1075
Development and validation of a rapid robust 3D-MRF with fast online recon suitable for large-scale neuroscientific and clinical applications1Department of Radiology, Stanford university, Stanford, CA, United States, 2Graduate School of Education, Stanford University, Stanford, CA, United States, 3Department of Electrical Engineering, Stanford University, Stanford, CA, United States, 4Division of Developmental Behavioral Pediatrics, Department of Pediatrics, Stanford University School of Medicine, Stanford, CA, United States, 5Department of Radiology, Stanford University School of Medicine, Stanford, CA, United States, 6Department of Psychology, Stanford University, Stanford, CA, United States
Synopsis
Keywords: Software Tools, Software Tools, Pipeline, MR Fingerprinting
Motivation: A number of promising multiparameter mapping approaches have been developed but are not yet in routine-use in clinical and neuroscientific settings.
Goal(s): To create a rapid and robust 3D-MRF acquisition/reconstruction package, suitable for large-scale neuroscientific and clinical applications.
Approach: 3D-MRF acquisition is developed for 1-mm whole-brain-mapping in 2.5-minutes, with build-in robustness to motion, and quantification bias from B0&B1 inhomogeneities. Highly-efficient reconstruction package is created for online generation of quantitative maps and synthesized-contrasts within 4 minutes of scan-completion, benchmarked using a consumer-grade GPU.
Results: The pipeline has been validated on over 100-scans performed across clinical and neuroscientific settings with plan for open-source distribution soon.
Impact: The distribution of such an acquisition/reconstruction package should help facilitate wide-spread deployment of multiparameter mapping.
Introduction
Recent advances in MR Fingerprinting (MRF) allow for rapid high-resolution quantitative mapping. However, its clinical application faces challenges: (A)The lengthy reconstruction hampers real-time viewing of results, impeding image quality checks and prompt head-motion monitoring to avoid patient recall. (B)Field-inhomogeneities (B0/B1) degrade the images, necessitating additional calibration scans that prolong scan and reconstruction.Efforts have been made for automated MRF reconstruction pipelines1. However, the current pipelines haven't reported the B0-correction incorporation, which requires additional calibration scans and significantly longer reconstruction. We've introduced a pipeline with B0-correction but without B1-incorporated2,3, compromising the accuracy of T2 map. Furthermore, in the real-world clinical deployment of our pipeline, we encountered practical challenges: unintentional operation by the technologist can cause FOV-misalignment between the MRF and calibration scans, leading to challenges in accurate B0/B1 estimation and longer reconstruction due to extra registration. Additionally, patient head motion degrades the image quality.
To address these issues, we refine our pipeline on both the sequence and the reconstruction sides. This not only reduces the reconstruction time (to within 4-minutes), but also enhances the result robustness to B0/B1 inhomogeneity and head-motion. The proposed acquisition/reconstruction pipeline has been validated on over 100-scans performed across clinical and neuroscientific settings with plan for open-source distribution soon.
