1055
A Potential Substitution for Gadolinium in Brachial Plexus Magnetic Resonance Neurography: Deep Learning-Based Virtual Enhancement.1Department of Radiology, Department of Radiology,Tongji Hospital, Tongji Medical College, HUST, Wuhan, China, Wuhan, China, 2Institute of Research and Clinical Innovations, Neusoft Medical Systems Co., Ltd, Shanghai, China, Shanghai, China, 3Smart Imaging Software R&D Center, Neusoft Medical Systems Co., Ltd, Shenyang, China, Shenyang, China
Synopsis
Keywords: Peripheral Nerves, Neurography
Motivation: Contrast-enhanced Magnetic Resonance Neurography (MRN) improves visualization of brachial plexus, but gadolinium risks limit clinical use. To reduce reliance on gadolinium contrast in brachial plexus (BP) MRN, we explore deep learning's potential for virtual enhancement.
Goal(s): To investigate the feasibility of virtually enhancing brachial plexus MRN without gadolinium.
Approach: An image enhancement network based on 2.5D U-Net was trained to generate virtually enhanced BP images from non-enhancement BP images, achieving high image quality and nerve visualization.
Results: The virtual enhancement BP images showed comparable vascular suppression and image quality to gadolinium-enhanced images, demonstrating the potential for gadolinium substitution in brachial plexus MRN.
Impact: This work opens the door to safer
and more accessible BP MRN by reducing reliance on gadolinium. It may lead to
broader clinical adoption and facilitate research on non-contrast imaging
methods, benefiting both clinicians and patients.
Introduction
Magnetic Resonance Neurography (MRN) of the brachial plexus (BP) relies heavily on fat-suppressed T2-weighted imaging (T2WI) for delineating peripheral nerves1. One challenge in MRN of the brachial plexus is to distinguish nerves from adjacent blood vessels since both show high signal on T2WI. While intravenous gadolinium contrast enhances nerve visualization through shortened blood T1 and T2 relaxation times, its propensity to accumulate in the body raises concerns2-4. Recent studies showed that deep learning (DL) could reduce gadolinium dose in brain MRN enhancement5-7. However, its application in enhanced BP MRN remains unexplored. In the current study, we aim to investigate the feasibility of predicting contrast enhancement in BP MRN from non-enhanced MR images using DL.Methods
Subjects: This retrospective study included 162 patients who underwent contrast-enhanced BP MRN from May 2021 to August 2022. 3D short-tau inversion recovery (STIR) T2WI were collected respectively before and after gadolinium contrast agent injection. The first 112 cases were used to train a DL model to produce virtually enhanced images from non-enhanced data.Imaging protocol: 3D STIR T2-weighted sequences were collected in a 3T MR scanner: TR / TE = 3000/128 ms; number of slices = 36; slice thickness = 1 mm; matrix = 240 × 240; FOV = 240 × 240 mm2; number of excitations = 1; receiver bandwidth = 673 Hz/pixel; flip angle mode: T2 var.
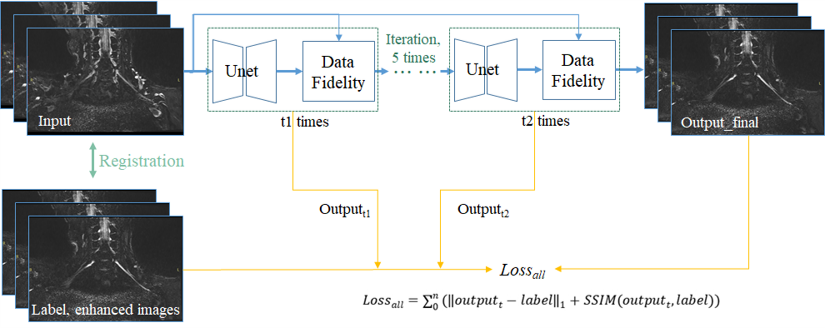
Development of the algorithm: As the input of 2.5D Unet, non-contrast images were registered to enhanced images. The image enhancement network proposed in this study were built on two blocks, i.e. data fidelity block and the 3-channel 2.5D Unet, which was adapted from the classical 2D Unet. The flowchart of the proposed image enhancement network is shown in Fig. 1.
