1027
Functional Kinematic Assessment of the Wrist Using Volumetric Dynamic MRI1The Bernard and Irene Schwartz Center for Biomedical Imaging, Department of Radiology, New York University Grossman School of Medicine, New York, NY, United States, 2Center for Advanced Imaging Innovation and Research (CAI2R), Department of Radiology, New York University Grossman School of Medicine, New York, NY, United States, 3Vilcek Institute of Graduate Biomedical Sciences, New York University Grossman School of Medicine, New York, NY, United States, 4Department of Computer Science and Engineering, NYU Tandon School of Engineering, Brooklyn, NY, United States, 5Department of Computer Science and Engineering, New York University Tandon School of Engineerin, Brooklyn, NY, United States
Synopsis
Keywords: Segmentation, Joints, Wrist
Motivation: Dynamic imaging can be useful for the evaluation of wrist instability.
Goal(s): To propose a semi-automatic approach for carpal bones segmentation on 3D dynamic wrist MRI to enable kinematic assessment.
Approach: We segmented carpal bones on a high-resolution 3D static MRI, registered it to a template created from the dynamic frames, and transferred back the segmentations onto individual 3D dynamic volumes. Bones surfaces were reconstructed and the reproducibility of motion patterns was assessed on repeated scans.
Results: Our proposed image processing and visualization pipeline enables semi-automatic segmentation of carpal bones and provides a framework for qualitative and quantitative analysis of wrist kinematics.
Impact: This work demonstrates semi-automatic segmentation of real-time dynamic MRI of the wrist to extract carpal bones motion. It could be used for quantitative kinematic analysis to detect and characterize wrist abnormalities.
Introduction
Static MRI examination of the wrist, as performed routinely in clinical practice, provides excellent spatial resolution and contrast for characterizing bone and soft tissue1. However, initial stages of wrist instabilities often manifest only during active motion, for example with snapping or sudden changes in the intercarpal alignment, and do not show visible abnormalities on routine static examinations2. Therefore, dynamic volumetric wrist imaging with high temporal spatial resolution is desirable for patients experiencing pain during wrist movement. A novel approach was recently proposed to obtain real-time dynamic 3D wrist data during ulnar-radial deviation3. The goal of this work is to introduce an image processing pipeline to analyze 3D dynamic MRI of the wrist for functional kinematic assessment.Methods
Experiments:Four healthy volunteers (after obtaining informed consent) were scanned on a clinical 3T scanner (MAGNETOM Prisma, Siemens Healthineers). A radial GRE sequence was used to obtain high-resolution static 3D wrist images. The technique proposed by Zi et al.3 was used to acquire two consecutive 3D dynamic wrist datasets for each subject (to assess reproducibility) during real-time ulnar-radial deviation.
