1035
A 60-channel high-density flexible receive array for pediatric abdominal MRI1Stanford University, Stanford, CA, United States, 2GE HealthCare, Aurora, OH, United States
Synopsis
Keywords: RF Arrays & Systems, RF Arrays & Systems
Motivation: Conventional MRI coils offer suboptimal parallel imaging performance for young children.
Goal(s): Our goal was to enhance imaging acceleration by dedicated flexible high-density coil design for pediatric patients at 3T.
Approach: We design, construct, and evaluate a highly flexible small element dense array constituted by dual turn loops with minimum inter-component interference layout design.
Results: Both phantom and in-vivo studies demonstrated superior parallel imaging performance using the proposed coil.
Impact: A dedicated high-channel count coil that allows highly localized coil sensitivities by minimum interference layout design may benefit small pediatric patients.
Introduction
Pediatric body MRI is a compelling imaging modality due to superior soft tissue contrast, functional/quantitative capabilities, and lack of ionizing radiation1. Despite its potential benefits in imaging applications, it is underutilized because of challenges associated with widely varying patient sizes, intricate imaging parameters, and lack of dedicated coil arrays in clinical use2. In line with recent coil technologies3,4, we introduce a prototype design of a 60-channel flexible blanket-type array to accelerate pediatric body imaging. The small loop array (SLA) design includes optimal coil component placement on a relatively small layout, cable assembly management, and preamp feed-board allocation. The proposed SLA performance is presented in terms of g-factor and SNR map as a function of 2D acceleration using an anthropomorphic pediatric phantom, compared to a commercial benchmark (BM) coil (Air coil, GE Healthcare). In addition, preliminary in-vivo images were presented in comparison to BM under IRB approval.Methods
SLA was designed and constructed on a flammability-rated flexible fabric, which consists of two independent 30-channel layout parts. SLA anterior-posterior pair provides 33cm x 24cm x 10cm (SI x RL x AP) FOV coverage in Figure 1 (a). A 30-channel layout in Figure 1 (b) contains 5 x 6 identical loop elements, critically overwrapped with neighboring elements. RF cables from each feed-board were routed through the center region of the loop elements toward the interface board to minimize EM field interaction with loop conductors. A total of 30 cables are bundled equally in five miniature bobbin traps to suppress common mode interference, shown in the left side of the photograph shown in Figure 1 (b). The array element forms a dual-turn circular loop sized 5.7cm diameter (edge to edge) using a lightweight and flexible PCB for the desired loading. The loop interfaces a small footprint preamp feed-board which integrates three series tuning capacitors and input balun in Figure 1 (c). This miniaturized integrated architecture provides the durability of a flexible loop as well as saves room for feed-board allocation within limited layout space. The feed-board was placed in the center region of the loop to minimize field interaction with the tuned loop.Phantom experiments were performed on a 3T MR750w scanner (GE Healthcare) to access the parallel imaging performance with SLA and BM (Air medium, GE Healthcare). SLA covers the anthropomorphic phantom in the anterior-posterior pair in Figure 1 (a) and the BM coil was folded to do the same. To access parallel imaging performance, 1/g-factor maps were calculated with coil sensitivities estimation by ESPIRIT algorithm5 as a function of 2D acceleration in Figure 2. In addition, SENSE reconstructed SNR maps on a coronal plane and the optimum SNR maps on an axial plane were calculated6 and compared in Figure 3 and Figure 4, respectively.
