1067
A Multi-Resolution Approach to Estimate Cardiac and Respiratory Motion Fields for 5D Whole-Heart MR Image Reconstruction – a Proof of Concept1Diagnostic and Interventional Radiology, Lausanne University Hospital (CHUV), Lausanne, Switzerland, 2Center for Biomedical Imaging (CIBM), Lausanne, Switzerland, 3Electrophysiology and Heart Modeling Institute, IHU LIRYC, Bordeaux, France
Synopsis
Keywords: Image Reconstruction, Image Reconstruction
Motivation: Estimating cardiac and respiratory inter-bin deformation fields from 5D motion-resolved free-running data is particularly challenging due to a high level of undersampling.
Goal(s): To address this challenge through an innovative multi-resolution approach to estimate the deformation fields and reconstruct 5D motion-resolved images.
Approach: The approach consists of a sequence of compressed-sensing image reconstructions that iteratively progresses from low to high spatial resolutions, where one lower-resolution iteration’s output is exploited as input for the next higher resolution until target resolution is reached.
Results: Using optimized regularization weights, the proposed approach achieved left-ventricular ejection fraction within a 4% error margin compared the 2D cine.
Impact: This study presents a multi-resolution framework for estimating cardiac and respiratory inter-bin deformation fields aimed at improved motion-resolved whole-heart 5D-imaging. This multi-resolution compressed sensing framework has the potential to accurately estimate deformation fields and reduce compression artefacts.
INTRODUCTION
Cardiac magnetic resonance (CMR) is the gold standard for evaluating left ventricular ejection fraction (LVEF).1 Standard protocols, however, are inefficient, requiring multiple breath-holds and precise planning by skilled technicians, in addition to relying on ECG triggering.2 Such complexities may lead to potential slice misalignments.3 The free-running framework4 (FRF) overcomes these limitations by acquiring 3D whole-heart data continuously without the need for ECG placement, breathholding, or respiratory navigators, then retrospectively reconstructing fully self-gated cardiac and respiratory motion-resolved (5D) images with a compressed sensing (CS) algorithm. However, determining the optimal regularization weight is challenging, particularly without contrast agent. The regularization weights must be carefully selected to strike a compromise between residual aliasing and compression of the underlying physiological motion. To reduce the sensitivity to user-defined weights and mitigate the potential risk of compression, studies have incorporated deformation fields for inter-bin compensation of cardiac motion.5 However, estimating inter-bin deformation fields from 5D motion-resolved free-running data with high fidelity is particularly challenging due to a high level of undersampling. To address this challenge, this study adopts an innovative multi-resolution optimization approach6 to estimate the deformation fields and reconstruct the motion-resolved images. We optimize the regularization weights to prevent the compression of physiological motion and present a comparison of LVEF assessment using our framework and comparing its results against those of the conventional 2D cine method.METHODS
