1080
Proximal Gradient Decent Network for Respiratory-Correlated Four-Dimensional Abdominal MR Fingerprinting Reconstruction (PGDN-RC-4DMRF)1The Hong Kong Polytechnic University, Hong Kong, China, 2The University of Hong Kong, Hong Kong, China
Synopsis
Keywords: MR Fingerprinting, Radiotherapy
Motivation: Four-dimensional MR fingerprinting (4D-MRF) has the potential to improve precision and efficacy in abdominal radiotherapy (RT). However, the long reconstruction time of the state-of-the-art reconstruction method, compress-sensed-based respiratory-correlated 4D-MRF (CS-RC-4DMRF), limits its clinical application.
Goal(s): The study aims to develop a novel method to reduce the reconstruction time of CS-RC-4DMRF.
Approach: We developed PGDN-RC-4DMRF by integrating a deep proximal gradient descent network (PGDN) into 4D-MRF. Tumor motion tracking accuracy, tissue quantification accuracy, and image quality were evaluated.
Results: The proposed PGDN-RC-4DMRF method reduce the reconstruction time by a factor of 120, decreasing it from 8 min/slice to 4 s/slice while maintaining other metrics.
Impact: The improvement in the reconstruction speed of 4D-MRF through PGDN-RC-4DMRF may enhance the practicality of 4D-MRF in clinical settings for clinicians and potentially benefit RT outcomes for patients.
INTRODUCTION
Four-dimensional MR fingerprinting (4D-MRF) has great potential for abdominal radiotherapy (RT) by capturing respiratory-correlated (RC) tissue property maps under free breathing1-4. The previous state-of-the-art method, compressive-sensing-based RC 4D-MRF (CS-RC-4DMRF), incorporated motion fields (MFs) to align all k-space data to one bin and subsequently reconstructed property maps for that bin iteratively3. CS-RC-4DMRF improves tumor motion-tracking accuracy, tissue quantification accuracy, and overall image quality3. However, its long reconstruction time has limited its clinical adoption. Recently, deep neural networks, especially model/physics-based unrolled networks5-8, have been explored for accelerating image reconstruction. These networks enforce data-driven priors via a deep neural network and perform well with smaller training sets, offering a way for accelerating CS-RC-4DMRF reconstruction. In this study, we develop a novel 4D-MRF reconstruction