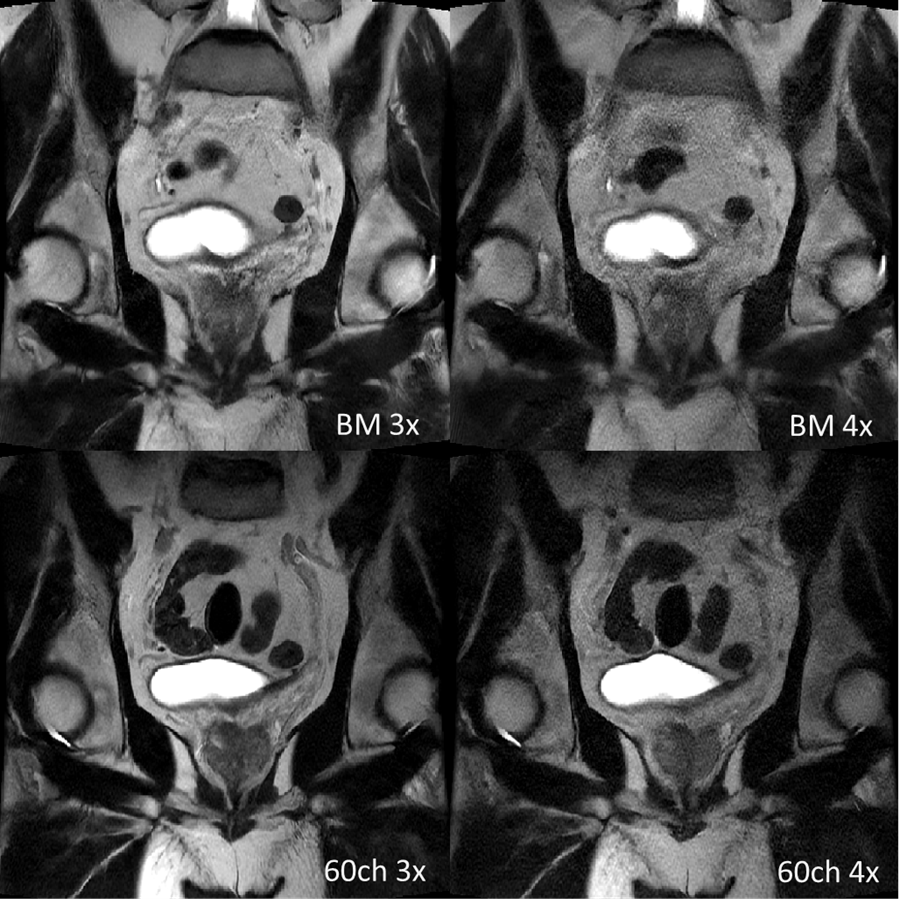
Normal adult volunteer pelvis images were obtained using SLA and BM with acceleration 3 and 4 along SI phase encoding direction in Figure 5. SLA was arranged in an anterior-posterior combination (60ch), and BM was arranged with Air medium and large (GE Healthcare) together to form anterior-posterior combinations (41ch), which is typically used in our institution. SSFSE T2 weighted sequence was used with Matrix size 386x256, FOV 24cm x 24cm, TE 132ms/131ms (3x/4x), TR 822ms/666ms, Slice thickness 4mm, Number of slices 7, Number of averages 1.
Results
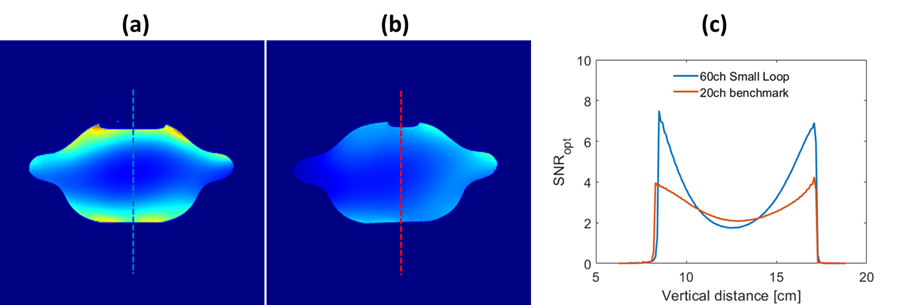
1/g-factor map in Figure 2, demonstrates that the parallel imaging performance using SLA (a) is superior to BM’s (b) at higher accelerations, which is attributed to its highly localized coil sensitivities in the region of interest. It is obvious to see the larger noise degradation at higher reductions under RL direction in both figures (a) and (b), noting that there are fewer elements in that direction. SNR maps using SLA in Figure 3 (a) also present superior imaging quality at higher accelerations (b). The optimum SNR map with SLA and its vertical profile exhibits a typical depth-dependent sensitivity profile, with higher sensitivity in the periphery and lower in the center region in Figure 4. The in-vivo images using SLA at 4x result in slight image quality degradation as that at 3x, whereas image quality with BM degrades significantly at 4x, which exhibits better acceleration performance using SLA as in the phantom results.Discussion and conclusion
Suboptimal coil scenarios in pediatric applications often limit efficient imaging procedures. A dedicated flexible small loop coil design that conforms to imaging subjects demonstrated superior parallel imaging performance than BM according to phantom and preliminary in-vivo studies. We anticipate further in-vivo pediatric volunteer scans and evaluations to assess the full potential of the proposed coil soon.Acknowledgements
