1039
Non-invasive magnetic resonance imaging agent for in-vivo detection of cardiac fibrosis.1Biomedical Engineering, University of Toronto, Toronto, ON, Canada, 2Ted Rogers Centre for Heart Research, University of Toronto, Toronto, ON, Canada, 3Electrical and Computer Engineering, University of Toronto, Toronto, ON, Canada
Synopsis
Keywords: Contrast Agents, Molecular Imaging, fibrosis, myocardium, hypertension, diabetes
Motivation: Fibrosis is a progressive pathological process that contributes to 45% of deaths worldwide and is associated with the accumulation of collagen and the destruction of tissue architecture. While progression of fibrosis is often slow, early detection is difficult, leading to intervention at late stage when transplant may be the only option.
Goal(s): Establish a targeted MRI contrast agent for detecting early fibrosis.
Approach: Validation of agent sensitivity in-vivo with isoproterenol-induced heart fibrosis in a mouse model.
Results: Our novel fibrosis agent surpassed the sensitivity and specificity of Gd contrast enhanced T1 mapping for detecting mild cardiac fibrosis.
Impact: This project sets out to create a new, hitherto inaccessible window on fibrogenesis, providing a new paradigm for diagnosing patients with fibrosis and the study of anti-fibrosis intervention before fibrosis becomes extensive and irreversible.
Introduction
All life-sustaining organs are susceptible to fibrosis, a progressive and intractable condition characterized by scarring and contributing to 45% of global deaths.1 Despite its ubiquity, fibrosis is notoriously difficult to detect without resorting to highly invasive biopsies usually performed at the advanced stages of disease. By this point, the tissue is irreversibly damaged by extensive scarring, and organ transplant may be the only treatment option.1,2 There is evidence, however, that fibrosis may be successfully