method named PGDN-RC-4DMRF, which employs a deep proximal gradient descent network9 (PGDN) to significantly reduce the reconstruction time of CS-RC-4DMRF. Results demonstrate that the proposed PGDN-RC-4DMRF method can reduce the reconstruction time of CS-RC-4DMRF by 120 times while maintaining comparable performance in tumor motion-tracking accuracy, tissue quantification accuracy, and image quality.METHODS
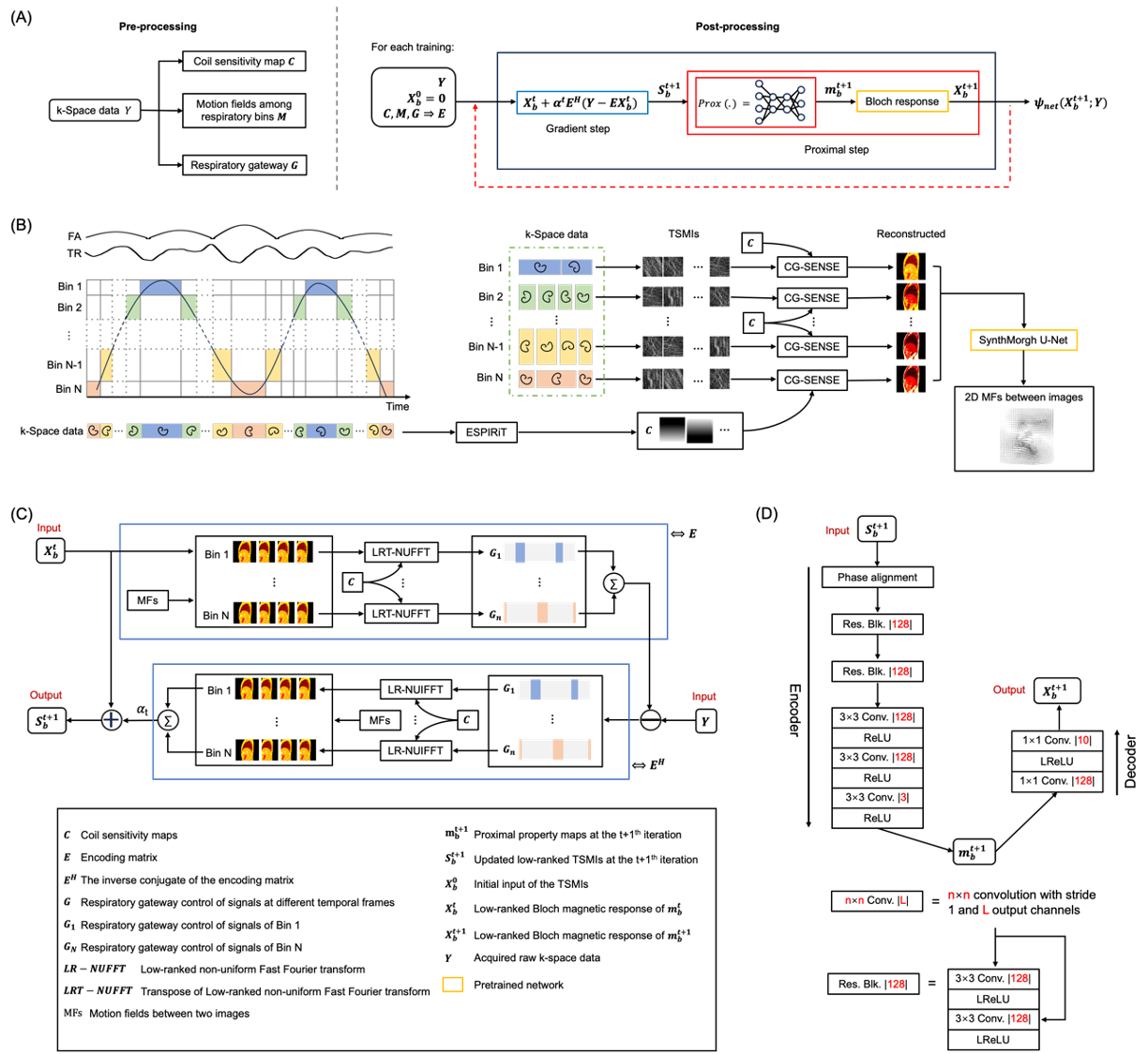
PGDN-RC-4DMRF techniqueFigure 1(A) illustrates the PGDN-RC-4DMRF pipeline comprising: (1) a pre-processing step for estimating coil sensitivity maps, respiratory information and MFs among respiratory bins (Figure 1(B)); and (2) a post-processing step for training the PGDN network to reconstruct property maps effectively (Figure 1(C)&(D)).
Given the MRF k-space data Y, the goal of PGDN-RC-4DMRF is to solve the optimization problem:
$$argmin‖Y-EX_b ‖_2^2+ψ_{net}(X_b;W)$$
where Xb is the low-rank complex-valued 2D time-series magnetic images (TSMIs) at respiratory bin b. ψnet is a neural network parameter by W, and E is the spatial encoding operator defined as:
$$E=\sum_1^n{F_Ω CM_b^i G_{bt} V}$$
where $$$F_Ω$$$ is the non-uniform Fourier transform (NUFFT) matrix with non-Cartesian sampling trajectory Ω, C is the coil sensitivity maps, M is the MFs from bin b to i, V is an orthonormal matrix that embeds TSMIs in low-ranked TSMIs, and G represents respiratory gateway control.
The above optimization problem can be solved by training PGDN, which includes a gradient descent step (Figure 1(C)) that encourages data consistency and the proximal step (Figure 1(D)) that serves the role of regularization.
Loss is defined as the sum of the mean square error (MSE) and total variation (TV) of the predicted property maps of respiratory bin b.
Experiments
Simulated datasets: Three 16-slice free-breathing abdominal datasets were generated using the XCAT phantom10 including T1, T2, and PD maps with a tumor in the liver. Forty-five-channel coil sensitivity maps were added and numerical MRF k-space data were generated with MRF-FISP parameters: TI=18ms, total number of RF pulses=1000, TE=1.77ms, FA=0°-70°, TR=11.7-14.3ms, a rotation angle of spiral interleaves=360°/377, slice thickness=5mm, in-plane resolution=256×256, FOV= 300×300mm2.