Method
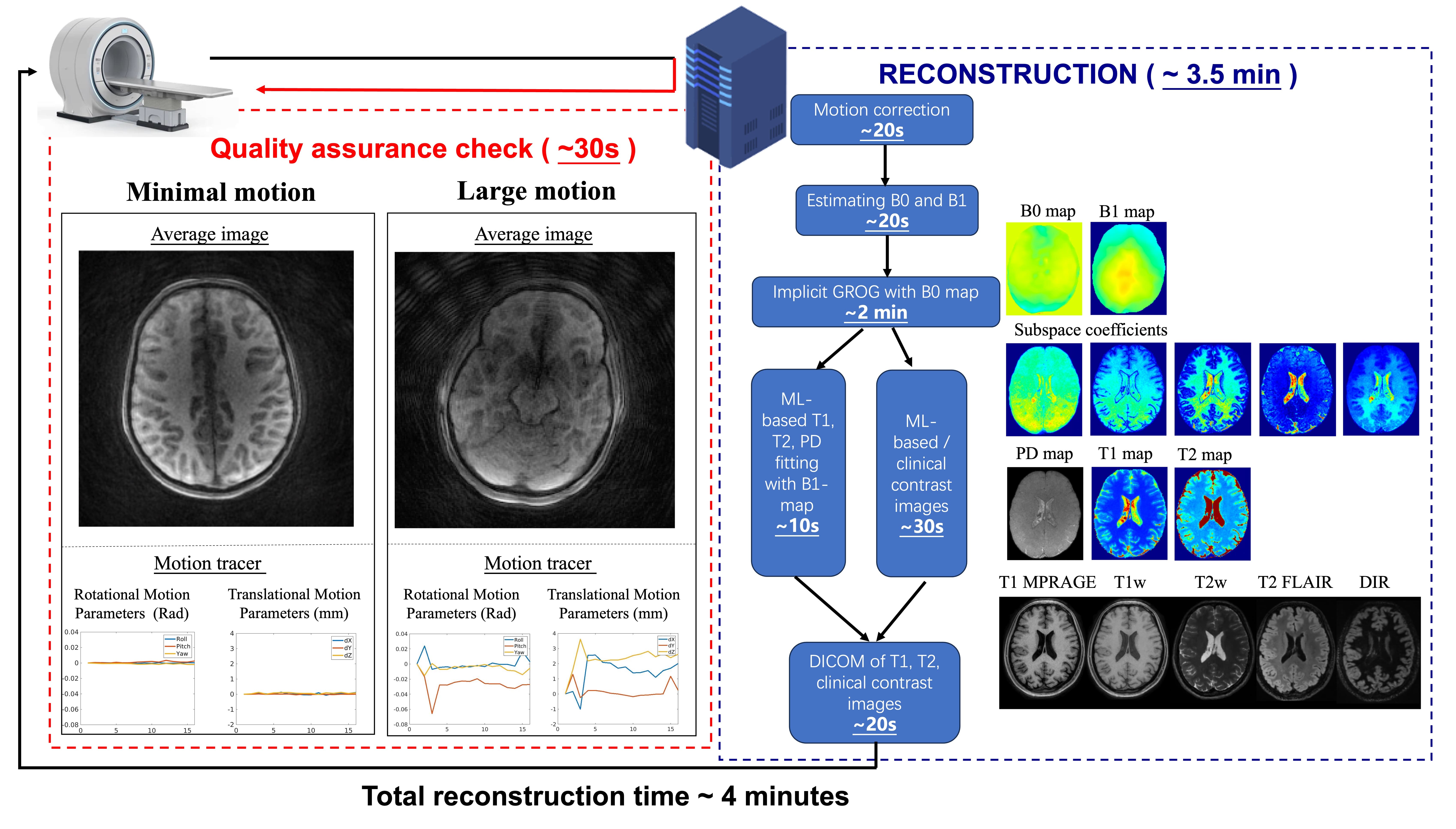
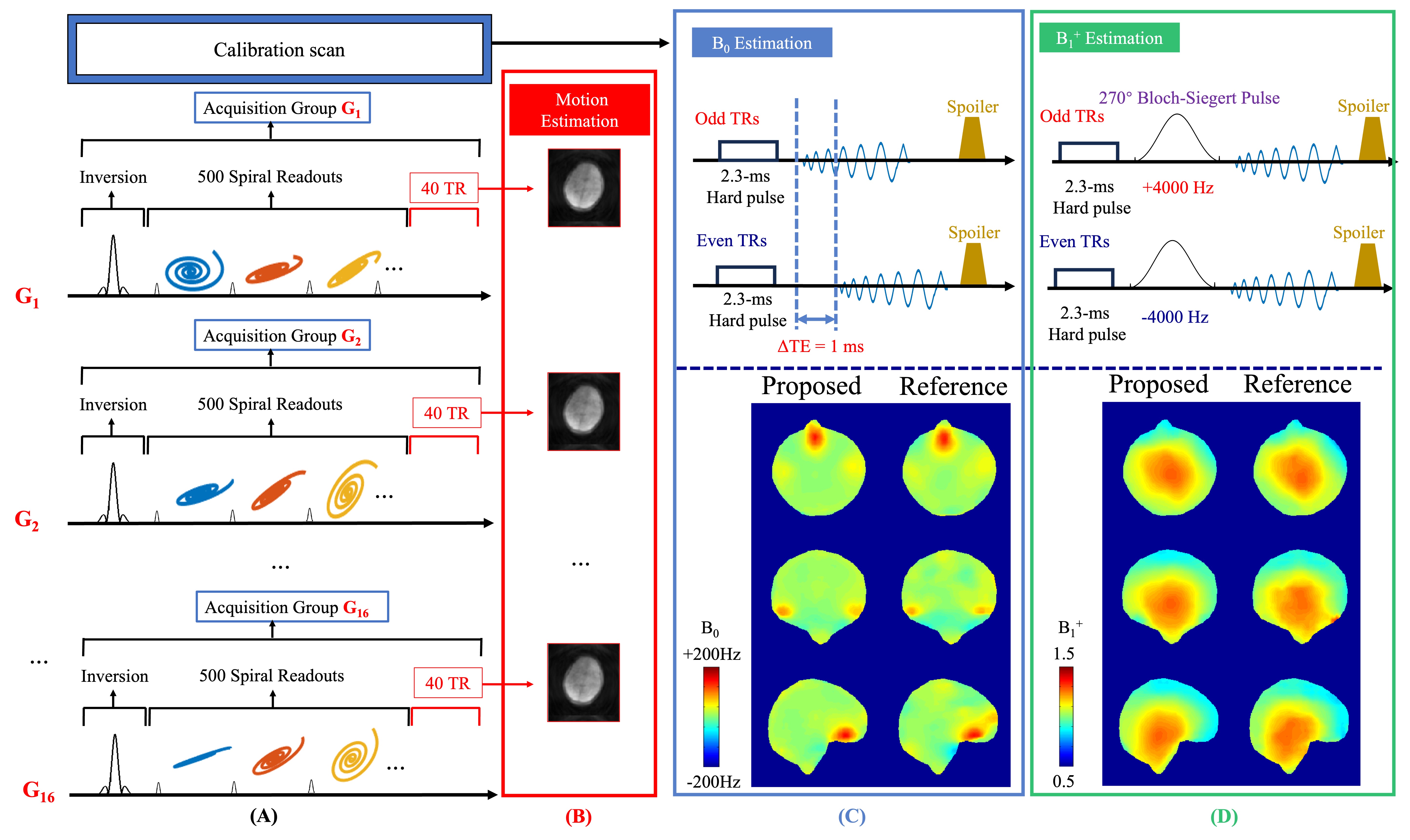
The pipeline (Fig.1) is based on a new-version MRF (Fig.2) that we've developed using 3D-spiral-projection MRF4, where rapid B0&B1 measurements are incorporated into the MRF’s dummy scan period, and motion navigators are added into the sequence dead-time every 7s, achieving well-aligned B0&B1 estimation and motion measurements. The MRF sequence takes 2.5-minutes to perform 1-mm whole-brain mapping.Within 30-second after scan completion, an average-contrast image and motion tracers are displayed online to aid rapid quality assurance, with rescan recommendation if dx/dy/dz>3-mm/rotation>0.05-rad (For smaller-motion, the build-in motion-aware reconstruction can ensure high quality results). The pipeline then progress with 20-second for B0&B1 estimations, 2-minute for efficient subspace reconstruction with B0-time-segmented correction using a recently-developed field-correcting implicitGROG algorithm5, followed by 30-second for ML-based parameter mapping that accounts for B1-inhomogeneity6 and ML-based semi-supervised contrast synthesis7,8. Finally, the T1,T2, and clinical-contrast images are converted to DICOM and sent to the scanner. The whole pipeline takes less than 4-minutes.
This pipeline has already been deployed at the Lucile Packard Children's Hospital(LPCH) for clinical use and at the Stanford Center for Cognitive and Neurobiological Imaging(CNI) where it has been adopted in a longitudinal intervention study for reading development.
