1026
Automatic spinal cord segmentation: Generalization across MR parameters, sites, vendors and pathologies1NeuroPoly Lab, Institute of Biomedical Engineering, Polytechnique Montréal, Montréal, QC, Canada, 2Mila - Quebec AI Institute, Montréal, QC, Canada, 3Max Planck Institute for Human Cognitive and Brain Sciences, Leipzig, Germany, 4Department of Anesthesiology, Perioperative and Pain Medicine, Stanford University School of Medicine, Stanford, CA, United States, 5Department of Radiology and Medical Informatics, University of Geneva, Geneva, Switzerland, 6Neuro-X Institute, École Polytechnique Fédérale de Lausanne (EPFL), Geneva, Switzerland, 7Spinal Cord Injury Center, Balgrist University Hospital, University of Zürich, Zürich, Switzerland, 8Department of Neurophysics, Max Planck Institute for Human Cognitive and Brain Sciences, Leipzig, Germany, 9Department of Medicine (Neurology), University of Toronto, Toronto, ON, Canada, 10BARLO Multiple Sclerosis Centre & Keenan Research Centre, St. Michael's Hospital, Toronto, ON, Canada, 11University of British Columbia, Vancouver, BC, Canada, 12School of Biomedical Engineering, Faculties of Applied Science and Medicine, University of British Columbia, Vancouver, BC, Canada, 13Department of neuroscience, Université de Montréal, Montréal, QC, Canada, 14Neuroimmunology research laboratory, University of Montreal Hospital Research Centre (CRCHUM), Montréal, QC, Canada, 15Physikalisch-Technische Bundesanstalt (PTB), Braunschweig and Berlin, Germany, 16Functional Neuroimaging Unit, CRIUGM, Université de Montréal, Montréal, QC, Canada, 17Centre de Recherche du CHU Sainte-Justine, Université de Montréal, Montréal, QC, Canada
Synopsis
Keywords: Segmentation, Spinal Cord, Segmentation; Deep Learning; Morphometrics; Atrophy; Variability; Reproducibility; Vendors
Motivation: Spinal cord cross-sectional area (CSA) is an important biomarker for neurodegenerative and traumatic diseases. However, CSA measurements vary across MRI contrasts and imaging protocols, limiting its use in multi-center studies.
Goal(s): The goal is to evaluate CSA variability using a novel contrast-agnostic segmentation method.
Approach: We compared this method to the Spinal Cord Toolbox's DeepSeg, analyzing CSA across different sites, and MRI vendors. Additionally, we compared the segmentations in diverse datasets and pathologies.
Results: The contrast-agnostic segmentation showed lower CSA variability, and superior performance in most cases, except for intramedullary cord compression, where the Spinal Cord Toolbox's DeepSeg was more accurate.
Impact: The contrast-agnostic method yields reliable spinal cord CSA measurements, independent of MRI contrasts and vendors. This, combined with a soft segmentation output, can potentially detect subtle spinal cord atrophy in prospective multi-center cohorts.
Introduction
Spinal cord cross-sectional area (CSA) is an important biomarker for the prognosis and monitoring of several neurodegenerative disorders such as multiple sclerosis, traumatic and non traumatic spinal cord injuries1–4. However, CSA measurements are known to vary across MRI contrasts. For instance, CSA values obtained from T2-weighted (T2w) images are about 8% larger compared to those from T1-weighted (T1w) images5,6. This variability poses challenges for the use of CSA in multi-center studies, where imaging protocols often differ. Recently, we proposed a novel segmentation method7 that specifically addressed this contrast-dependency in spinal cord segmentations. However, the variability of CSA measurements has not yet been validated across MRI vendors and diverse datasets.Our objective was to assess variability in spinal cord CSA across contrasts and MRI vendors. We compare segmentations obtained using the new contrast-agnostic method7 with those generated by the state-of-the-art DeepSeg method8 from the Spinal Cord Toolbox (SCT)9. We also highlight the predicted segmentations of the contrast-agnostic method on various datasets, contrasts and pathologies unseen during model training.