Implementation details: The k-space data were first compressed using ESPIRiT and the MRF k-space data were grouped into four amplitude bins based on respiratory amplitudes detected using a 30-frame time window. Soft-SENSE was used for reconstructing images of each bin and MFs among the images were estimated using a pre-trained SynthMorph network. Two datasets including 32 samples were used for training and one dataset including 16 samples for testing, using the Pytorch interface and NVIDIA RTX A6000 GPU with 48GB memory. The Adam optimizer was employed with lr = 10-4, β1 = 0.9, β2 = 0.999, mini-batch size=1, and 1000 epochs.
Evaluation: The proposed PGDN-RC-4DMRF was compared to CS-RC-4DMRF in terms of tumor motion tracking accuracy, tissue quantification accuracy, and image quality. Metrics including tumor motion amplitudes, MAPE, PSNR, and SSIM were calculated and evaluated by a two-sample paired t-test.
RESULTS
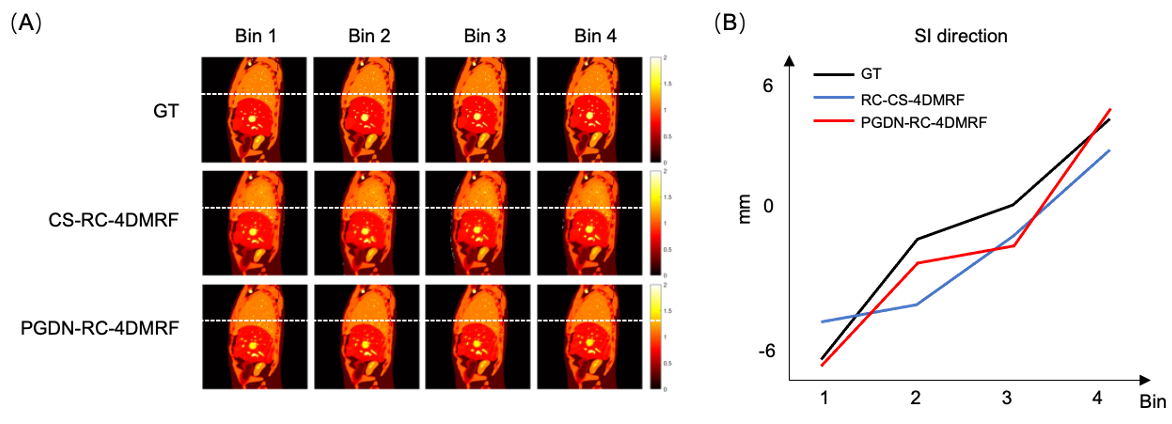
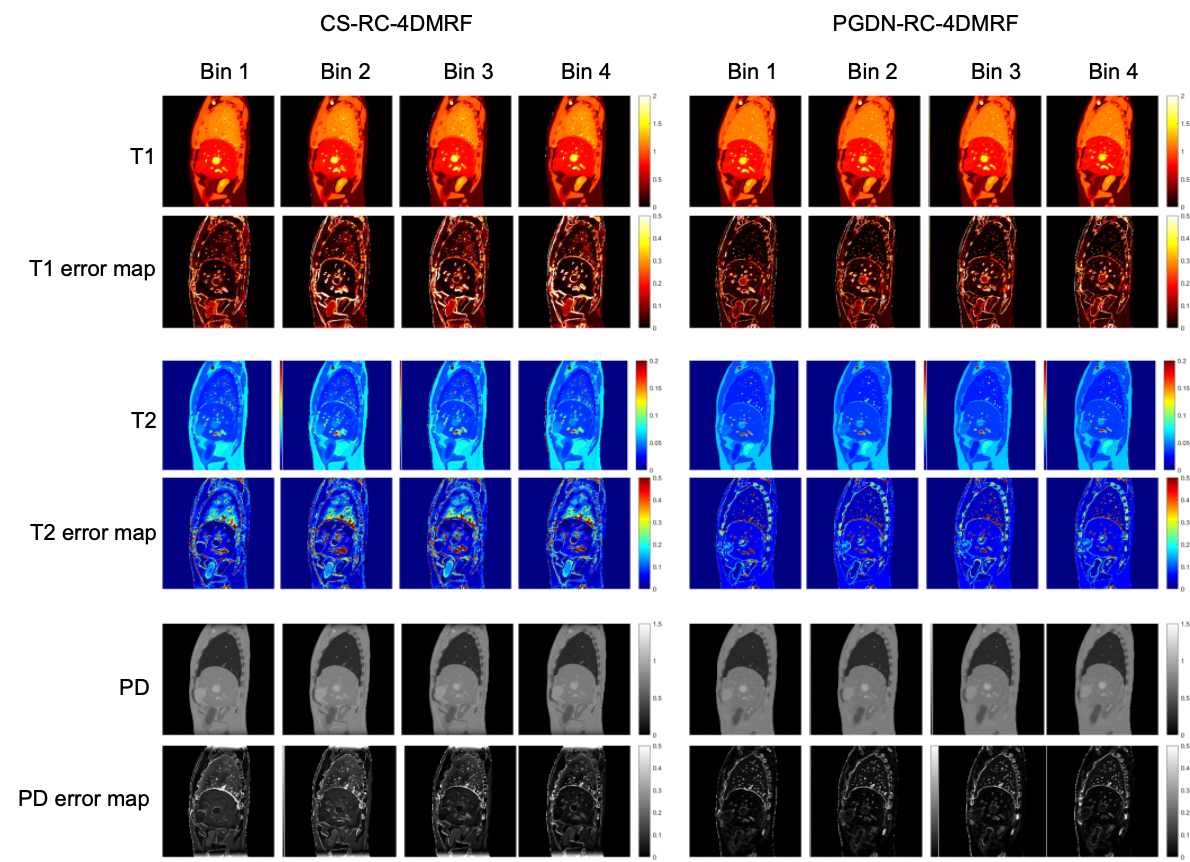
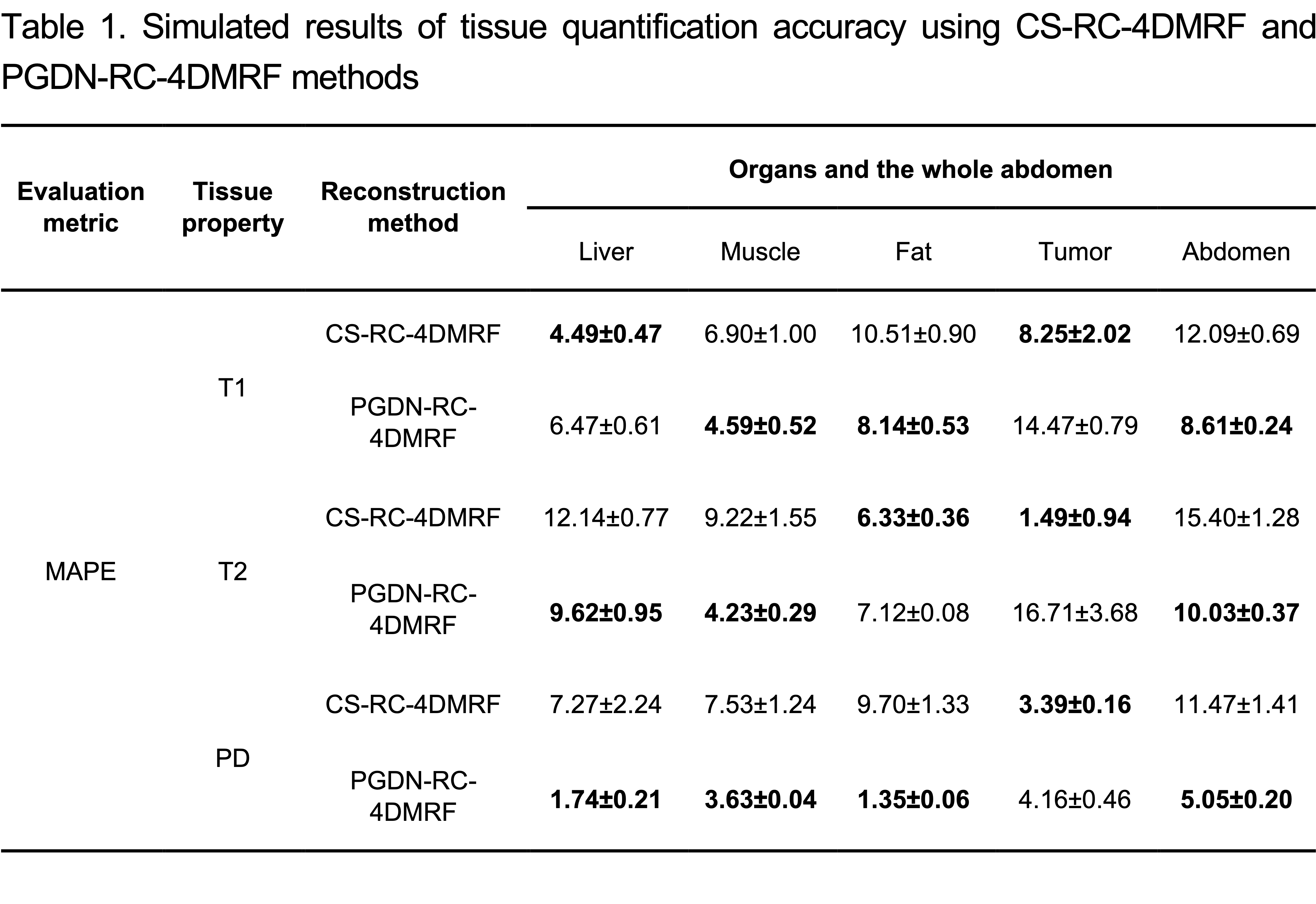
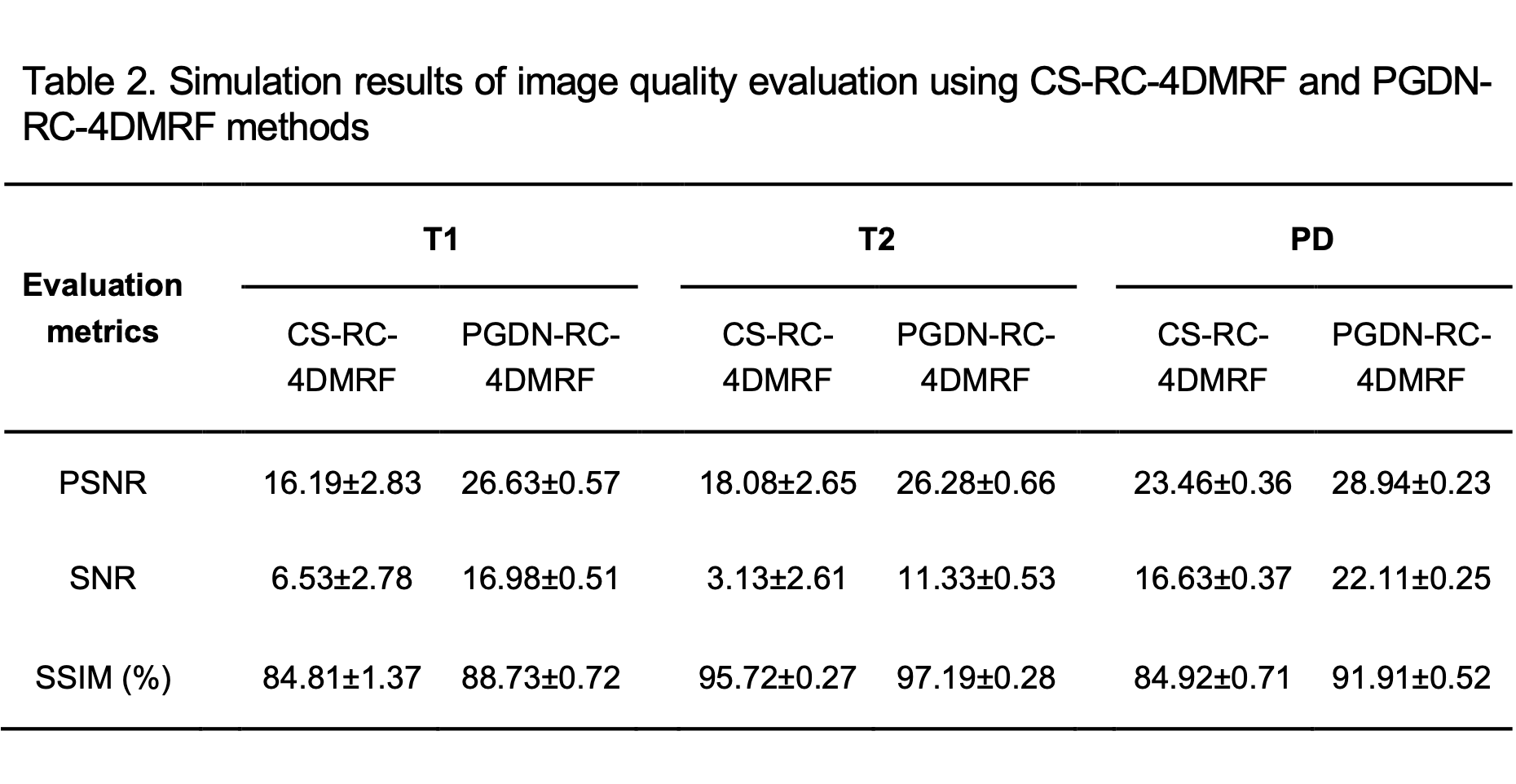
