1058
Mapping spinal cord vascular reactivity and vascular territories using fMRI in highly sampled individuals1Northwestern University, Chicago, IL, United States
Synopsis
Keywords: Spinal Cord, fMRI
Motivation: Impaired vascular function in the spinal cord contributes to numerous neurological pathologies and it is important to be able to image those changes in individuals.
Goal(s): Map spinal cord vascular reactivity (SCVR) amplitude and hemodynamic delay at the individual level in two highly sampled adults.
Approach: Participants performed 18 spinal cord fMRI runs of a breath-holding task. SCVR amplitude was mapped using an end-tidal CO2 regressor and hemodynamic delay was mapped by temporally shifting that regressor.
Results: Individual SCVR amplitude and hemodynamic delay maps reveal an earlier ventral response and later dorsal response, aligning with vascular territories of the cervical spinal cord.
Impact: Individual maps of spinal cord vascular reactivity (SCVR) hemodynamic delay align with arterial territories. These are the first non-invasive maps of vascular territories in the human spinal cord. Future work will map altered SCVR in patients with neurological conditions.
Introduction
Impaired vascular function in the spinal cord contributes to neurological pathologies, e.g., spinal cord injury1 or degenerative cervical myelopathy2, and it is important to be able to characterize these changes in individual patients. In the brain, cerebrovascular reactivity and hemodynamic delay measured with fMRI have been established as robust metrics of cerebrovascular function3,4. However, similar techniques are not well established for the cord.Spinal cord vascular reactivity (SCVR), the cord’s response to a vasodilatory stimulus, can provide insight into vascular health. The associated hemodynamic delay maps can show regional variation in the timing of this vascular response. In preliminary work, we demonstrated the robust group-level (n=27) BOLD fMRI response to a hypercapnic (elevated CO2) breath-hold task in the ventral spinal cord5. However, to provide more clinically relevant information, SCVR needs to be characterized in individuals.
Here, we evaluate whether individual SCVR amplitude and delay mapping is achievable in order to assess feasibility for translational research. We accomplish this through a “highly-sampled individuals” approach6: two healthy adults undergo 18 breath-hold task fMRI runs and their SCVR amplitude and hemodynamic delay are mapped. The amount of data required for reliable SCVR estimates, and the relation of hemodynamic delay to spinal cord vascular anatomy, are assessed.
Methods
Spinal cord MRI was performed in two healthy participants (26±2y, 2F) using a 3T Siemens Prisma MRI system with a 64-channel head/neck coil and SatPadTM. Spinal cord fMRI (~C4-C8) was acquired using GRE-EPI with ZOOMit selective excitation (TR/TE=2000/30ms, voxel=1x1x3mm3, 25 axial slices, 205 volumes). Participants completed 18 breath-hold task fMRI runs spread across 3 sessions. The 6.8-min task included 7 end-expiration breath-holds (18s each) alternated with paced breathing. Structural T2-weighted scans were acquired. Exhaled CO , pulse, and respiratory effort were collected.Data were motion-corrected in-plane7, manually segmented, and spatially smoothed8 (2x2x6mm3 FWHM kernel). End-tidal CO2 (PETCO2) regressors were calculated. First-level analyses, without accounting for hemodynamic delay, modeled task (PETCO2) and nuisance (RETROICOR9,10, motion, cerebrospinal fluid) regressors. For higher-level analyses, parameter estimates were averaged across 18 runs in PAM50 template space11. A non-parametric 1-sample t-test with threshold-free cluster enhancement was used12.
To probe the reliability of SCVR estimates for different amounts of data, a split-halves approach repeatedly and randomly split 18 fMRI runs into 2 halves, comparing subsets of one half (1-9 runs) to the other 9 runs combined (spatial Pearson correlation)13.
