1071
Alternating low-rank tensor reconstruction for more precise and repeatable multiparametric mapping with Cardiovascular MR Multitasking1Department of Radiological Sciences, University of California, Los Angeles, Los Angeles, CA, United States, 2Biomedical imaging research institute, Cedars Sinai Medical Center, Los Angeles, CA, United States, 3Departments of Imaging and Cardiology, Cedars Sinai Medical Center, Los Angeles, CA, United States, 4Department of Bioengineering, University of California, Los Angeles, Los Angeles, CA, United States
Synopsis
Keywords: Quantitative Imaging, Sparse & Low-Rank Models
Motivation: While MR Multitasking shows initial promise as a free-breathing, non-ECG approach for multiparametric CMR, its precision and repeatability still require further improvement to match the widely adopted clinical protocols.
Goal(s): To improve precision and repeatability of multiparametric mapping by cardiovascular MR Multitasking.
Approach: A novel low-rank tensor reconstruction strategy was developed to improve the reconstruction performance. Numerical simulations and in-vivo studies on healthy volunteers and cardiomyopathy patients were used to evaluate the proposed technique.
Results: Compared to conventional recontruction, the proposed approach showed lower RMSE in numerical simulations, and improved precision by ~20% and repeatability by ~30% in in-vivo studies.
Impact: The improved cardiovascular MR Multitasking has the potential to be an efficient and subject friendly (free-breathing, non-ECG) alternative for diagnosis of CMR patients whose T1 and T2 changes are greater than 100 ms and 2 ms, e.g., amyloidosis patients.
Introduction
Quantitative cardiovascular MR (CMR) provides objective information for diagnosis and prognosis of cardiovascular diseases1.2. This objectivity hinges on precision and repeatability, which are vital for diagnostic confidence and longitudinal studies. MR Multitasking3 is promising for comprehensive tissue characterization within a practical scan time. However, MR Multitasking currently estimates spatial and temporal low-rank model factors from separate subsets of acquired data, which may compromise reconstruction performance. Here we developed a novel low-rank tensor reconstruction approach to jointly estimate spatial/temporal factors from the entire acquired dataset, in pursuit of improving precision and repeatability. The approach was evaluated for 2D myocardial T1/T2 mapping in numerical simulations, healthy volunteers, and cardiomyopathy patients.Methods
Data collectionA numerical phantom was created from the XCAT phantom4, using 20 cardiac$$$\times$$$6 respiratory bins and simulating Multitasking 2D T1/T2 acquisition3. For in-vivo healthy volunteer studies, N=10 volunteers (3 males, age: 36.4±12.5y) were scanned on a 3T scanner (Siemens). The Multitasking acquisition was also integrated into a clinical protocol for cardiomyopathy patients, with N=11 patients (9 males, age: 57.5±13.9y) scanned on a 3T scanner (Siemens). The acquisitions were performed on the mid-ventricular slice with short-axis view twice to assess repeatability.