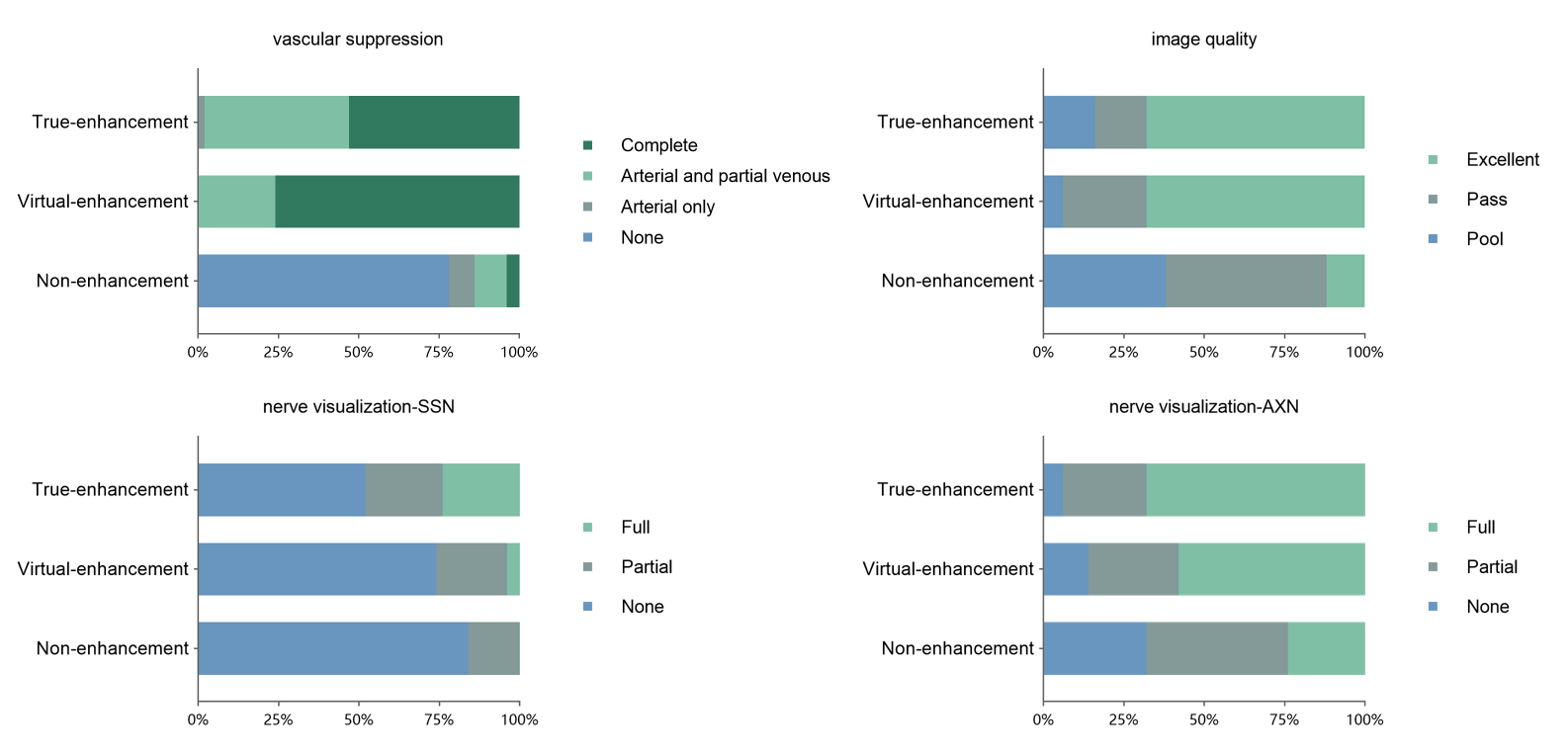
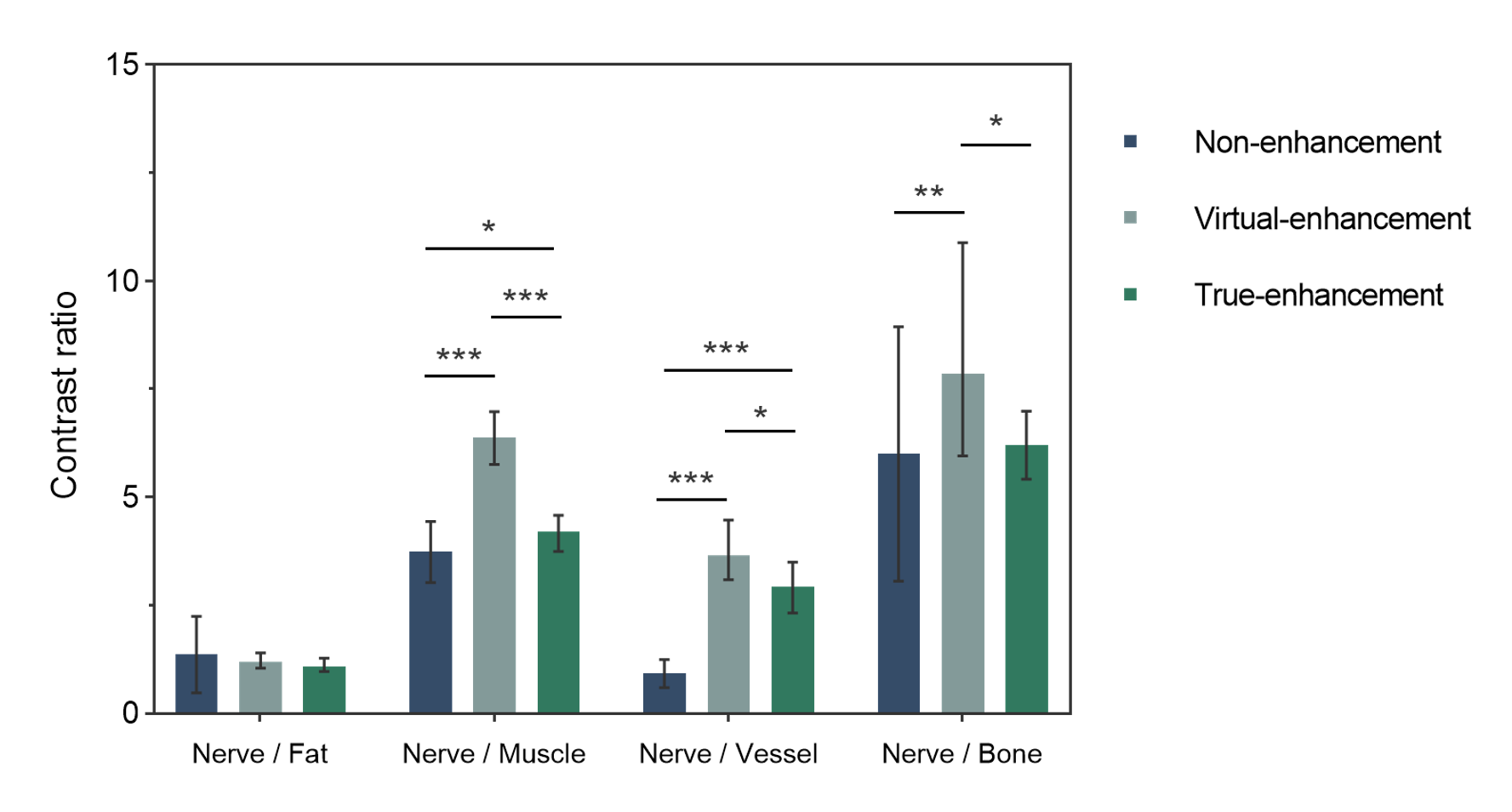
Clinical assessment: Two radiologists evaluated the remaining 50 cases on nerve visualization (0-2, none to full), vascular suppression (0-3, none to full) and image quality (0-2, poor to excellent) across unenhanced, virtually enhanced, and contrast-enhanced images8. Nerve-to-tissue contrast ratios (nerve to muscle, fat, and vessels) were calculated from manually delineated region of interests9.
