1053
Cortical Microhemorrhage Presentation of Small Vessel Primary Angiitis of the Central Nervous System1Beijing Tiantan Hospital, Beijing, China, 2MR research collaboration team, siemens healthineers, Beijing, China, 3Tianjin General Hospital, Tianjin, China, 4The First Affiliated Hospital of Fujian Medical University, Fuzhou, China
Synopsis
Keywords: Neuroinflammation, Neuroinflammation
Motivation: PACNS entails a biopsy for diagnosis, but only with an intermediate sensitivity. It is necessary to revisit PACNS with advanced imaging technique to provide a non-invasive diagnostic standard.
Goal(s): We aim to find more pathological details with enough sensitivity and specificity to provide potential biomarkers for PACNS.
Approach: 21 patients with small-vessel PACNS were included in this study. T1-MPRAGE, T2 T2*W, and SWI images were collected.
Results: Our study highlighted the image features of patients with small-vessel PACNS with coral-like signs through 7T MRI. Due to the small patient cohort, no specific clinical differences between hemorrhagic and non-hemorrhagic patients were found.
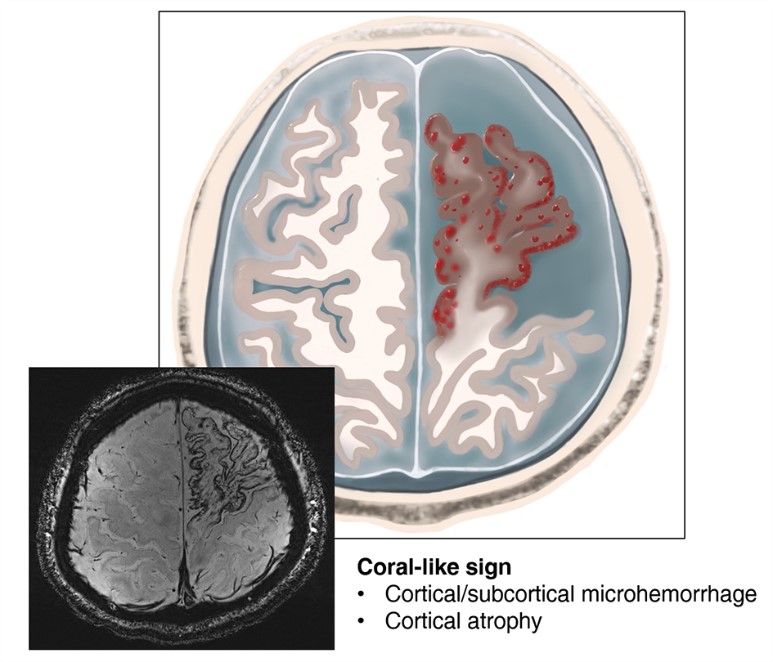
Impact: The signal characteristics of the coral-like sign represent cerebral cortical microhemorrhages with atrophy, which could be an important MRI pattern of small-vessel PACNS.
Introduction
Primary angiitis of the central nervous system (PACNS) is an inflammatory central nervous system disorder that is an unexplained vasculitis confined to the brain, spinal cord, and leptomeninges with an estimated annual incidence of 2.4 per million.1 PACNS could be categorized into angiogram-confirmed and biopsy-confirmed subtypes based on the involved vessel size.2 Biopsy-confirmed PACNS usually involves small vessels and more possibly has normal magnetic resonance angiography (MRA) and vice versa.2 Brain magnetic resonance imaging (MRI) of biopsy-confirmed PACNS are mostly abnormal; infarctions, hemorrhage, parenchymal and/or leptomeningeal enhancement, and hyperintensity on fluid attenuation inversion recovery (FLAIR)/T2-weighted sequences are usually reported.1 Due to the lack of specificity in clinical manifestations, laboratory tests, and traditional imaging examinations, the definitive diagnosis for PACNS entails a biopsy. Biopsy is the diagnostic gold standard, but it is an invasive procedure with an intermediate sensitivity ranging from 53% to 77%.3 7.0T MRI has an increased signal-to-noise ratio and advances contrast in susceptibility-sensitive sequences, such as susceptibility-weighted imaging (SWI).4 Therefore, it is necessary to revisit PACNS with advanced technology to explore potential biomarkers.Method
This is an ongoing prospective observational cohort study. We included 21 patients with small-vessel PACNS between December 2021 and July 2023. Patients who satisfied the Calabrese and Mallek criteria and underwent at least one 7.0T MRI scan were included. MRI scan was performed on a 7.0T MR system (MAGNETOM Terra, Siemens Healthcare, Erlangen, Germany) using a 32- channel Rx/8Tx head-coil (Nova Medical, Wilmington, Massachusetts, USA), including T1-weighted magnetization-prepared rapid gradient echo imaging (T1-MPRAGE), T2 star weighted imaging (T2*W), and susceptibility-weighted imaging (SWI). The neuroimages were independently reviewed by two experienced radiologists. Clinical data were extracted from electronic patient records. Categorical variables were presented as frequencies and percentages. The t-test, Mann-Whitney U test, and Fisher’s exact test were performed to compare demographic, clinical, laboratory, and MRI differences between the two subgroups. Statistical significance was defined as a two-sided p-value of < 0.05.Result
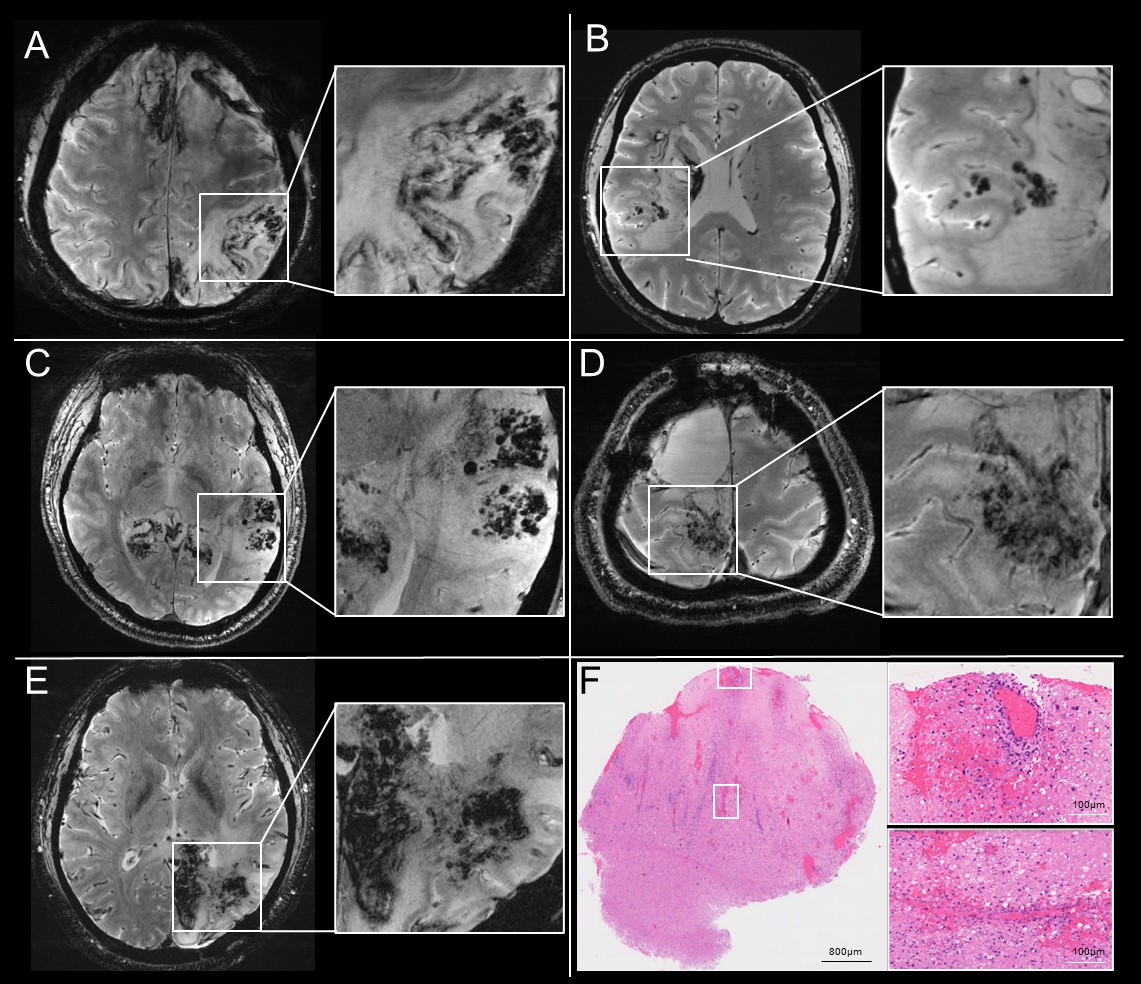
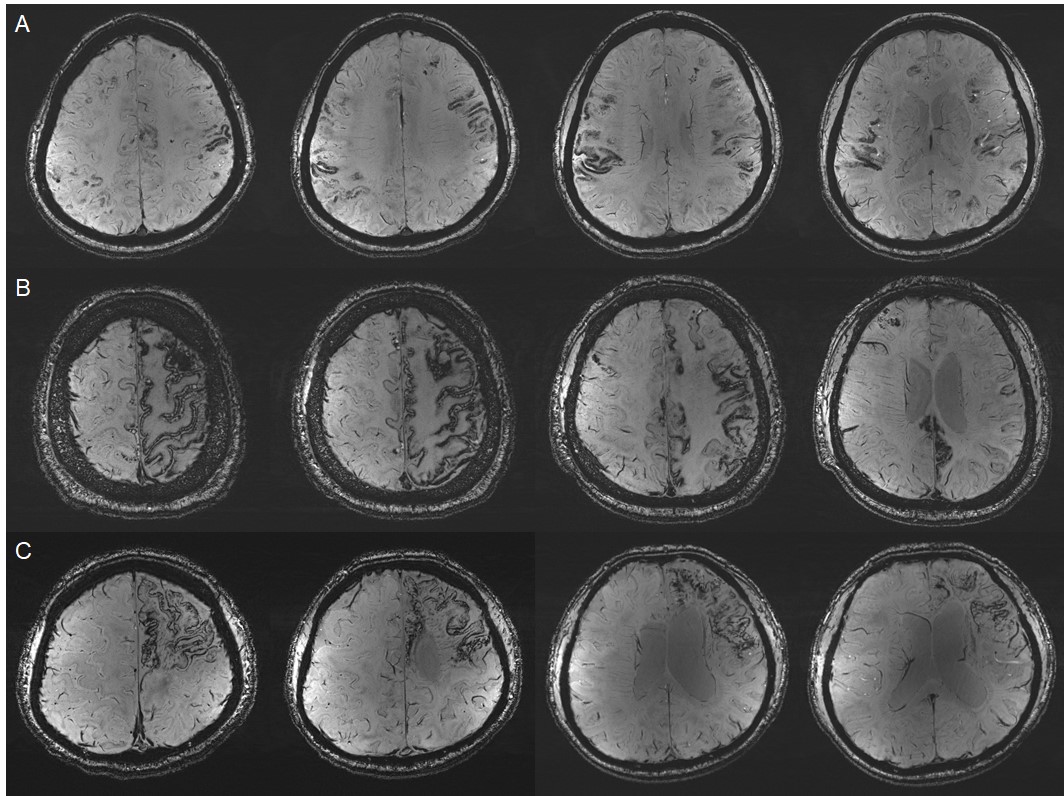
Twelve patients (57.14 %) had cerebral cortical microhemorrhages with atrophy. MRI microhemorrhage patterns were described in detail according to the gradient echo sequence, and we named this the coral-like sign (Figure 1). The age of onset of patients with cortical microhemorrhage (32.17 ± 8.33 years) seemed younger