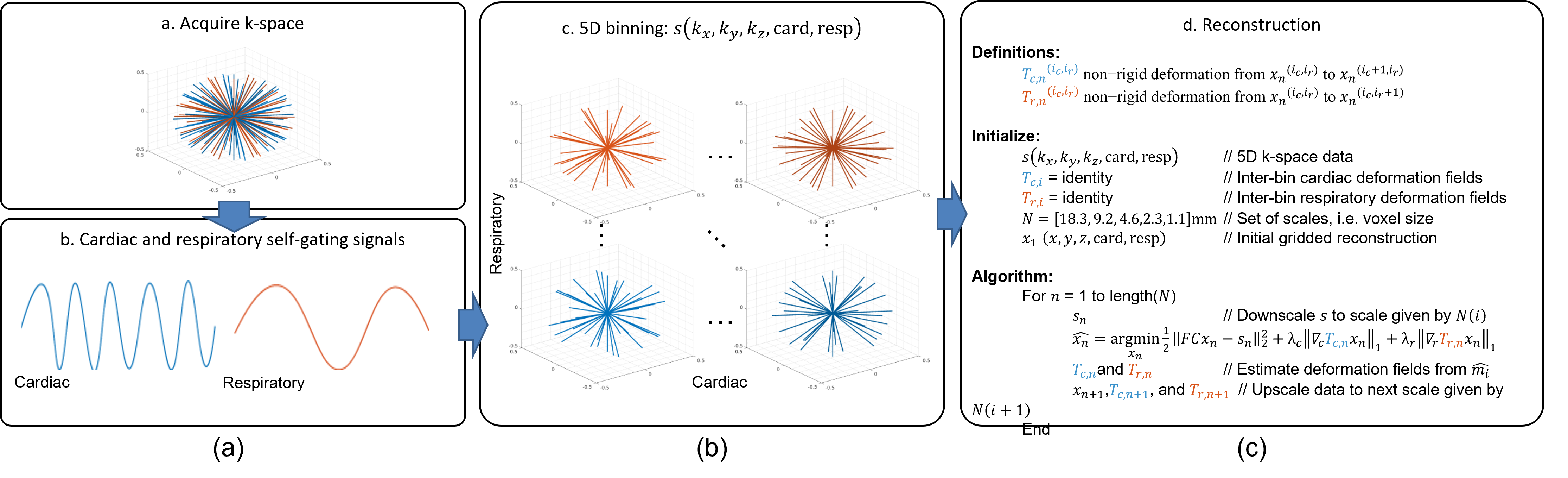
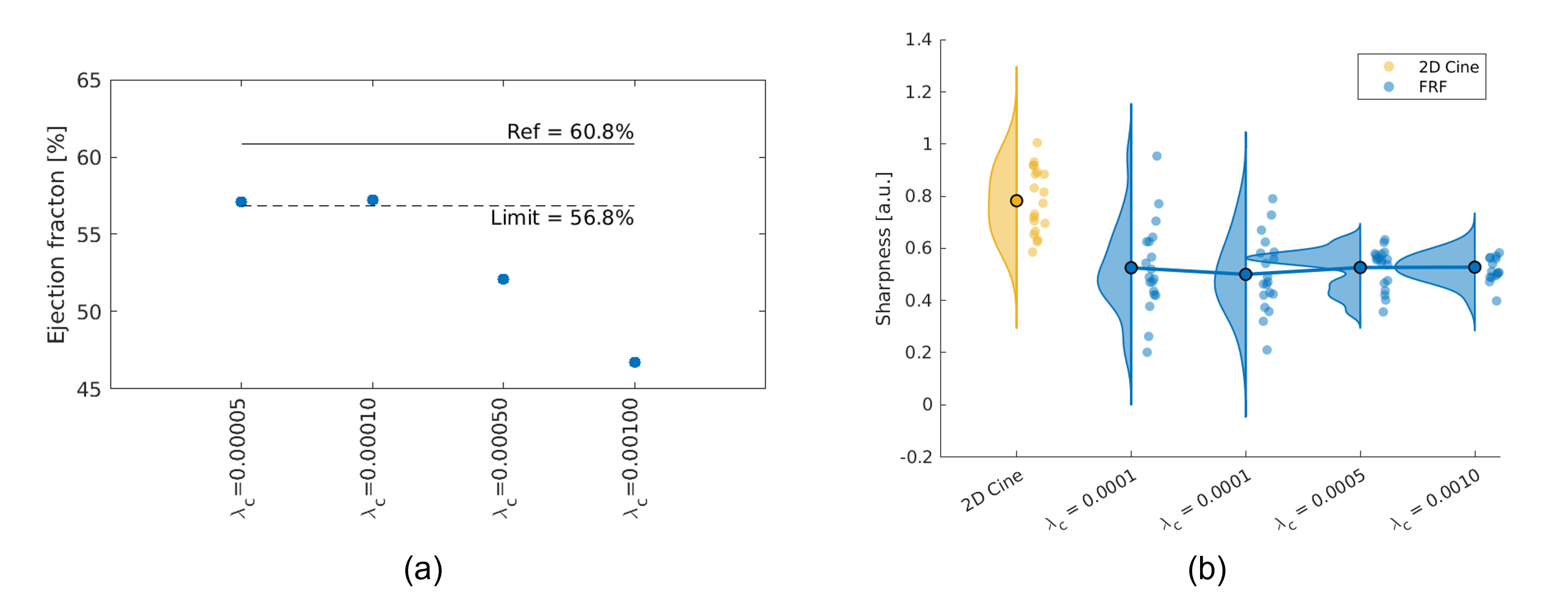
An overview of our novel multi-resolution inter-bin cardiac motion compensation framework is provided in Figure 1. First, data from four volunteers were acquired on a MAGNETOM Aera 1.5T MRI system (Siemens Healthcare) using a free-running radial 3D golden-angle bSSFP sequence7 with the following sequence parameters: (192)3 matrix, (1.1mm)3 resolution, 1.91ms/3.9ms TE/TR, a 67° RF excitation angle, and 126’478 readouts acquired continuously over 8:18 min. Second, we extracted cardiac and respiratory self-gating signals to sort the data into four respiratory bins and cardiac phases of 50ms. Finally, these free-running data were reconstructed with our proposed multi-resolution, inter-bin cardiac and respiratory motion-compensated method (Figure 1c). The method consists of a sequence of CS reconstructions that progresses from coarse to refined spatial resolutions (from 18.3mm to 1.1mm isotropic resolution). Starting with the lowest resolution, we first reconstructed the data without deformation fields (i.e., identity fields). The lowest resolution effectively minimizes undersampling artifacts and facilitates initial deformation field estimation between consecutive cardiac and respiratory phases. Each subsequent reconstruction used the previous iteration's output as the starting point by upsampling both the image and deformation fields to the next resolution. This iterative process continued until achieving the target resolution.For CS, the cardiac and respiratory regularization weights $$$\lambda_c$$$ and $$$\lambda_r$$$ were varied within the range of 0.00001 to 0.001 to assess their impact. The compression of cardiac motion was quantified by measuring the LVEF relative to a standard reference 2D cine approach, while the image quality was quantitatively assessed by measuring the blood-myocardium interface sharpness. We identified the optimal regularization weights as those that yielded the highest image quality while maintaining the error in LVEF within a 4% absolute margin when compared to the reference. Statistically significant differences in sharpness between different weights were measured using paired Student’s t-tests with a p-value less than 0.05 considered significant.
RESULTS