Statistical analysis: Statistical analyses were performed using SPSS Statistics (version 28; IBM Corp., Armonk, NY, USA). Quantitative metrics were compared with the Wilcoxon signed rank test and independent samples t-test with significance set at P < 0.05.
Results
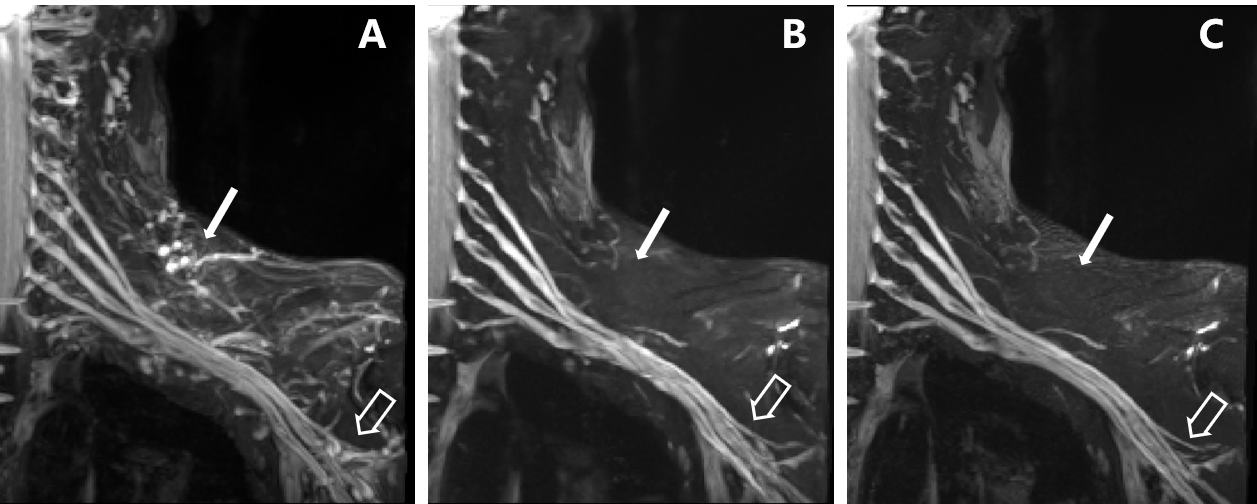
Both true and virtual-enhanced images exhibited higher vascular suppression than non-enhanced images (all p < 0.001), with no significant difference between true and virtual enhancement (p = 0.970). The image quality scores for virtual enhanced images matched those of true enhanced images (p = 0.737), and both were superior to non-enhanced images (all p < 0.001). The suprascapular nerve display rate was higher in true-enhanced than non-enhanced and virtual-enhanced images (p < 0.001 and p=0.008, respectively), which were comparable (p = 0.195). The axillary nerve display rate showed no significant difference between virtual and true enhanced images (p = 0.228), both of which exceeded non-enhanced images (p = 0.001 and p < 0.001) (Fig. 2, 3). Quantitatively, nerve-vascular, nerve-muscular and nerve-skeletal ratios were significantly higher in virtual enhanced images compared to non-enhanced and true enhanced images. No significant difference in nerve-fat ratios was found among the three image groups (Fig. 4).Discussion
In this study, we demonstrated the feasibility of using a DL method to achieve virtual enhancement effects in BP MRN without intravenous contrast administration. The images produced by the 2.5D U-Net based image enhancement network achieved comparable imaging quality and nerve visualization to true enhancement images, demonstrating its potential as a gadolinium substitute. Three-channel 2.5D U-Net model accounts for inter-layer information of input images and guarantees output continuity compared to classic 2D U-Nets10. The algorithm architecture alternates between the 2.5D U-Net block and the data fidelity block, enhancing anatomical structures while suppressing lymph node and vein signals. This iterative approach allows progressive improvement of reliable virtually enhanced images11.The model performed well for larger nerve branches like the axillary nerves, whereas its performance on smaller distal branches like the suprascapular nerve were not comparable, which is likely because these tiny nerve signals were misidentified as adjacent vessels and were suppressed by using the proposed approach. Presumably, such an issue may be attributed to the relatively small sample size in the present study, which might be improved by enriching data with multi-center BP MRN cases in future studies.