Methods
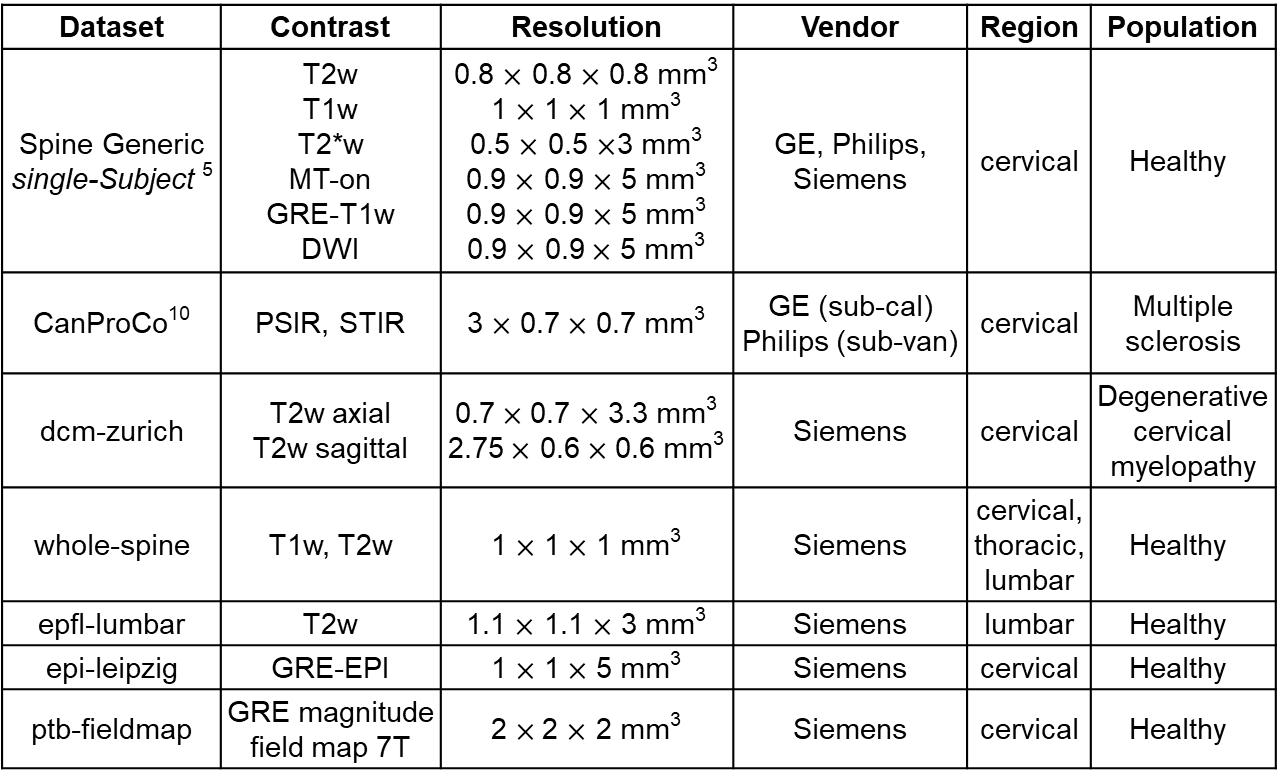
In this study, we analyzed data from the Spine Generic data-single-subject dataset5, which includes scans of the cervical spinal cord in a single healthy participant using six contrasts (T2w, T1w, T2*w, MT-on, GRE-T1w, and DWI) across 15 sites with 3 scanner vendors (GE n=4, Philips n=4, Siemens n=7). For all contrasts and sites, we segmented the spinal cord automatically using DeepSeg in SCT and the contrast-agnostic method. It is important to note that the contrast-agnostic method was trained only on a dataset of healthy participants. Vertebral levels were identified using sct_label_vertebrae. We computed CSA averaged across C2-C3 vertebral levels and its standard deviation (SD) across contrasts per site to compare CSA variability. We compared the SD of both segmentation methods across vendors.Subsequently, both the contrast-agnostic segmentation method and DeepSeg were applied to additional datasets for a qualitative assessment of the segmentations, as outlined in Table 1.