stopped or reversed with intervention at earlier stages.3,4 However, these potentially lifesaving interventions cannot be effectively implemented or studied without improving our current methods of detection. To improve the prognosis for patients, we require a non-invasive technology to detect early and active fibrosis in deep tissues. Conventional imaging methods for “detecting” fibrosis is non-specific, with detection limited to the dense scars of late fibrosis or elevated extracellular volume left by dead cells.5 Attempts to specifically target collagen, the primary component of fibrosis, have also failed to translate clinically, due to the potential release of toxic gadolinium (Gd) metal used in current MRI contrast agents.6 Therefore, a technique that safely targets collagen, especially in early fibrosis and active, ongoing fibrogenesis, is urgently needed.Methods
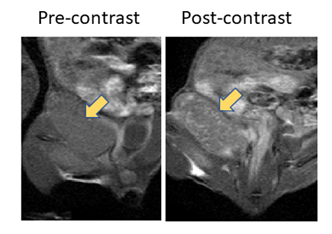
Contrast enhancement and some collagen affinity of our unfunctionalized porphyrin precursor (MnP) was previously found in a pilot in-vivo study of breast cancer in a rat (Figure 1). The resulting enhancement of collagen-rich tumor extracellular matrix represents the minimum contrast increase expected from this un-functionalized base porphyrin. To further improve its affinity to collagen, we conjugated this porphyrin to a proprietary collagen-binding moiety 33 to further improve sensitivity to fibrosis. To validate the collagen-binding ability of Fibrosis Agent, the agent was incubated with type I collagen gels at concentrations ranging from 1.2 to 480 µM for 24 hours before being scanned on a 3T preclinical scanner (MR solutions, Guildford, UK). Affinity curves were later generated by incubating collagen films in fibrosis agent solutions for 24 hours before measuring remaining concentration of Mn in solutions by Inductively induced plasma optical emission (Thermo