Figure 2 provides an animated depiction of reconstructed images at varying spatial resolutions and with different regularization weights. An increase in regularization weights typically led to a decrease in perceived noise but also to greater motion compression. This effect is more pronounced in Figure 3, where a red outline delineates the automatically segmented left ventricular volume in the final reconstructed images for enhanced visibility. A similar pattern is observable for respiratory motion (Figure 4). These qualitative findings are confirmed by quantitative analysis (Figure 5). Higher regularization weights resulted in reduced LVEF, but there was no significant difference on image sharpness within the investigated scope of weights. The optimal regularization weights that achieved both the highest image quality and an LVEF within a 4% error margin, in comparison to the 2D cine approach, were $$$\lambda_c=0.0001$$$ and $$$\lambda_r=0.0001$$$.DISCUSSION AND CONCLUSIONS
This study presents a multi-resolution approach for motion-resolved 5D whole-heart imaging. It progressively refines the resolution, allowing for the calculation of cardiac and respiratory movements between adjacent physiological phases. We optimized the regularization weights to balance image quality and physiological motion accuracy, which is crucial for the evaluation of LVEF. While incorporating deformation fields to the reconstruction helps mitigating compression artefacts, increasing the regularization weights may still possibly underestimate LVEF. Despite its promising preliminary results, this proof-of-concept needs to be further validated and tested, both on numerical data and on volunteers.Acknowledgements
Research funding for this project was provided by the Swiss National Science Foundation grants 310030_215604, 320030_143923, and 326030_150828.References
1. Curtis, J. P. et al. The association of left ventricular ejection fraction, mortality, and cause of death in stable outpatients with heart failure. J Am Coll Cardiol 42, 736–42 (2003).
2. Larson, A. C. et al. Self-gated cardiac cine MRI. Magn Reson Med 51, 93–102 (2004).
3. Chandler, A. G. et al. Correction of misaligned slices in multi-slice cardiovascular magnetic resonance using slice-to-volume registration. J. Cardiovasc. Magn. Reson. 10, (2008).
4. Di Sopra, L., Piccini, D., Coppo, S., Stuber, M. & Yerly, J. An automated approach to fully self-gated free-running cardiac and respiratory motion-resolved 5D whole-heart MRI. Magn. Reson. Med. 82, 2118–2132 (2019).
5. Asif, M. S., Hamilton, L., Brummer, M. & Romberg, J. Motion-adaptive spatio-temporal regularization for accelerated dynamic MRI. Magn. Reson. Med. 70, 800–812 (2013).
6. Royuela-del-Val, J. et al. Multiresolution reconstruction of real-time MRI with motion compensated compressed sensing: Application to 2D free-breathing cardiac MRI. in 2016 IEEE 13th International Symposium on Biomedical Imaging (ISBI) 506–509 (2016). doi:10.1109/ISBI.2016.7493318.
7. Piccini, D., Littmann, A., Nielles-Vallespin, S. & Zenge, M. O. Respiratory self-navigation for whole-heart bright-blood coronary MRI: methods for robust isolation and automatic segmentation of the blood pool. Magn. Reson. Med. 68, 571–9 (2012).
Figures