Results
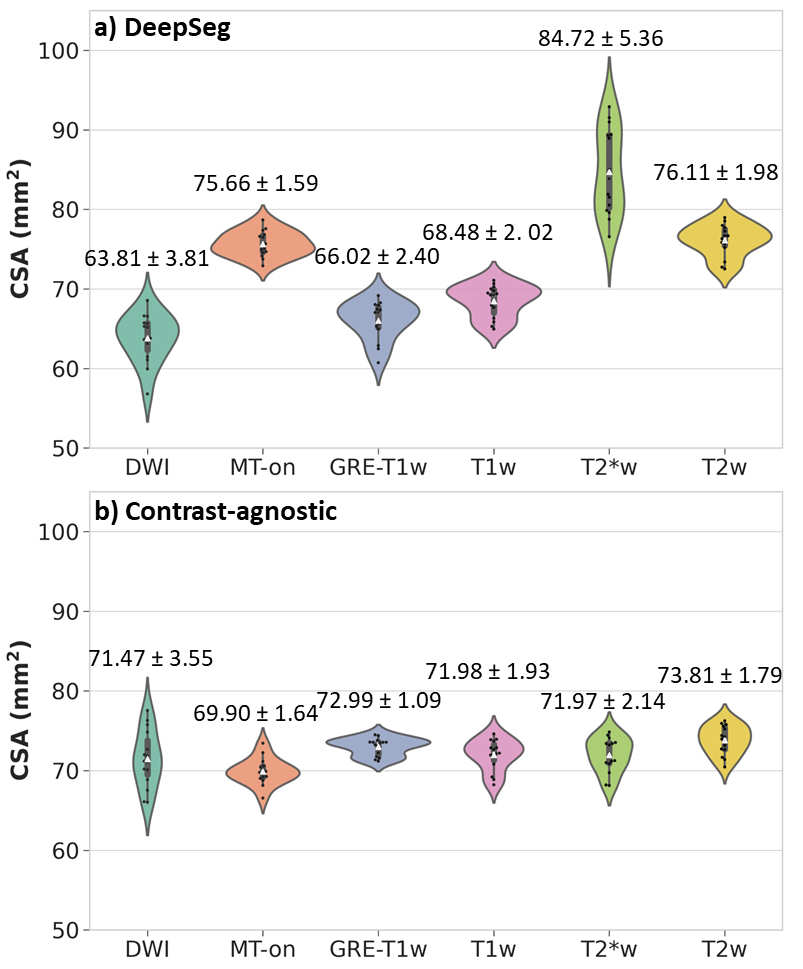
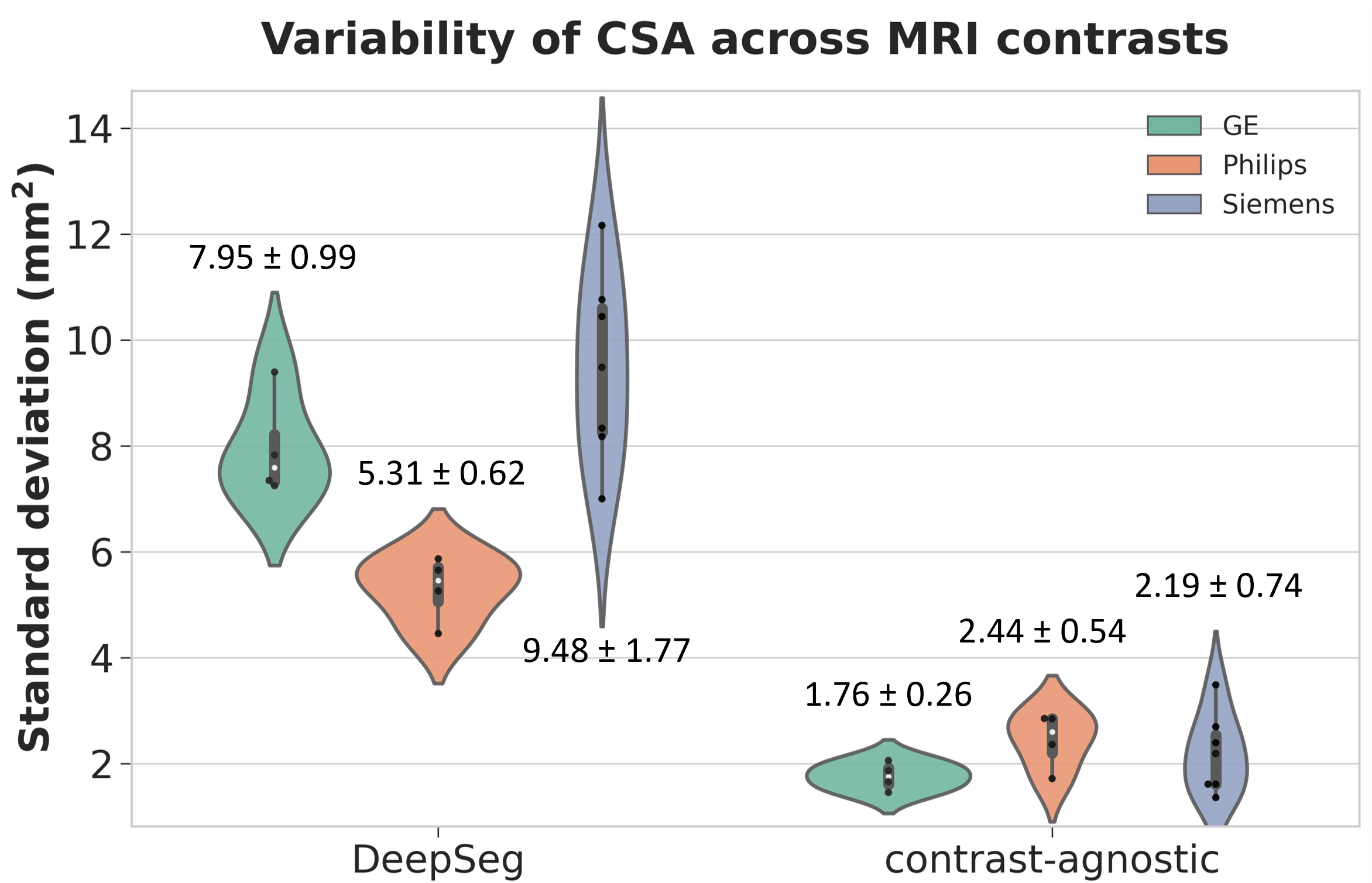
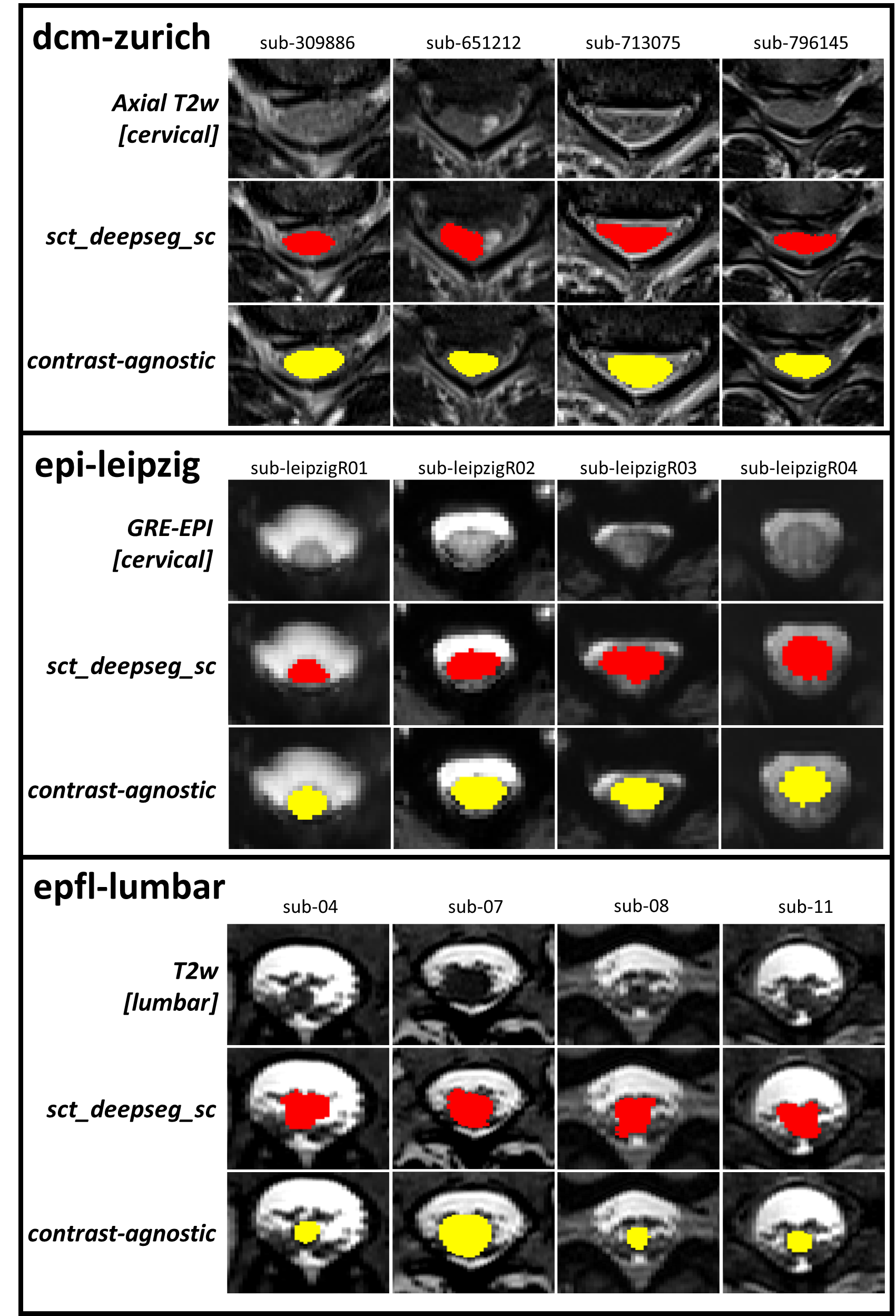
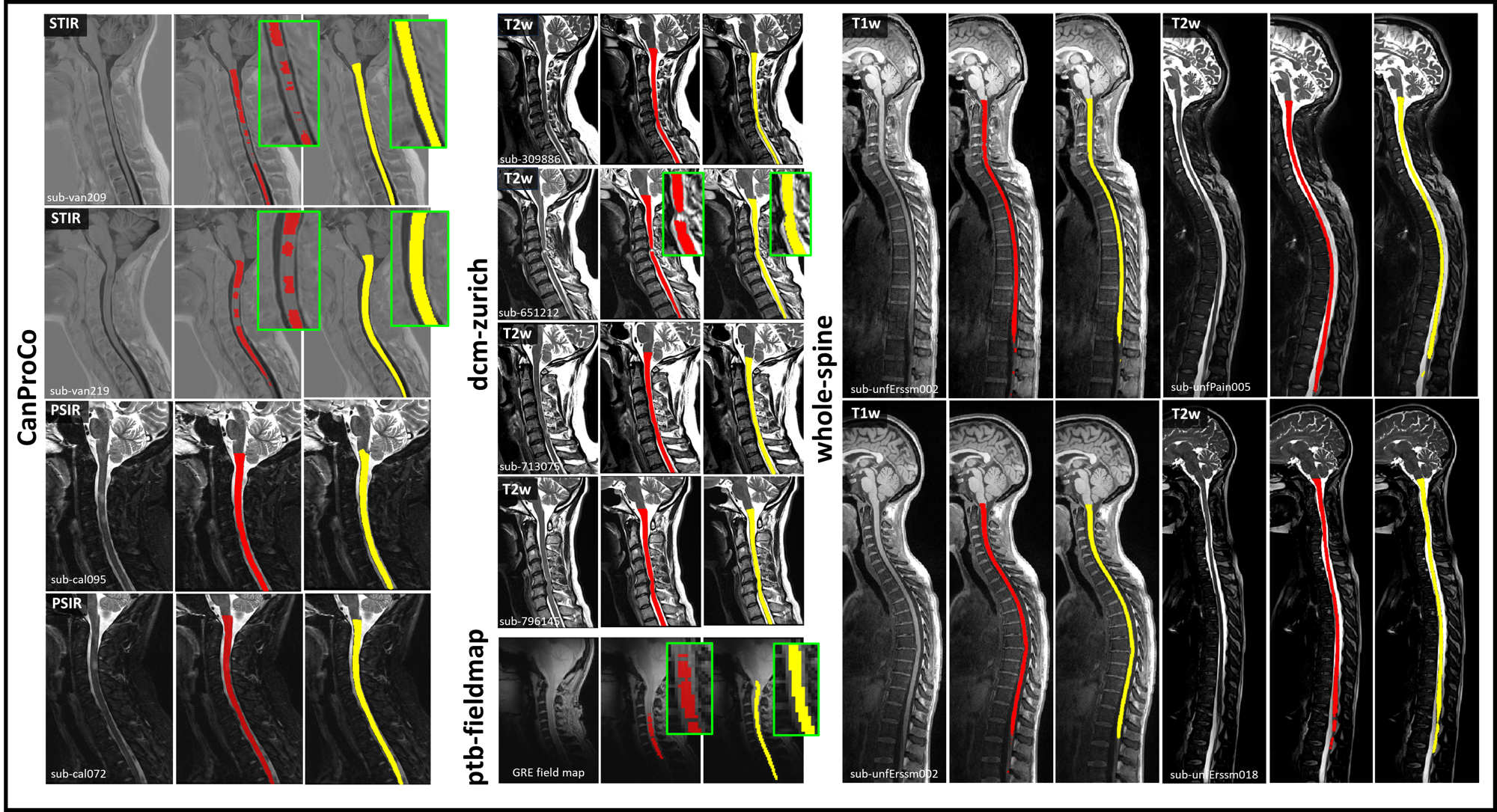
Figure 1 presents the spinal cord CSA values for each of the 6 contrasts comparing the two segmentation methods across all 15 sites. Qualitatively, the contrast-agnostic method (Figure 1b) notably demonstrates less variability in CSA values compared to those derived from DeepSeg (Figure 1a). It is important to stress that all data points