Scientific, Madison, Wisconsin, USA). A Scatchard plot was used to determine affinity of the fibrosis agent and the unfunctionalized precursor. To test feasibility of detecting mild cardiac fibrosis In-vivo, we used the β-andrenergic agonist isoproterenol hydrochloride to trigger an immune response against the heart leading to mild cardiac fibrosis in C57BL/6 mice. A single high dose of Isoproterenol was given followed by imaging with fibrosis agent or Gadobutrol at either 2, 6 or 15 weeks. T1 map of the heart was acquired longitudinally to monitor changes in the T1 value of the left ventricular wall. Respiratory gating with a T1- weighted FLASH sequence with the following parameters were used: TE=min; TR=7ms; FA=[2o, 5o,10o, 15o, 20o]; FOV= 50 mm; reconstruction with Retro8.Results and Discussion
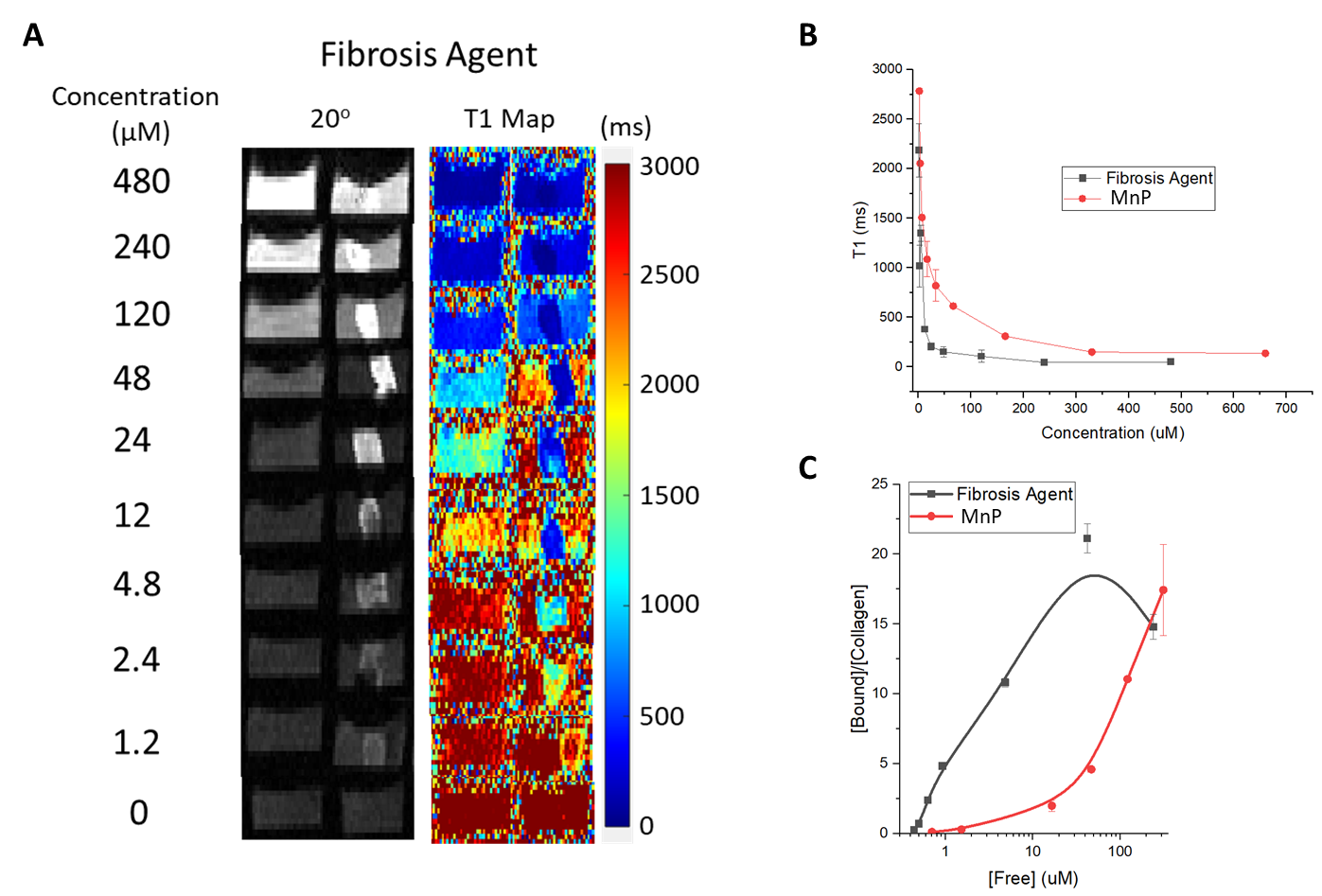
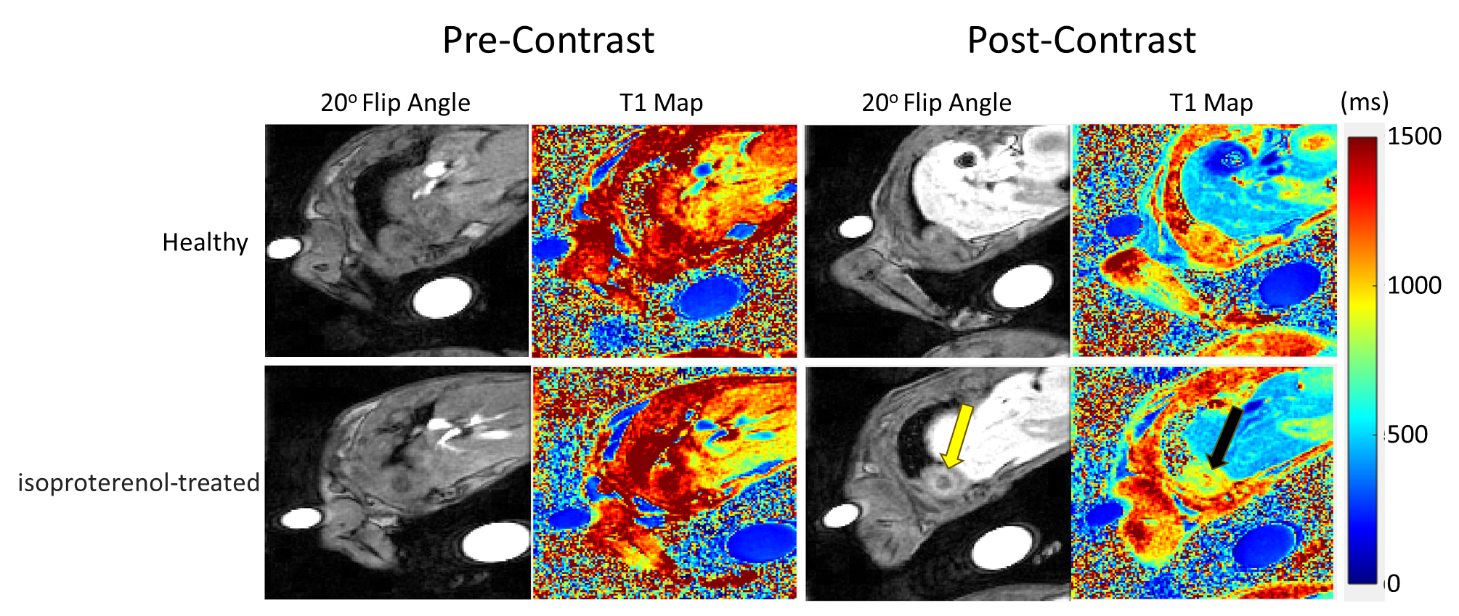
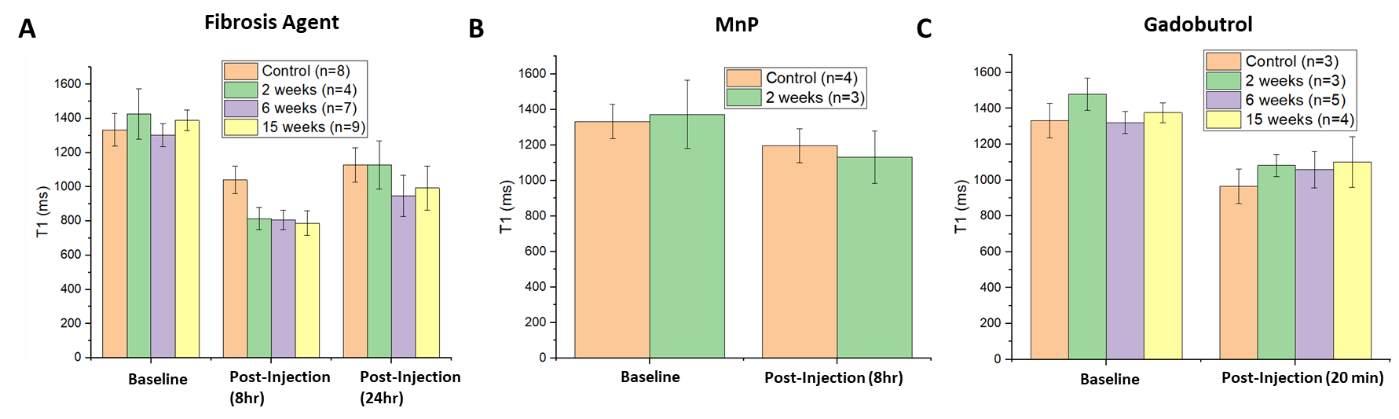
In-vitro T1 contrast enhancement of collagen gels incubated with a range of fibrosis agent concentrations is shown in Figure 2A. Fibrosis agent conferred bright contrast to collagen gels across all concentrations tested; saturation occurred when concentrations exceeded 100 µM. Furthermore, our fibrosis agent provided significant contrast enhancement down to concentrations as low as 1.2 µM. These T1 values obtained for fibrosis agent enhanced collagen gels are plotted in Figure 2B for direct comparison to the unfunctionalized porphyrin precursor MnP. These results show that functionalization of MnP with our proprietary fibrosis binding group enhances T1 contrast of collagen gels. This is consistent with affinity curves depicted in Figure 2C, which shows that fibrosis agent affinity for collagen I was enhanced by orders of magnitude (dissociation constant 4.7 ± 1.7 µM versus >230). In-vivo study of fibrosis agent in isoproterenol-treated mice revealed significant