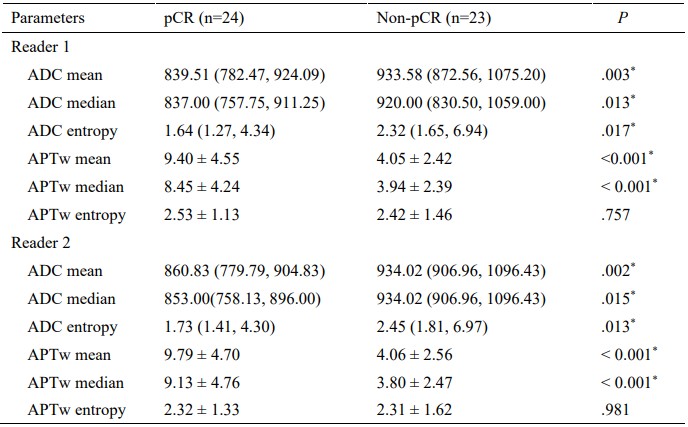
Table 1: Comparison of baseline histogram features between pCR and non-pCR participants with bladder cancer.
Data following the normal distribution are expressed as the mean ± standard deviation; other data are expressed as the median (first quartile and third quartile). P values for differences were determined by the independent sample Student’s t-test or the Mann-Whitney U test. * Statistically significant differences (P < 0.05).
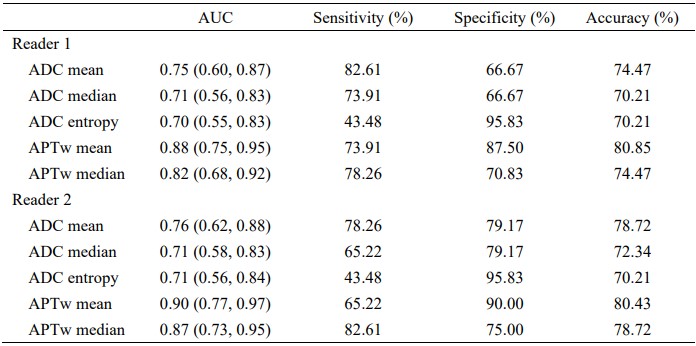
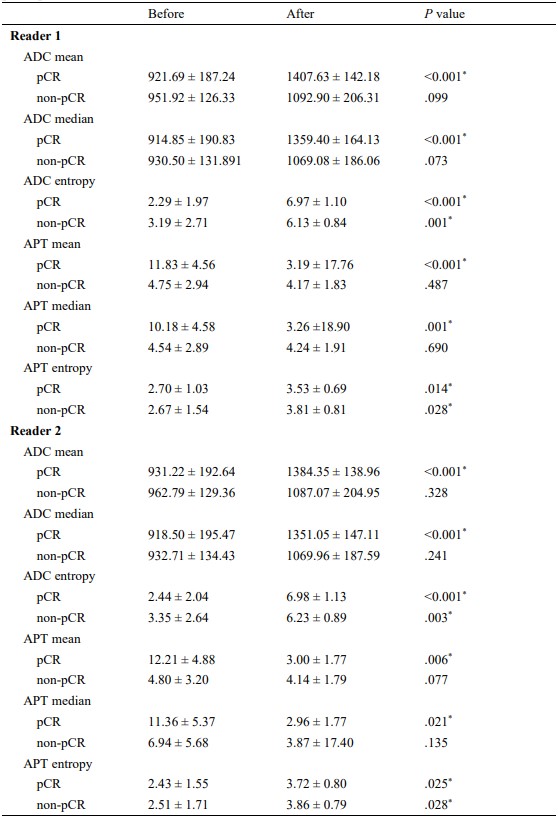
Table 3: Comparison of pre- and post-treatment histogram features between pCR and non-pCR participants with bladder cancer.
Data following the normal distribution are expressed as the mean ± standard deviation. P values for differences were determined by the paired t-test or the Wilcoxon matched-pairs signed rank test. * Statistically significant differences (P < 0.05).