than that of patients without cortical microhemorrhage (42.11 ± 14.18 years) (p = 0.085). Figure 2 showed petechial microhemorrhage in cortical and subcortical lesions. Figure 3 showed gyriform microhemorrhage of PACNS. Moreover, the cerebral lesions of cortical microhemorrhagic PACNS patients have a greater propensity toward bilateral lesions (p = 0.03).Discussion
In this study, we propose that cortical microhemorrhage with atrophy as a characteristic pattern of small-vessel PACNS. The proportion of microhemorrhages in patients with biopsy-confirmed PACNS was 57.14% in our cohort. The mean age at onset was lower in patients with cortical microhemorrhage than in those without cortical microhemorrhage. The lesions were prone to be bilateral. Through literature research, our investigation is the first study to display 7.0T brain MRI images of PACNS, though with small cohort. As a preliminary study, we temporarily did not include control groups, and this will be included in the future. Also, we plan to match histological findings with MR images, to see whether more pathological information will be uncovered. Our research is a promising start for detailed studies of PACNS patients.Conclusion
Our study found cortical microhemorrhage with atrophy is a typical presentation of small-vessel PACNS. This is a first-realized radiographic finding and we named it as coral-like sign.Acknowledgements
No acknowledgement found.References
1. Salvarani C, Brown RD, Jr., Calamia KT, et al. Primary central nervous system vasculitis: analysis of 101 patients. Ann Neurol. 2007 Nov;62(5):442-51.
2. Beuker C, Strunk D, Rawal R, et al. Primary Angiitis of the CNS: A Systematic Review and Meta-analysis. Neurol Neuroimmunol Neuroinflamm. 2021 Nov;8(6).
3. Paul SA, Roy D, Mondal GP, et al. Primary angiitis of central nervous system - A challenging diagnosis. J Neuroimmunol. 2022 May 15;366:577844.
4. Burkett BJ, Fagan AJ, Felmlee JP, et al. Clinical 7-T MRI for neuroradiology: strengths, weaknesses, and ongoing challenges. Neuroradiology. 2021;63(2):167-77.
Figures