Image Processing:
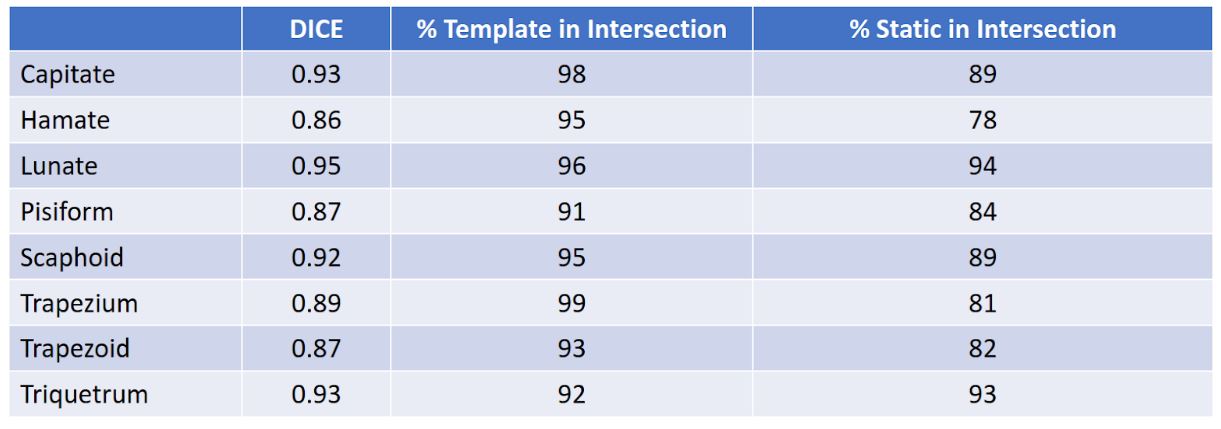
To facilitate segmentation, we created a template image for each acquisition, using all dynamic frames to compute a set of diffeomorphisms using LDDMM with cross-correlation similarity metric4. The template was spatially registered to the corresponding static MRI. We segmented each of the 8 carpal bones in the static 3D volume using edge-attraction to model an active contour model5 . We performed the same segmentation on the template image and used the DICE coefficient between segmentations as a proxy-metric to validate the registration. We then propagated the segmentation from template space directly back to image space using the inverse of the calculated diffeomorphisms to automatically segment all the dynamic frames.
The diffeomorphisms tend to non-linearly deform the individual bones so we performed an additional poly-rigid registration to enforce structural consistency across time. Fixing the first dynamic 3D frame as the baseline, we rigidly align all other frames to it with a RANSAC6 based registration using FPFH7 feature vectors extracted from the bone surface. The registration was further refined using ICP8. This secondary registration, implemented with Open3D9, ensures that any trajectory based analysis performed on these bones isolates only the desired rigid body kinematics of the wrist and are not affected by residual non-rigidities introduced by non-linear deformations. Finally, we computed the rigid body parameters for each bone segmentation.
Results
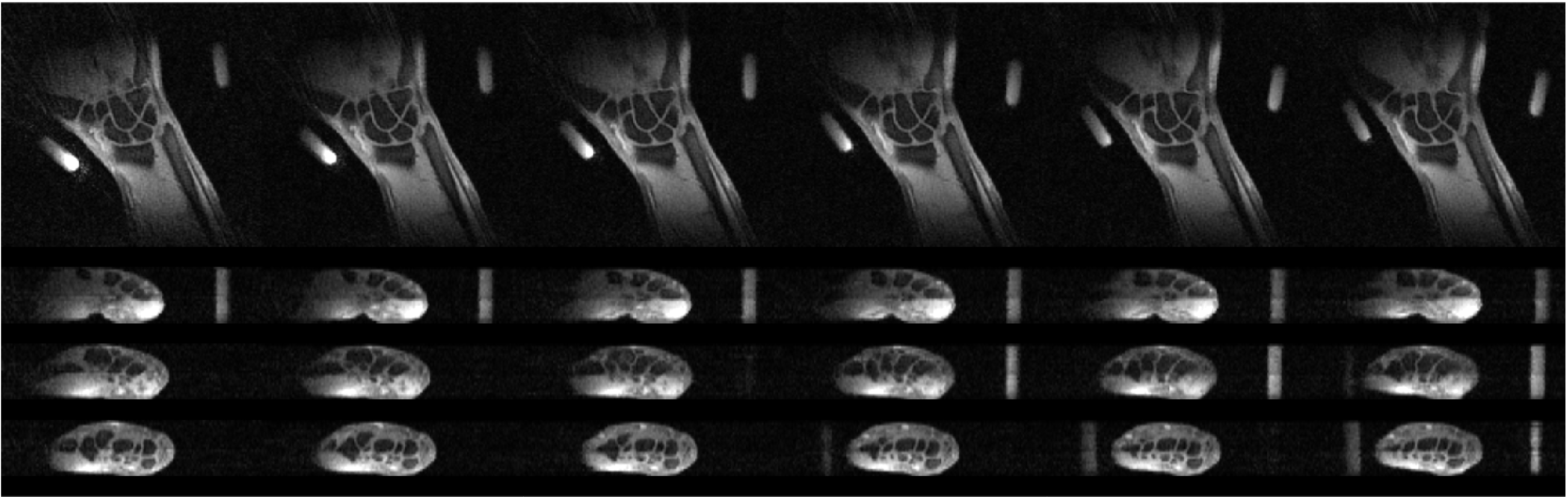
Figure 1 shows the assembled dynamic volumes for different wrist angular positions, for a representative volunteer. The temporal resolution was 48 ms/frame3. Table 1 shows the accuracy of the registration between the static MRI and the template by evaluating the similarity between their segmentation maps. Figure 2 shows the non-rigid artifacts created by non-linear deformation of the bone segments from the template to each 3D frame. Figure 3 shows the improved accuracy of our wrist model after applying poly-rigid registration to enforce rigid body constraints over the respective motion trajectory of each bone. Figure 4 qualitatively assesses the repeatability of the wrist motion by juxtaposing two scans of the same subject. Furthermore, it demonstrates the potential to enforce structural consistency across multiple scans of the same subject.Discussion