Image reconstruction
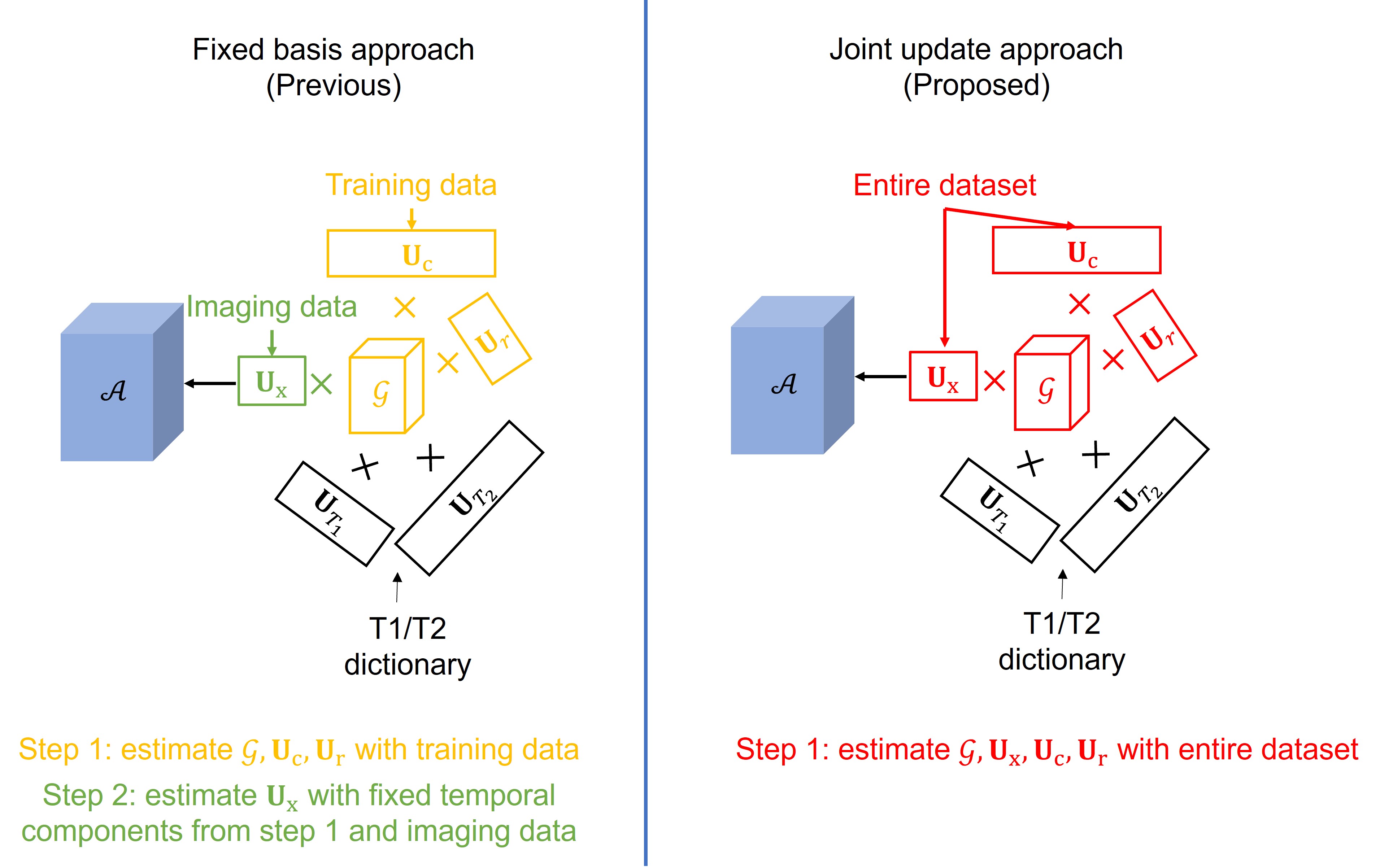
The underlying image series is modeled as a low-rank tensor with Tucker decomposition, i.e. $$$\mathcal{A}=\mathcal{G}\times_1 \mathbf{U}_{\mathrm{x}} \times{ }_2 \mathbf{U}_{\mathrm{c}} \times{ }_3 \mathbf{U}_{\mathrm{r}} \times{ }_4 \mathbf{U}_{\mathrm{T}_1} \times{ }_5 \mathbf{U}_{\mathrm{T}_2}$$$, where $$$\mathbf{U}_{\mathrm{x}}$$$ are the spatial factors, $$$\mathbf{U}_{\mathrm{c}}$$$ and $$$\mathbf{U}_{\mathrm{r}}$$$ are the cardiac and respiratory motion bases, and $$$\mathbf{U}_{\mathrm{T}_1}$$$ and $$$\mathbf{U}_{\mathrm{T}_2}$$$ are the pre-computed basis functions for T1 and T2 relaxation. Different from previously used fixed basis approach3 (as shown in Figure 1), here we sought to jointly solve spatial and temporal components using the entire acquired dataset as follows:
$$\begin{aligned}& \widehat{\mathbf{U}}_{\mathrm{x}}, \hat{\mathcal{G}}, \widehat{\mathbf{U}}_{\mathrm{c}}, \widehat{\mathbf{U}}_{\mathbf{r}} \\& =\arg \min _{\mathbf{U}_{\mathrm{x}}, \mathcal{G}, \mathbf{U}_{\mathrm{c}}, \mathbf{U}_{\mathrm{r}}}\left\|\mathbf{d}_{\mathrm{all}}-\Omega\left(\mathcal{G} \times_1 \mathbf{F S} \mathbf{U}_{\mathrm{x}} \times_2 \mathbf{U}_{\mathrm{c}} \times_3 \mathbf{U}_{\mathbf{r}} \times_4 \mathbf{U}_{\boldsymbol{T}_1} \times_5 \mathbf{U}_{\boldsymbol{T}_2}\right)\right\|_2^2+\lambda_1\left\|W \mathbf{U}_{\mathrm{x}}\right\|_1 \\& +\lambda_2\|\mathcal{G}\|_1, \text { s.t. }\mathbf{U}_{\mathrm{c}}^H \mathbf{U}_{\mathrm{c}}=\mathbf{I}, \mathbf{U}_{\mathrm{r}}^H \mathbf{U}_{\mathbf{r}}=\mathbf{I},\end{aligned}$$
where $$$\mathbf{d}_{\mathrm{all}}$$$ is the entire dataset, $$$\mathbf{FS}$$$ denotes sensitivity multiplication and Fourier transform, $$$W$$$ is the wavelet transform, $$$\lambda_1$$$, $$$\lambda_2$$$ are regularization parameters.
Analysis
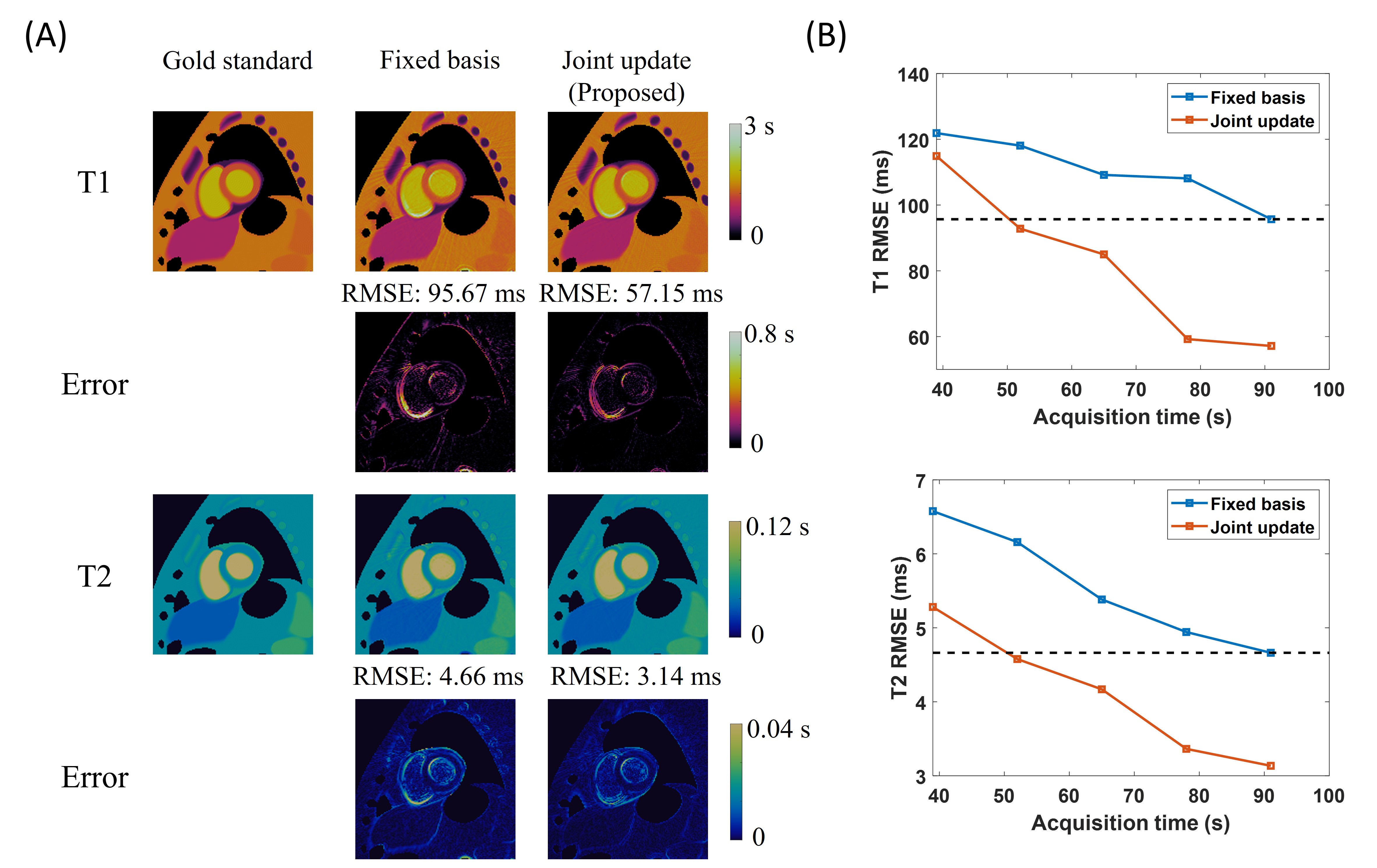