Result
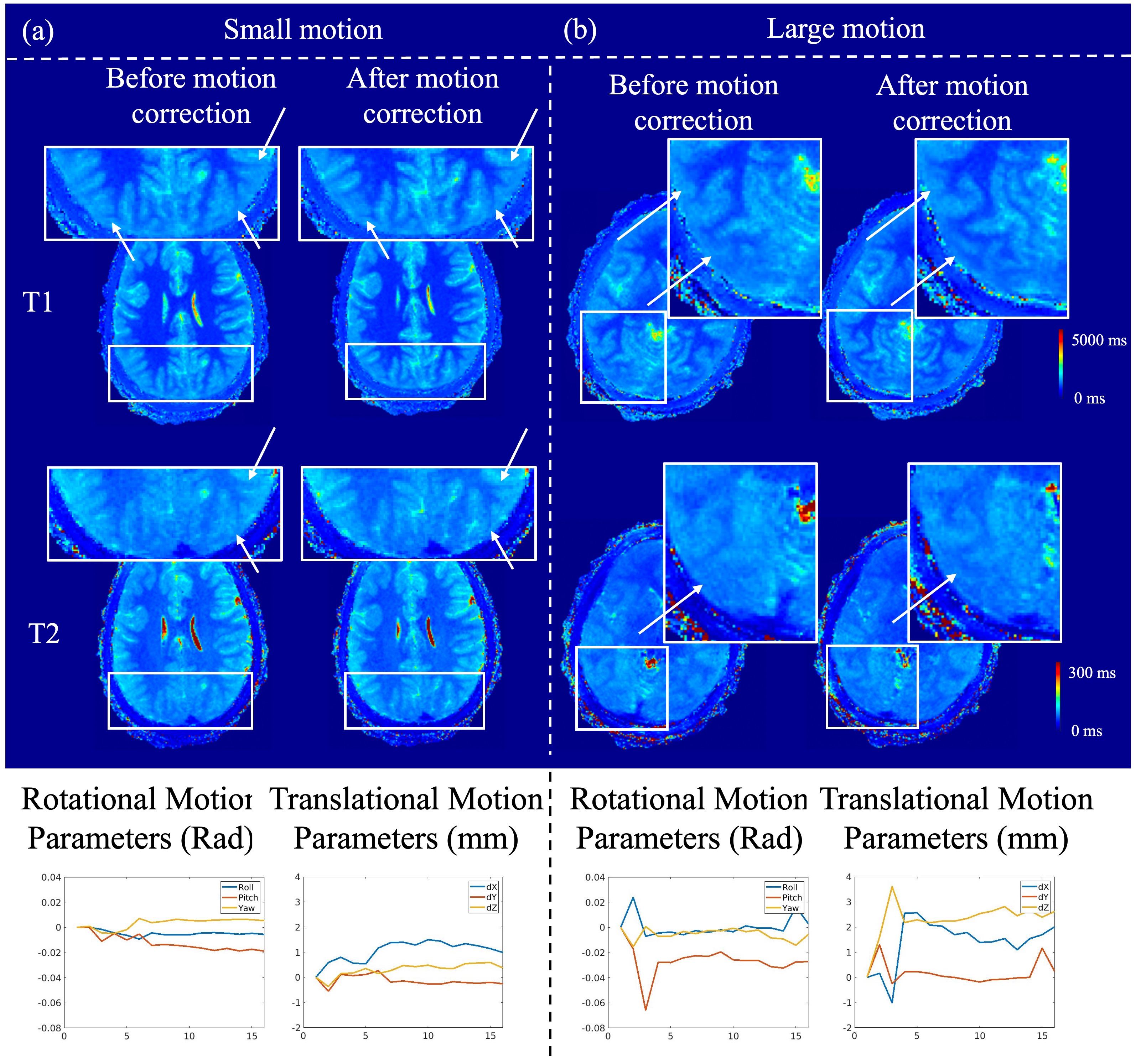
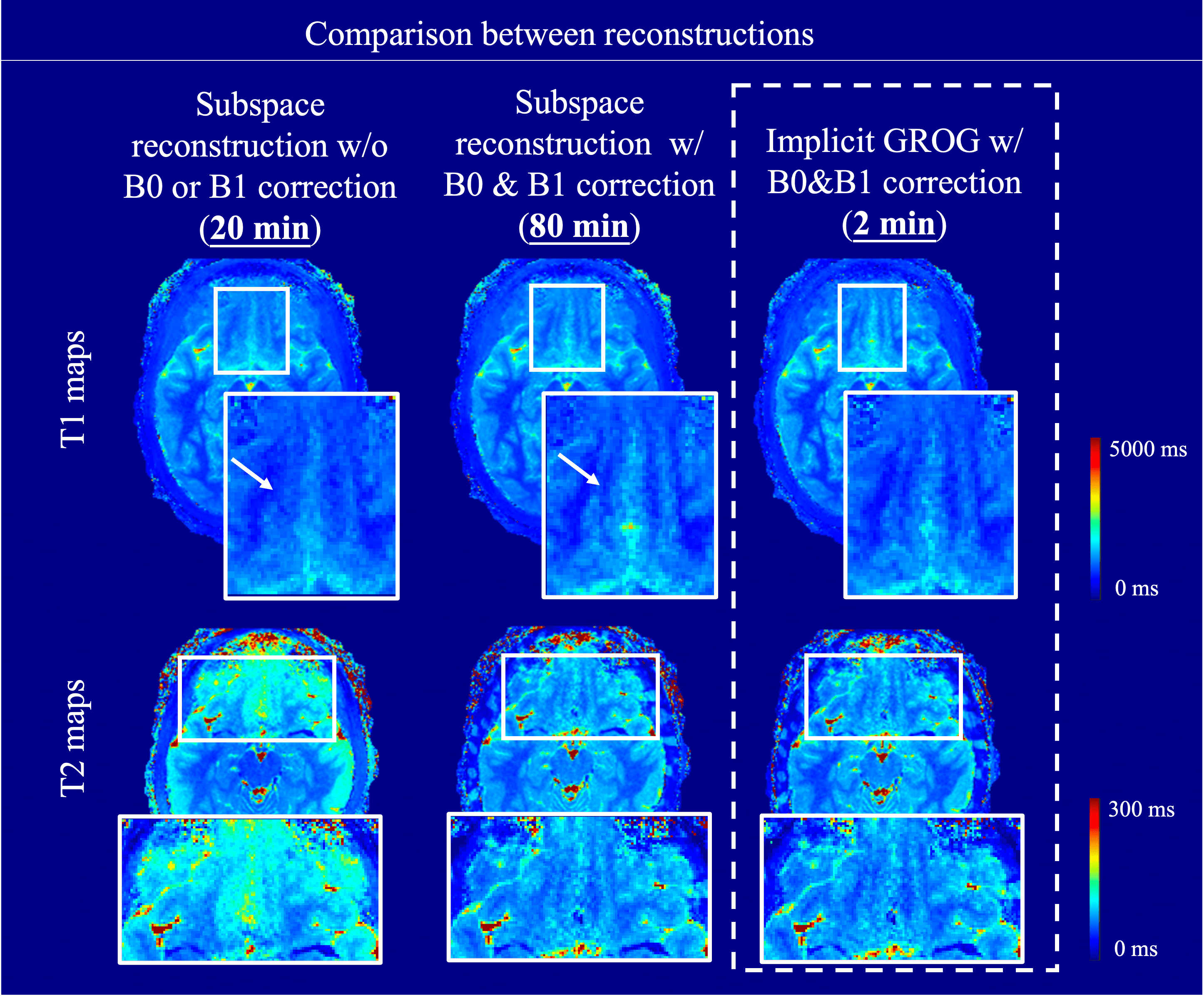
Fig.3 shows T1,T2 maps w/o and w/ motion-aware reconstruction for small&large motion cases.Fig.4 shows reconstruction results, where w/ B0&B1-correction it significantly improves the quality of T1&T2 maps. The field-correcting implicitGROG reconstruction achieves comparable results to gold-standard time-segmented subspace reconstruction, but with 40x faster speed.
Fig.5 shows application of pipeline. (a) Results from 2 representative clinical cases, where lesions are well-delineated in the synthetic images.(b) shows preliminary results from a longitudinal neuroscientific study using our MRF acquisition/reconstruction package.