Figure 2 shows that the motion-tracking accuracy of PGDN-RC-4DMRF is higher than that of CS-RC-4DMRF (p<0.05, all). Figures 3 & 4 demonstrate that PGDN-RC-4DMRF outperforms CS-RC-4DMRF in whole abdominal tissue property quantification. PGDN-RC-4DMRF achieves lower MAPE values of 8.61%, 10.03%, and 5.05% for T1, T2, and PD maps, respectively, compared to 12.09%, 15.40%, and 11.47% for CS-RC-4DMRF (p<0.05, all). Moreover, Figure 5 indicates that PGDN-RC-4DMRF provides improved image quality, as demonstrated by the enhanced PSNR, SNR, and SSIM metrics compared to CS-RC-4DMRF (p<0.05, all)DISCUSSION&CONCLUSION
It is feasible for the trained unrolling network, i.e., PGDN-RC-4DMRF, to act as a regularization term and reduce the number of iterations of CS-RC-4DMRF. The edges of the images reconstructed from PGDN-RC-4DMRF are sharper than those from CS-RC-4DMRF (Figure 2&3), which benefits from the accurate MFs and deep learning properties. One problem is even though the tumor motion-tracking accuracy and whole image quality are better than CS-RC-4DMRF, the tumor quantification accuracy of PGDN-RC-4DMRF is not comparable with CS-RC-4DMRF, which needs to be further improved.Acknowledgements
The work is supported by General Research Funds (GRF 15102219, GRF 15104822), National Natural Science Foundation of China (NSFC) Young Scientist Fund (8220294)References