represent the same participant. Figure 2 presents the CSA SD across 6 contrasts per site for both segmentation methods separated per MRI vendor. The SD using the contrast-agnostic method yields a lower SD than when using DeepSeg for segmentation (p-value < 0.05, two-sided paired non-parametric Wilcoxon signed-rank test). We observe for both segmentation methods a higher SD for Siemens compared to the two other vendors, which may be attributed to the higher number of Siemens sites (n=7) compared to n=4 for Philips and n=4 for GE.Figure 3 and Figure 4 show the spinal cord segmentations obtained from the DeepSeg (in red) and the contrast-agnostic method (in yellow), applied to a range of images across different contrasts and datasets (Table 1). We observe that in the presence of lesions (CanProCo and dcm-zurich), the contrast-agnostic method is able to delineate the shape of the spinal cord superior compared to DeepSeg segmentation which tends to under-segment the spinal cord at the location of the lesions. In contrast, in cases of spinal cord compression (observed in dcm-zurich), DeepSeg appears to more accurately match the segmentation to the compressed spinal cord structure. This disparity is likely due to the fact that the contrast-agnostic method was trained on healthy participants, and hence did not include participants with spinal cord compression. Additionally, we observed that the contrast-agnostic method was able to segment the cord on a field map magnitude image while DeepSeg under-segmented the spinal cord (Figure 2).