We thank GE Healthcare for research support and NIH 1RO1 EB019241
References
1. Olsen OE. Practical body MRI - A pediatric perspective. Eur J Radiol. 2008 Nov;68(2):299-308.
2. Vasanawala, S. S., & Lustig, M. (2011). Advances in pediatric body MRI. In Pediatric radiology: Vol. 41 Suppl 2.
3. Darnell D, Truong TK, Song AW. Recent Advances in Radio-Frequency Coil Technologies: Flexible, Wireless, and Integrated Coil Arrays. J Magn Reson Imaging. 2022 Apr;55(4):1026-1042.
4. Ohliger MA. Invited Commentary: MRI Radiofrequency Coils-Current Uses and Future Innovation. Radiographics. 2022 May-Jun;42(3):E100-E101
5. Uecker M, Lai P, Murphy MJ, Virtue P, Elad M, Pauly JM, Vasanawala SS, Lustig M. ESPIRiT--an eigenvalue approach to auto calibrating parallel MRI: where SENSE meets GRAPPA. Magn Reson Med. 2014 Mar;71(3):990-1001.
6. Kellman P, McVeigh ER. Image reconstruction in SNR units: a general method for SNR measurement. Magn Reson Med. 2005 Dec;54(6):1439-47.
Figures
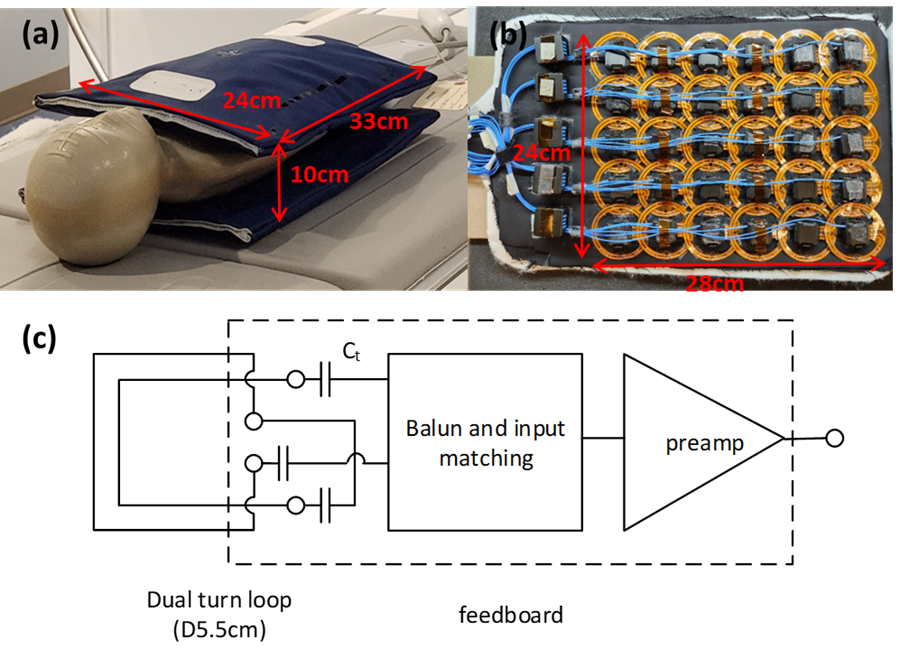
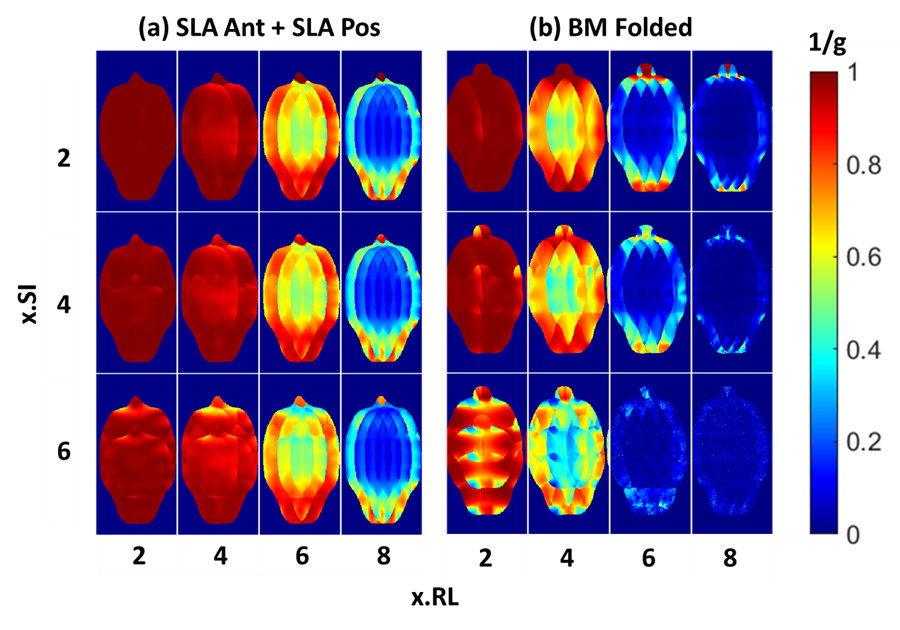
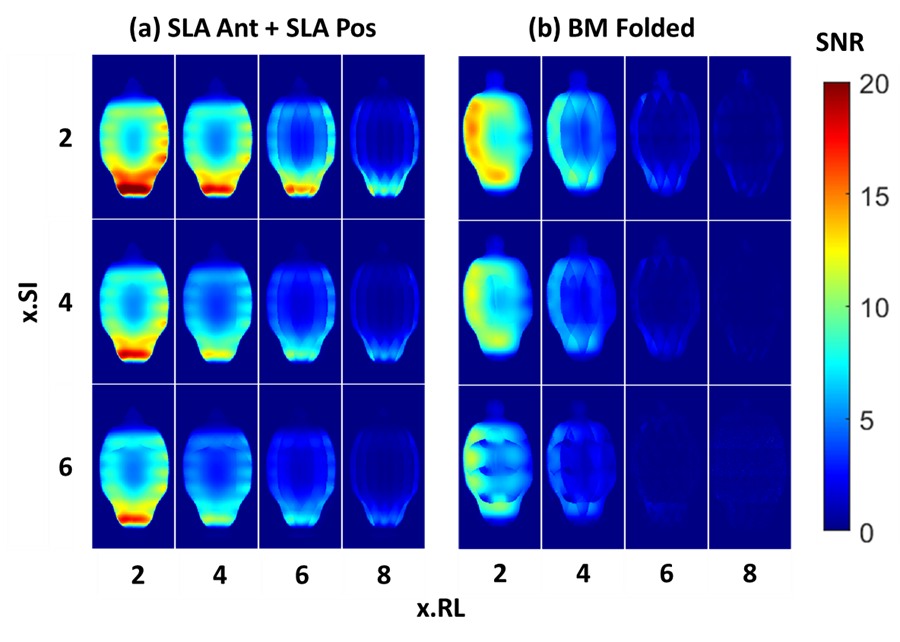
Figure 3. SENSE reconstructed SNR maps as a function of 2D accelerations at the center coronal plane of pediatric torso phantom with SLA pair (a) and with folded BM (b), showing better image quality in (a) than in (b) at higher accelerations.