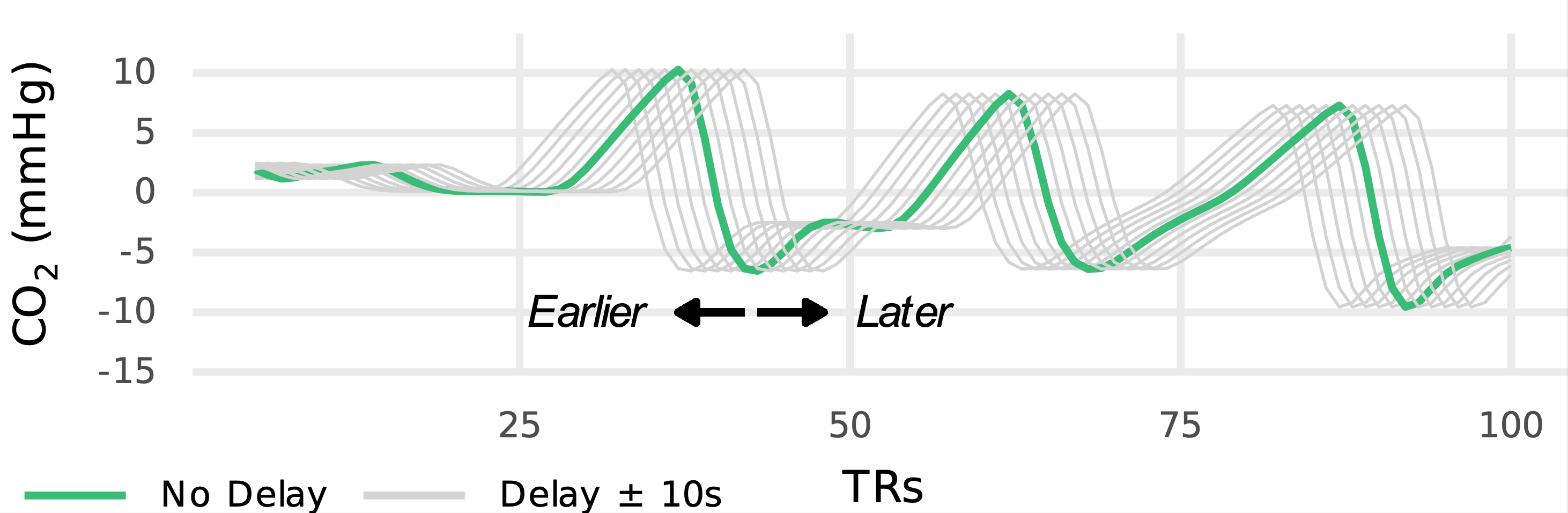
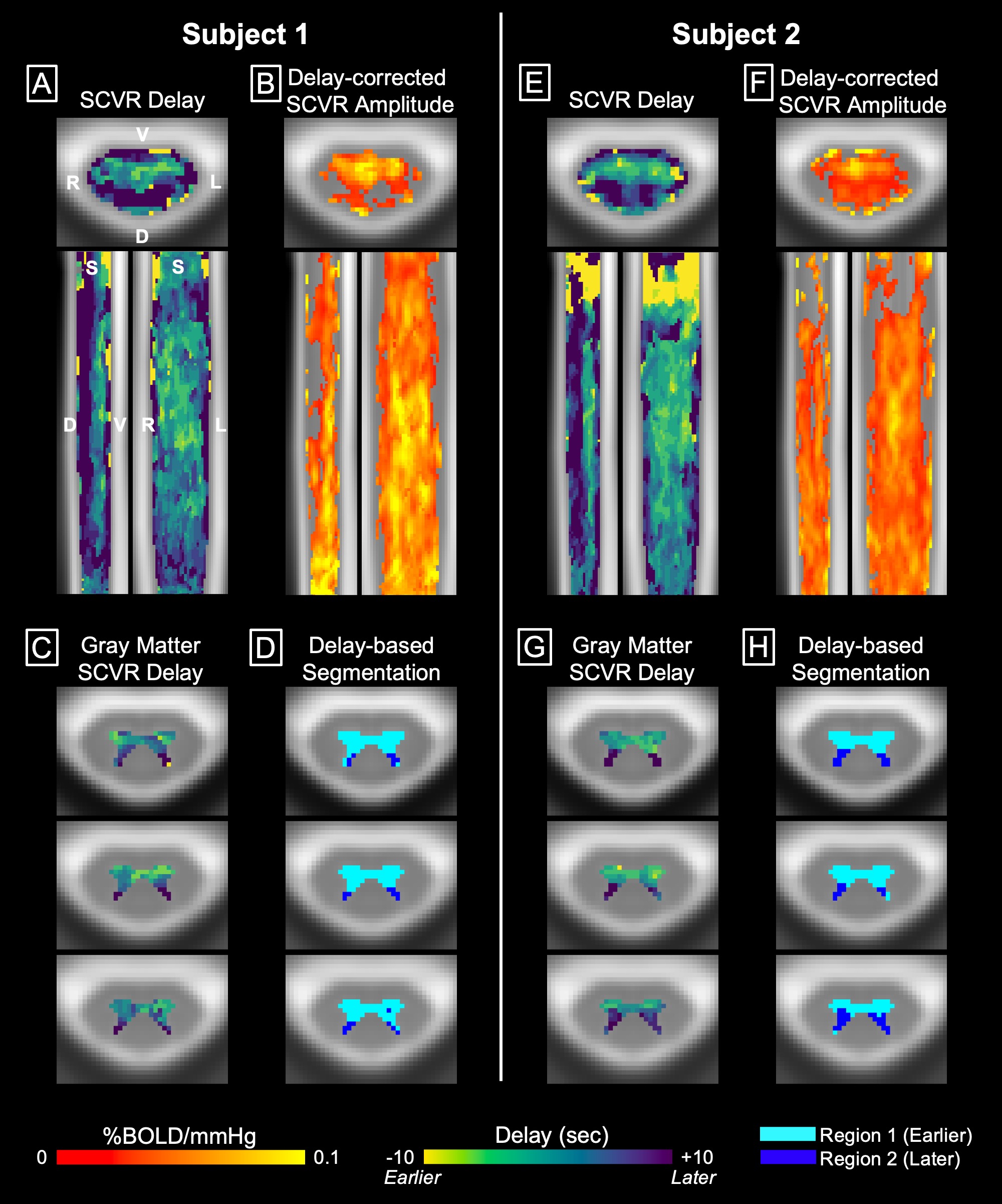
SCVR hemodynamic delay was evaluated by repeating first-level models with temporally shifted PETCO2 regressors and then repeating higher-level analyses. The delay associated with the best model fit for each voxel composes the hemodynamic delay map and was used to calculate a delay-corrected SCVR map. A histogram of gray matter delays was thresholded to estimate anterior and posterior arterial territories.
Results
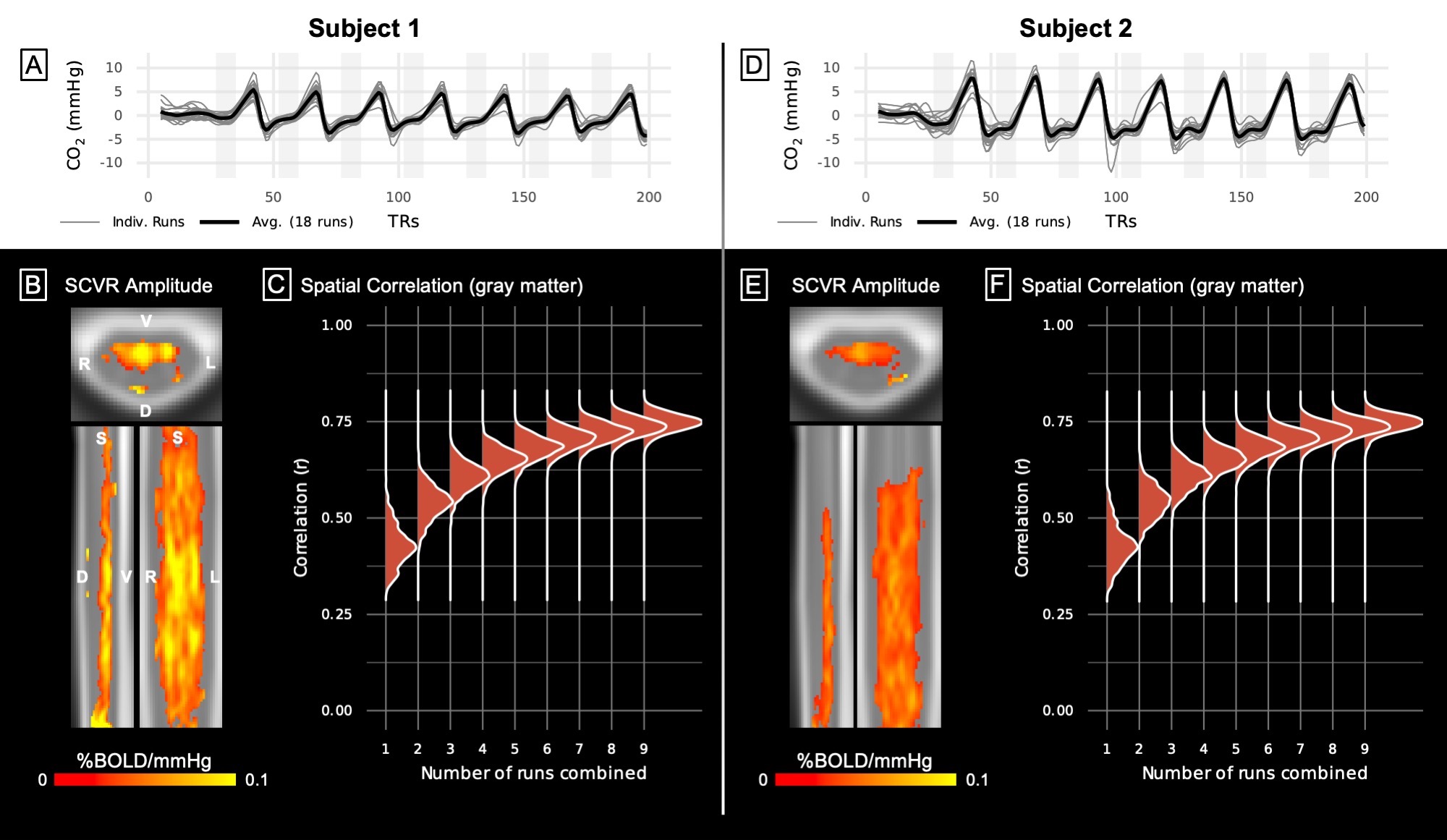
Fig1 shows the consistency of PETCO2 regressors across the 18 runs, the SCVR amplitude map, and the split halves spatial correlation. Fig2 demonstrates temporal shifting of PETCO2 regressors for delay mapping. Fig3 shows SCVR delay maps (whole cord and gray matter) and delay-corrected amplitude.Discussion