Discussion
The contrast-agnostic segmentation method allows reproducible spinal cord morphometrics not only across MRI contrast but across sites, MRI vendors and pathologies. This will facilitate multi-center studies using CSA as a biomarker, where protocols, scanners and vendors often differ11. The study also highlights the generalizability of the contrast-agnostic method compared to the traditional DeepSeg method, especially notable in contrasts and resolutions not included during training, such as GRE magnitude field map, GRE-EPI, STIR, and PSIR.Future research directions will involve implementing active learning strategies12 to address the issue of manually fixing soft segmentation, and to incorporate a broader spectrum of contrasts, pathologies (i.e., spinal cord compression), and anatomical regions. This expansion is expected to further enhance the method's applicability and accuracy in diverse clinical and research settings.
Acknowledgements
We thank Nicholas Guenther, Alexandru Foias and Mathieu Guay-Paquet for data management with git-annex. We thank Haris Tsagkas for the insightful discussions.
Funded by the Canada Research Chair in Quantitative Magnetic Resonance Imaging [CRC-2020-00179], the Canadian Institute of Health Research [PJT-190258], the Canada Foundation for Innovation [32454, 34824], the Fonds de Recherche du Québec - Santé [322736, 324636], the Natural Sciences and Engineering Research Council of Canada [RGPIN-2019-07244], the Canada First Research Excellence Fund (IVADO and TransMedTech), the Courtois NeuroMod project, the Quebec BioImaging Network [5886, 35450], INSPIRED (Spinal Research, UK; Wings for Life, Austria; Craig H. Neilsen Foundation, USA), Mila - Tech Transfer Funding Program.
References
1. Bonacchi, R. et al. Clinical Relevance of Multiparametric MRI Assessment of Cervical Cord Damage in Multiple Sclerosis. Radiology 296, 605–615 (2020).
2. Barkhof, F. et al. Comparison of MRI criteria at first presentation to predict conversion to clinically definite multiple sclerosis. Brain 120 ( Pt 11), 2059–2069 (1997).
3. Trolle, C., Goldberg, E. & Linnman, C. Spinal cord atrophy after spinal cord injury - A systematic review and meta-analysis. Neuroimage Clin 38, 103372 (2023).
4. Martin, A. R. et al. Can microstructural MRI detect subclinical tissue injury in subjects with asymptomatic cervical spinal cord compression? A prospective cohort study. BMJ Open 8, e019809 (2018).
5. Cohen-Adad, J. et al. Open-access quantitative MRI data of the spinal cord and reproducibility across participants, sites and manufacturers. Sci Data 8, 219 (2021).
6. Kim, G. et al. T1- vs. T2-based MRI measures of spinal cord volume in healthy subjects and patients with multiple sclerosis. BMC Neurol. 15, 124 (2015).
7. Bédard, S. et al. Towards contrast-agnostic soft segmentation of the spinal cord. arXiv [eess.IV] (2023).
8. Gros, C. et al. Automatic segmentation of the spinal cord and intramedullary multiple sclerosis lesions with convolutional neural networks. Neuroimage 184, 901–915 (2019).
9. De Leener, B. et al. SCT: Spinal Cord Toolbox, an open-source software for processing spinal cord MRI data. Neuroimage 145, 24–43 (2017).
10. Oh, J. et al. The Canadian prospective cohort study to understand progression in multiple sclerosis (CanProCo): rationale, aims, and study design. BMC Neurol. 21, 418 (2021).
11. Bautin, P. & Cohen-Adad, J. Minimum detectable spinal cord atrophy with automatic segmentation: Investigations using an open-access dataset of healthy participants. Neuroimage Clin 32, 102849 (2021).
12. Budd, S., Robinson, E. C. & Kainz, B. A survey on active learning and human-in-the-loop deep learning for medical image analysis. Med. Image Anal. 71, 102062 (2021).
Figures