For numerical simulations, root mean squared error (RMSE) between the ground truth and the reconstructed maps was calculated. To evaluate the impact of scan time on different approaches, reconstruction was performed at different scan lengths ([39,52,65,78,91]s).
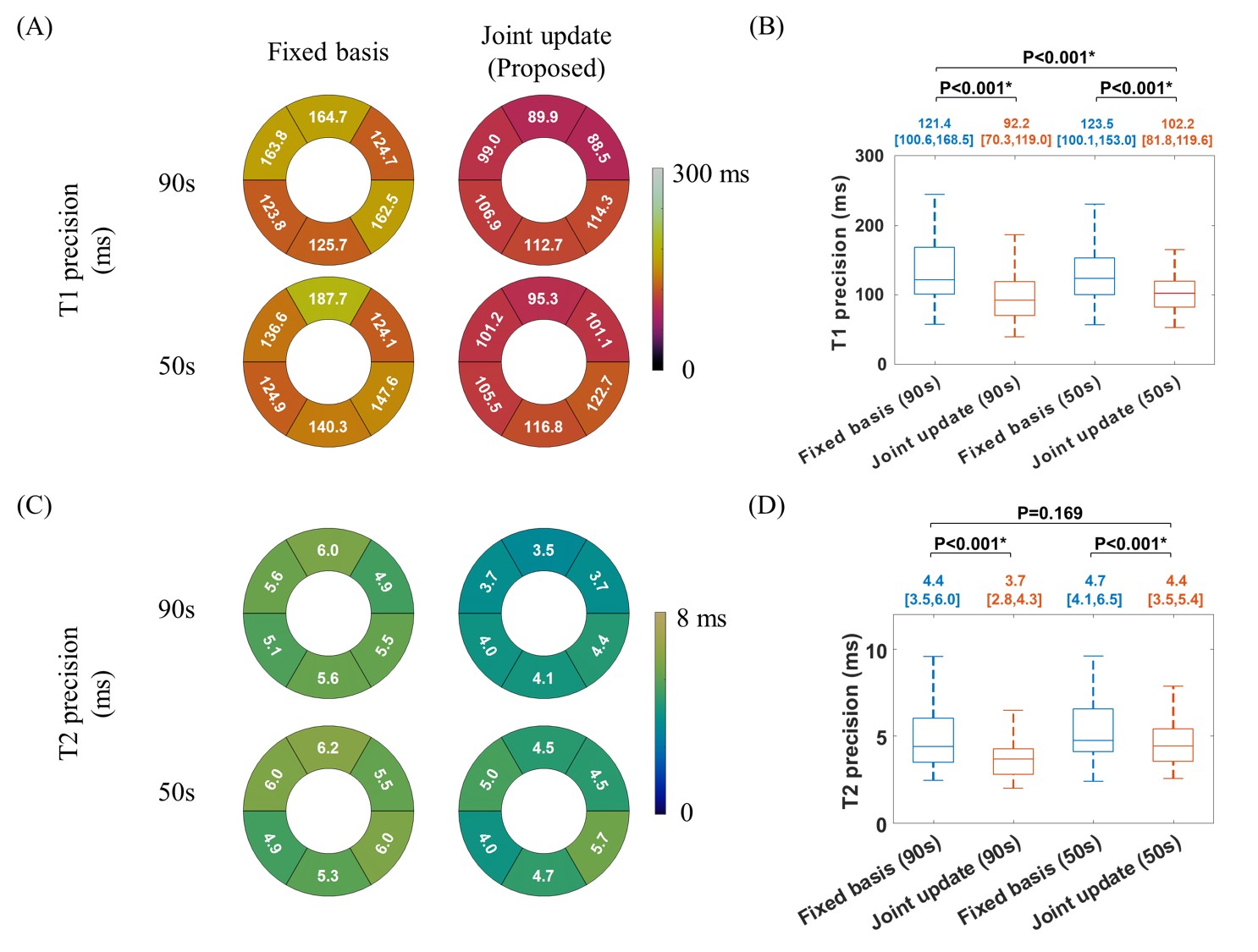
In-vivo reconstruction was performed at scan times of 50s and 90s with different approaches. Precision (voxel-wise standard deviation within a myocardium segment) and repeatability (standard deviation of repeated measurements for the same segment) were evaluated and compared between different approaches. For patients, only repeatability was evaluated, as there is no expectation of myocardial homogeneity. The Wilcoxon signed-rank test was used for statistical comparison.
Results
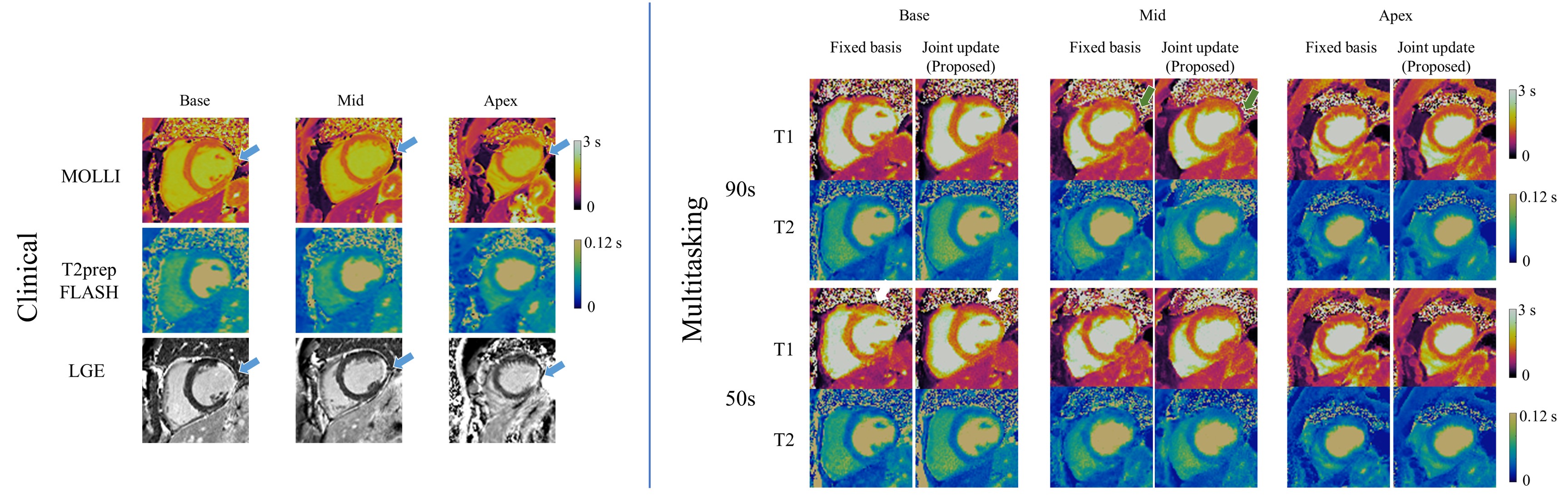
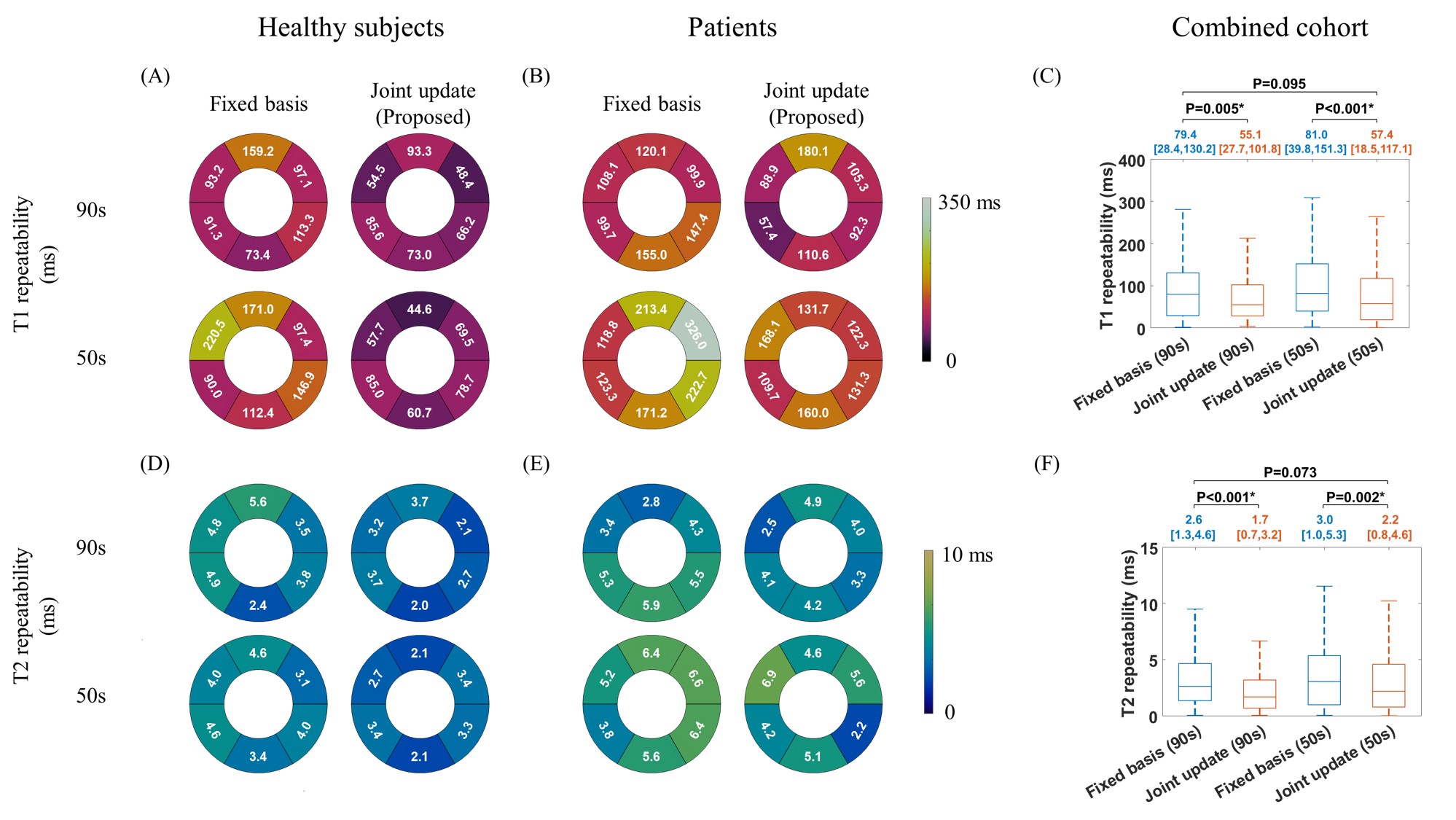