Conclusion
Overall, this study presents promising evidence that optimized DL virtual enhancement could enable comparable BP MRN visualization without gadolinium administration. Further research with collaborative multi-center data will facilitate clinical translation, thus increasing accessibility for patients unable to receive gadolinium.Acknowledgements
Thanks for all the participants.References
1. Filler A. Magnetic resonance neurography and diffusion tensor imaging: origins, history, and clinical impact of the first 50,000 cases with an assessment of efficacy and utility in a prospective 5000-patient study group. Neurosurgery. 2009;65(4 Suppl):A29-43.
2. Bjørnerud A, Vatnehol SAS, Larsson C, Due-Tønnessen P, Hol PK, Groote IR. Signal Enhancement of the Dentate Nucleus at Unenhanced MR Imaging after Very High Cumulative Doses of the Macrocyclic Gadolinium-based Contrast Agent Gadobutrol: An Observational Study. Radiology. 2017;285(2):434-444.
3. McDonald RJ, McDonald JS, Kallmes DF, et al. Intracranial Gadolinium Deposition after Contrast-enhanced MR Imaging. Radiology. 2015;275(3):772-782.
4. Murata N, Gonzalez-Cuyar LF, Murata K, et al. Macrocyclic and Other Non-Group 1 Gadolinium Contrast Agents Deposit Low Levels of Gadolinium in Brain and Bone Tissue: Preliminary Results From 9 Patients With Normal Renal Function. Invest Radiol. 2016;51(7):447-453.
5. Gong E, Pauly JM, Wintermark M, Zaharchuk G. Deep learning enables reduced gadolinium dose for contrast-enhanced brain MRI. J Magn Reson Imaging. 2018;48(2):330-340.
6. Kleesiek J, Morshuis JN, Isensee F, et al. Can Virtual Contrast Enhancement in Brain MRI Replace Gadolinium?: A Feasibility Study. Invest Radiol. 2019;54(10):653-660.
7. Luo H, Zhang T, Gong NJ, et al. Deep learning-based methods may minimize GBCA dosage in brain MRI. Eur Radiol. 2021;31(9):6419-6428.
8. Pedrick EG, Sneag DB, Colucci PG, Duong M, Tan ET. Three-dimensional MR Neurography of the Brachial Plexus: Vascular Suppression with Low-dose Ferumoxytol. Radiology. 2023;307(1):e221087. 9. Wang L, Niu Y, Kong X, et al. The application of paramagnetic contrast-based T2 effect to 3D heavily T2W high-resolution MR imaging of the brachial plexus and its branches. Eur J Radiol. 2016;85(3):578-584.
10. Ryu K, Lee C, Han Y, et al. Multi-planar 2.5D U-Net for image quality enhancement of dental cone-beam CT. PLoS One. 2023;18(5):e0285608.
11. Kofler A, Haltmeier M, Schaeffter T, Kolbitsch C. An end-to-end-trainable iterative network architecture for accelerated radial multi-coil 2D cine MR image reconstruction. Med Phys. 2021;48(5):2412-2425.
Figures