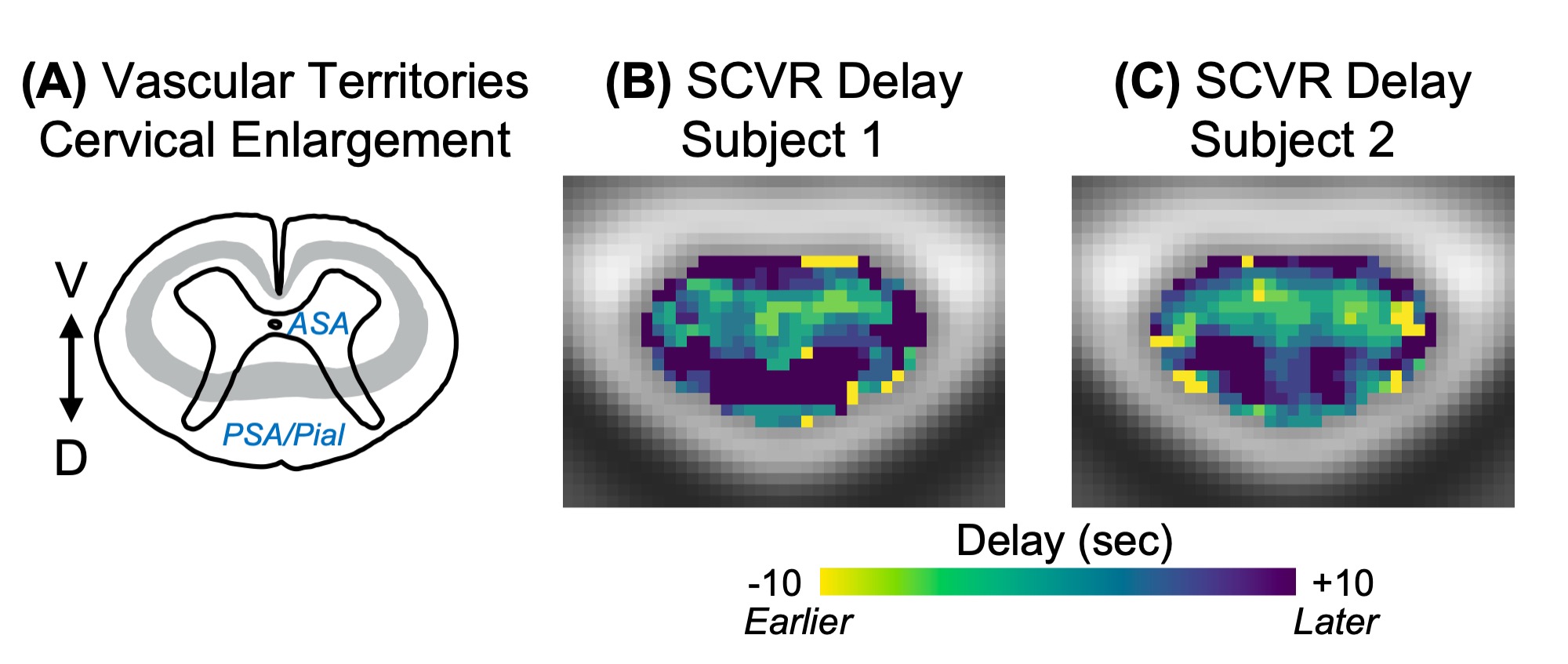
The robust SCVR response for Subjects 1 and 2 is concentrated in the ventral gray matter, as expected from previous group-level results5. These maps, however, are comprised of 18 fMRI runs from one individual. The split halves analysis plateaus at approximately 5-6 runs (spatial correlation ~0.7), indicating data from one scan session (34-41 min) may be sufficient to map SCVR in gray matter.SCVR delay maps for both subjects show an earlier response in the ventral horns and later in the dorsal horns. This may represent vascular territories of the centrifugal system (derived from the anterior spinal artery (ASA)) and the centripetal system (derived from the posterior spinal artery (PSA) and pial arterial plexus) (Fig4)1,14,15. ASA and PSA territories supply approximately the ventral 2/3 and dorsal 1/3 of the cord, respectively1,14,15. Vascular territory segmentation based on a delay threshold delineates two gray matter regions in both subjects: (1) early-responding areas of likely ASA supply (ventral horns) and (2) late-responding areas of likely PSAs supply (dorsal horns). When delay values are used to correct SCVR amplitude, significant responding voxels are more diffusely spread over both ventral and dorsal regions. This agrees with work in the brain showing increased cerebrovascular reactivity estimates after delay correction4.