The proposed approach outperformed the fixed basis approach at all scan times, producing lower T1 and T2 RMSE (Figure 2). A 50-s scan time with the proposed approach had comparable RMSE to the 90-s scan time with the fixed basis approach, prompting the in-vivo comparison at these intervals. Figure 3 shows a 73-year-old patient with transmural lesions around the lateral wall, as indicated by clinical MOLLI and late-gadolinium enhancement (LGE). T1 maps from the proposed approach mirrored clinical findings at both scan times. In contrast, the mid-ventricular T1 map from the fixed basis approach at 90-s scan time was unable to define the scar region as clearly (green arrows), and the basal T1 map from the fixed basis approach at 50-s scan time showed false positives in the anterior segment (orange arrows).The T1/T2 precision measurements in healthy subjects are compared in Figure 4. The proposed approach significantly improved precision for both biomarkers at both scan times. Even when truncating to 50-s scan time, the proposed approach still yielded comparable or significantly better precision that that of the previous approach at 90-s scan time. The T1/T2 repeatability measurements over both cohorts are compared in Figure 5. The proposed approach significantly improved repeatability compared to the fixed basis approach. There was no significant difference between repeatability of the proposed approach at 50-s scan time and the previous approach at 90-s scan time.
Discussion and Conclusion
In pursuit of improving precision and repeatability of quantitative CMR with Multitasking, we developed a novel low-rank tensor reconstruction approach that jointly recovers spatial and temporal components using the entire dataset acquired. The proposed approach was evaluated on numerical simulations and in-vivo studies, which significantly improved precision by ~20% and repeatability by ~30%. The approach is promising for improving lesion identification, elevating diagnostic confidence, and enhancing sensitivity. The comparisons across different scan times further indicated the potential of reducing scan time while preserving image quality.Acknowledgements
This work was supported by the National Institutes of Health (Grant/Award Nos. R01EB028146 and R01HL156818).References
- O’Brien AT, Gil KE, Varghese J, Simonetti OP, Zareba KM. T2 mapping in myocardial disease: a comprehensive review. Journal of Cardiovascular Magnetic Resonance 2022;24(1):1-25.
- Aherne E, Chow K, Carr J. Cardiac T1 mapping: techniques and applications. Journal of Magnetic Resonance Imaging 2020;51(5):1336-1356.
- Christodoulou AG, Shaw JL, Nguyen C, Yang Q, Xie Y, Wang N, Li D. Magnetic resonance multitasking for motion-resolved quantitative cardiovascular imaging. Nat Biomed Eng 2018;2(4):215-226.
- Segars WP, Sturgeon G, Mendonca S, Grimes J,
Tsui BM. 4D XCAT phantom for multimodality imaging research. Med Phys
2010;37(9):4902-4915
Figures