Discussion
We proposed an easy-to-deployed automated MRF acquisition/reconstruction package, which we have validated and plan for open-source distribution soon.Compared to exist pipelines, we include B0&B1-correction and motion-correction without adding processing time. For reconstruction, the use of gold-standard B0-time-segmented subspace reconstruction with locally-low-rank produces high quality results at a cost of a lengthy (80-minutes) reconstruction, even through an efficient ‘sigpy’-based implementation.The use of a recently-developed field-correction implicitGROG5, and polynomial-preconditioning9 can markedly reduce reconstruction time to 2-minutes, while retaining high image quality.
Based on clinical feedback, our pipeline has been updated in two ways. (A)By incorporating the B1&B0 calibration scans into MRF’s dummy-period, which effectively mitigating misalignment errors/motion between scans. (B)Motion-estimation and its incorporation into the reconstruction can improve image quality adequately for small-to-moderate head-movements. For larger motion, a motion-tracer is implemented, allowing for rapid assessment and guidance for same-session re-scan, minimizing the need for patient recall.
The deployment to clinical use shows synthetic contrast images have similar contrasts with clinical sequences and can accurately detect lesions with much shorter scan-time, demonstrating the value in MRF’s clinical translation. The pipeline has also applied to a longitudinal study. Thirty-six 8-13 year-old children were scanned twice, with a 2/4-month interval in-between. Preliminary results show high repeatable T1 values within CC while T2 shows observable change. The unexpected reduction of T2 repeatability in anterior CC may be attributed to brain development. However, the proximity of this region to CSF could also cause increased partial-volume effects, which necessitate further investigation using multi-compartment analysis to remove any potential confound, which is underway.
Conclusion
A robust and repeatable MRF acquisition/reconstruction package was developed and validated to provide high-fidelity T1, T2, and clinical contrasts images with near real-time reconstruction.Acknowledgements
This work was supported by grants: R01MH116173, R01EB019437, U01EB025162, P41EB030006, R01EB033206, U24NS129893, R01-HD095861References
1. Dupuis A, Boyacioglu R, Chen Y, et al., Fully automated online reconstruction, registration and analysis pipeline for 3D Magnetic Resonance Fingerprinting. In Proceeding of Annual Meeting of the ISMRM, Toronto, Canada, May. 2023, pp:0422.
2. Schauman S, Iyer SS, Cao X, et al., Five clinical contrasts from 1 minute whole brain MRF with B0 correction. In Proceeding of Annual Meeting of the ISMRM, Toronto, Canada, May. 2023, pp: 2184.
3. Schauman S, Iyer SS, Yurt M, et al., Toward a 1-minute high-resolution brain exam- MR Fingerprinting with fast reconstruction and ML-synthesized contrasts. In Proceeding of Annual Meeting of the ISMRM, London, UK, May. 2022, pp: 0053.
4. Cao X, Liao C, Iyer SS, et al., Optimized multi-axis spiral projection MR fingerprinting with subspace reconstruction for rapid whole-brain high-isotropic-resolution quantitative imaging. MRM. 2022; 88(1):133-150.
5. Nishimura M, Abraham D, Zhou Z, et al., Efficient Constrained Reconstruction of Non-Cartesian Time-Segmented Data with Implicit GROG and Polynomial Preconditioning. In Proceeding of Annual Meeting of the ISMRM, 2024.
6. Gao M, Cao X, Abraham D, et al., Sequence adaptive deep learning framework to improve accuracy and robustness of MRF quantification via retrospective estimation and correction of B1+ and B0 inhomogeneities. In Proceeding of Annual Meeting of the ISMRM, 2024.
7. Yurt M, Alkan C, Schauman S, et al., Semi-Supervision for Clinical Contrast-Weighted Image Synthesis from Magnetic Resonance Fingerprinting. In Proceeding of Annual Meeting of the ISMRM, Toronto, Canada, May. 2023, pp: 0423.
8. Yurt M, Zhou Z, Liao C, et al., Unlocking Data-Consistent Synthesis of Clinical Contrasts fromMagnetic Resonance Fingerprinting with Semi-Supervised Learning. In Proceeding of Annual Meeting of the ISMRM, 2024.
9. Iyer SS, Frank O, Cao X, et al., Polynominal preconditioners for regularized linear inverse problems. arXiv:2204.10252.
Figures