contrast enhancement in the myocardium compared to healthy controls (Figure 3). Quantitative T1 analysis of fibrosis agent’s enhancement of the myocardium is shown in Figure 4A – here, T1 was significantly reduced in all isoproterenol-treated mice groups at 8 hours post-contrast. Results obtained with unfunctionalized porphyrin and Gadobutrol found no significant T1 reduction in the myocardium of isoproterenol-treated mice compared to controls.Conclusion
We have developed a novel MRI contrast agent for imaging mild cardiac fibrosis. In-vitro experiments demonstrated a high sensitivity to collagen. Most notably, significant T1 reduction was achieved in isoproterenol-induced heart injury, where conventional Gadobutrol failed to detect fibrosis.Declaration of Conflicts
A provisional patent has been filed on this invention: “Manganese bifunctional chelating agent conjugation platform for targeted MR imaging”. (GB2216233.3, filed 2022-11-01).Acknowledgements
No acknowledgement found.References
1. Wynn, T. A. Cellular and molecular mechanisms of fibrosis. J. Pathol. 214, 199–210 (2008).
2. Zeisberg, M. & Kalluri, R. Cellular mechanisms of tissue fibrosis. 1. Common and organ-specific mechanisms associated with tissue fibrosis. Am. J. Physiol. Cell Physiol. 304, C216-25 (2013).
3. Jun, J.-I. & Lau, L. F. Resolution of organ fibrosis. J. Clin. Invest. 128, 97–107 (2018).
4. Fioretto, P., Steffes, M. W., Sutherland, D. E., Goetz, F. C. & Mauer, M. Reversal of lesions of diabetic nephropathy after pancreas transplantation. N. Engl. J. Med. 339, 69–75 (1998).
5. Horowitz, J. M. et al. Evaluation of hepatic fibrosis: a review from the society of abdominal radiology disease focus panel. Abdom. Radiol. (New York) 42, 2037–2053 (2017).
6. Caravan, P. et al. Collagen-targeted MRI contrast agent for molecular imaging of fibrosis. Angew. Chem. Int. Ed. Engl. 46, 8171–8173 (2007).
Figures