In this work, we presented a novel imaging and processing approach for functional kinematic analysis. Most of the existing methods use either 2D real-time imaging or 3D dynamic imaging with temporal resolution of several seconds. To our knowledge, this is the first work to model carpal bone motion using dynamic volumetric MRI at high temporal-spatial resolution.Future work includes quantitative kinematic analysis, a reproducibility study of bone motion quantification and the evaluation of patients with wrist instability vs. healthy volunteers.
Acknowledgements
This work was supported in part by NIH R21 AR080325 and performed under the rubric of the Center for Advanced Imaging Innovation and Research (CAI2R, www.cai2r.net), an NIBIB National Center for Biomedical Imaging and Bioengineering (NIH P41 EB017183).References
1. Vassa R, Garg A, Omar IM. Magnetic resonance imaging of the wrist and hand. Polish Journal of Radiology. 2020 Aug 26;85(1):461-88.
2. Ramamurthy NK, Chojnowski AJ, Toms AP. Imaging in carpal instability. Journal of Hand Surgery (European Volume). 2016;41(1):22-34.
3. Zi R, Wang B, Walczyk J, Brown R, Petchprapa C, Fishbaugh J, Gerig G, Block KT, Lattanzi R, Volumetric Dynamic Imaging for Functional Kinematic Assessment of the Wrist, ISMRM 2023: 1437.
4. Avants, B. B., et al. "Ants: open-source tools for normalization and neuroanatomy. Transac Med Imagins Penn Image Comput Sci Lab 2009."
5. P. A. Yushkevich, Y. Gao, and G. Gerig. Itk-snap: An interactive tool for semi-automatic segmentation of multi-modality biomedical images. In 2016 38th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), pages 3342–3345, 2016. www.itksnap.org.
6. Sungjoon Choi, Q. -Y. Zhou and V. Koltun, "Robust reconstruction of indoor scenes," 2015 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Boston, MA, USA, 2015, pp. 5556-5565, doi: 10.1109/CVPR.2015.7299195.
7. R. B. Rusu, N. Blodow and M. Beetz, "Fast Point Feature Histograms (FPFH) for 3D registration," 2009 IEEE International Conference on Robotics and Automation, Kobe, Japan, 2009, pp. 3212-3217, doi: 10.1109/ROBOT.2009.5152473.
8. P. J. Besl and N. D. McKay, "A method for registration of 3-D shapes," in IEEE Transactions on Pattern Analysis and Machine Intelligence, vol. 14, no. 2, pp. 239-256, Feb. 1992, doi: 10.1109/34.121791.
9. Zhou, Qian-Yi, Jaesik Park, and Vladlen Koltun. "Open3D: A modern library for 3D data processing." arXiv preprint arXiv:1801.09847 (2018).
Figures