1. Li T, Cui D, Hui ES, Cai J. Time-resolved magnetic resonance fingerprinting for radiotherapy motion management. Medical Physics. 2020;47(12):6286-6293.2. Huang SS, Boyacioglu R, Bolding R, MacAskill C, Chen Y, Griswold MA. Free-breathing abdominal magnetic resonance fingerprinting using a pilot tone navigator. Journal of Magnetic Resonance Imaging. 2021;54(4):1138-1151.
3. Liu C, Li T, Cao P, et al. Respiratory-Correlated 4-Dimensional Magnetic Resonance Fingerprinting for Liver Cancer Radiation Therapy Motion Management. International Journal of Radiation Oncology* Biology* Physics. Published online 2023.
4. Li T, Cui D, Ren G, Hui ES, Cai J. Investigation of the effect of acquisition schemes on time-resolved magnetic resonance fingerprinting. Physics in Medicine & Biology. 2021;66(9):095013.
5. Yaman B, Hosseini SAH, Moeller S, Ellermann J, Uğurbil K, Akçakaya M. Self‐supervised learning of physics‐guided reconstruction neural networks without fully sampled reference data. Magnetic Resonance in Med. 2020;84(6):3172-3191. doi:10.1002/mrm.28378
6. Combettes PL, Pesquet JC. Proximal Splitting Methods in Signal Processing. In: Bauschke HH, Burachik RS, Combettes PL, Elser V, Luke DR, Wolkowicz H, eds. Fixed-Point Algorithms for Inverse Problems in Science and Engineering. Vol 49. Springer Optimization and Its Applications. Springer New York; 2011:185-212. doi:10.1007/978-1-4419-9569-8_10
7. Daubechies I, Defrise M, De Mol C. An iterative thresholding algorithm for linear inverse problems with a sparsity constraint. Comm Pure Appl Math. 2004;57(11):1413-1457. doi:10.1002/cpa.20042
8. Boyd S, Parikh N, Chu E, Peleato B, Eckstein J. Distributed optimization and statistical learning via the alternating direction method of multipliers. Foundations and Trends® in Machine learning. 2011;3(1):1-122.
9. Chen D, Davies ME, Golbabaee M. Compressive MR Fingerprinting Reconstruction with Neural Proximal Gradient Iterations. In: Martel AL, Abolmaesumi P, Stoyanov D, et al., eds. Medical Image Computing and Computer Assisted Intervention – MICCAI 2020. Vol 12262. Lecture Notes in Computer Science. Springer International Publishing; 2020:13-22. doi:10.1007/978-3-030-59713-9_2
10. Segars, W. P., Sturgeon, G., Mendonca, S., Grimes, J., & Tsui, B. M. (2010). 4D XCAT phantom for multimodality imaging research. Medical physics, 37(9), 4902-4915.
Figures