Conclusion
In repeatedly-scanned individual subjects, robust SCVR maps are possible with ~40 minutes of scan data. Hemodynamic delay maps agree with known arterial territories in the cervical spinal cord, constituting the first non-invasive maps of vascular territories in the human spinal cord. In the future, this method can be applied to identify regions of impaired SCVR related to neurological pathology.Acknowledgements
This work was supported by the Center for Translational Imaging at Northwestern University. KJH was supported by NIH grants: T32EB025766, F31NS134222. Research supported by the Craig H. Neilsen Foundation (595499).References
- Martirosyan, N. L. et al. Blood supply and vascular reactivity of the spinal cord under normal and pathological conditions: A review. Journal of Neurosurgery: Spine vol. 15
- Nouri, A., Tetreault, L., Singh, A., Karadimas, S. K. & Fehlings, M. G. Degenerative cervical myelopathy: Epidemiology, genetics, and pathogenesis. Spine vol. 40
- Pinto, J., Bright, M. G., Bulte, D. P. & Figueiredo, P. Cerebrovascular Reactivity Mapping Without Gas Challenges: A Methodological Guide. Front Physiol 11, 1–19 (2021).
- Moia, S. et al. Voxelwise optimization of hemodynamic lags to improve regional CVR estimates in breath-hold fMRI. Annu Int Conf IEEE Eng Med Biol Soc 2020, 1489–1492 (2020).
- Hemmerling, K. J., Hoggarth, M. A., Sandhu, M. S., Parrish, T. B. & Bright, M. G. Spinal cord fMRI BOLD response to hypercapnic breath-hold challenge. Proceedings 29th Scientific Meeting, Organization for Human Brain Mapping (2023).
- Braga, R. M., DiNicola, L. M., Becker, H. C. & Buckner, R. L. Situating the left-lateralized language network in the broader organization of multiple specialized large-scale distributed networks. J Neurophysiol 124, (2020).
- Deshpande, R. & Barry, R. Neptune: a toolbox for spinal cord functional MRI data processing and quality assurance. Proceedings 30th Scientific Meeting, International Society for Magnetic Resonance in Medicine (2022).
- Cox, R. W. AFNI: Software for analysis and visualization of functional magnetic resonance neuroimages. Computers and Biomedical Research 29, 162–173 (1996).
- Glover, G. H., Li, T. Q. & Ress, D. Image-based method for retrospective correction of physiological motion effects in fMRI: RETROICOR. Magn Reson Med 44, 162–167 (2000).
- Brooks, J. C. W. et al. Physiological noise modelling for spinal functional magnetic resonance imaging studies. Neuroimage 39, 680–692 (2008).
- de Leener, B. et al. SCT: Spinal Cord Toolbox, an open-source software for processing spinal cord MRI data. Neuroimage 145, 24–43 (2017).
- Smith, S. M. & Nichols, T. E. Threshold-free cluster enhancement: Addressing problems of smoothing, threshold dependence and localisation in cluster inference. Neuroimage 44, 83–98 (2009).
- Laumann, T. O. et al. Functional System and Areal Organization of a Highly Sampled Individual Human Brain. Neuron 87, (2015).
- Tator, C. H. & Koyanagi, I. Vascular mechanisms in the pathophysiology of human spinal cord injury. J Neurosurg 86, (1997).
- Mautes, A. E., Weinzierl, M. R., Donovan, F. & Noble, L. J. Vascular Events After Spinal Cord Injury: Contribution to Secondary Pathogenesis Spinal Cord Injury Special Series. Physical Therapy vol. 80
Figures