1011
Robust Multi-Shot Diffusion Weighted Imaging of the Abdomen with Region-Based Shot Rejection1Radiology, Stanford University, Stanford, CA, United States, 2Bioengineering, Stanford University, Stanford, CA, United States, 3Electrical Engineering, Stanford University, Stanford, CA, United States
Synopsis
Keywords: Diffusion Reconstruction, Diffusion/other diffusion imaging techniques
Motivation: To improve the motion robustness of multi-shot DWI in the abdomen and reduce signal dropouts and ADC overestimation caused by unresolved shot-to-shot phase.
Goal(s): Demonstrate that region-based weighting of different shots improves diffusion contrast in rapidly moving abdominal organs.
Approach: Shot rejection was evaluated in the pancreas. Multiple shot rejection formulations were tested, and compared using conventional monopolar, and motion-compensated diffusion encodings.
Results: Shot rejection allows conventional monopolar encoding to achieve diffusion weighting and ADCs similar to the motion-compensated encoding in the pancreas. The reconstruction is linear, requires no modifications to the sequence, and is applicable to many encoding trajectories.
Impact: Shot rejection may improve the consistency and robustness of multi-shot abdominal DWI in the clinic, as well as its ability to differentiate pathologies. This will improve repeatability of DWI studies of rapidly moving organs, such as the pancreas and heart.
Introduction
Diffusion-weighted imaging is a useful clinical contrast for cancer surveillance, treatment planning, and imaging inflammation1. Multi-shot EPI reduces distortions caused by off-resonance in EPI, which are prominent in body imaging. Multi-shot DWI reconstructions often assume an unspecified “low-resolution” phase to simplify phase navigator estimation. In practice however, the phase navigator resolution required to correctly reconstruct the image is dependent on multiple factors including: anatomy, gradient moment of the diffusion encoding waveform, and subject participation.This work studies the effect of phase navigator resolution in abdominal DWI, and applies a new multi-shot rejection formulation to discard regions overly-corrupted diffusion gradients. We compared shot rejection in DW-EPI data acquired with conventional monopolar, and flow-compensated diffusion encoding. The shot rejection reconstruction allows monopolar diffusion encoding to obtain median ADCs in the pancreas (a rapidly moving organ)2 comparable to flow-compensated gradients, and provides the ability to partially recover when the phase navigator is estimated poorly.
Theory
The conventional multi-shot reconstruction problem3 is shown in Figure 1, Equation 1. Two assumptions are made when solving the linear system in Equation 1:1. The underlying image magnitude is constant between shots
2. The phase navigator estimate is accurate
The first assumption may be violated when a large gradient imbalance causes subvoxel dephasing. The second assumption may be violated when the phase navigator is too low-resolution. Examples are shown in Figure 2, with shots from a respiratory-triggered 4-shot abdomen acquisition reconstructed with parallel imaging and filtered to different resolutions. Subvoxel dephasing is visible in the pancreas (blue arrows), where the signal magnitude changes between shots. Flow-compensated diffusion encoding improves the consistency of the signal magnitudes but some variations persist. Dropouts in the low-resolution phase navigator that change between shots are due to phase cancellation between adjacent voxels, and indicate that the phase navigator incorrectly estimates the underlying image phase (red arrow). These artifacts can be reduced by applying image domain rejection weights (Equation 2), which weight down areas where assumptions are violated (white arrows).
Methods
Acquisitions were performed at 3T (GE Signa Premier) in three healthy volunteers (two male) following IRB approval and informed consent. Pancreas acquisition parameters were: 4-shots, 3 NEX b = 0, 500 s/mm2, FOV 36 cm, matrix 192×192, slice thickness 5 mm, TE 55 ms (conventional monopolar), respiratory triggering, 12 slices / 2 passes, partial Fourier 0.75, one diffusion direction (all axes enabled). The flow-compensated acquisition used M1-Nulled Convex Optimized Diffusion Encoding4 (CODE), TE 75 ms.Reconstructions were performed with two different phase navigator resolutions, reconstructed with parallel imaging5, and triangle windowed in k-space to FWHM 24×24 (1.6 cm voxels), and 96×96 (0.4 cm voxels). Weights were computed by applying the Walsh method6 to the phase navigator magnitude images (window size 0.8×0.8 cm). Single-shot, multi-shot without shot rejection using low and high-resolution phase navigators, the WLSQ3 (Equations 3/4), and SENSE-like rejection formulations were compared.
Results
Figure 3 shows one slice reconstructed with different phase navigator resolutions and rejection formulations. Conventional multi-shot reconstructions have different contrast in the pancreas (white arrow), dependent on phase navigator resolution. Applying shot rejection achieves image contrast in the pancreas independent of phase navigator resolution. Banding is present in the kidney (red arrow), when reconstructed with the low-resolution phase navigator, but it is eliminated with shot rejection (blue arrow). This demonstrates that the shot rejection is effective at eliminating shots where the phase navigator is estimated poorly. The reconstructions for all rejection formulations in one volunteer are shown in Figure 4.Figure 5 shows ADCs in the pancreas for images in Figure 3. With monopolar encoding, single-shot reconstruction overestimates ADC compared to the flow-compensated single-shot reference, which is expected since the pancreas is dephased in many shots. Neither the high, nor low-resolution phase navigator is sufficient to obtain the same median ADC as the single-shot reconstruction due to cancellations from residual shot-to-shot phase. With SENSE-like shot rejection, the monopolar acquisition achieves similar median ADCs to the flow-compensation with shot rejection. Flow-compensated diffusion encoding requires a lower phase navigator resolution to obtain ADCs comparable to the single-shot reconstruction, and shot rejection has a lesser effect.
Discussion
We applied a region-based shot rejection to improve the motion robustness of multi-shot DWI in the abdomen. We studied the effect of phase navigator resolution, and showed how it affects diffusion contrast. Shot rejection and motion-compensated diffusion encoding are complementary, and applications may still benefit from flow compensation despite its longer TE.Conclusion
Region-based shot rejection is a linear reconstruction that improves the motion robustness of multi-shot DWI, requires no sequence modifications, and is applicable to many encoding trajectories.Acknowledgements
Research support from GE Healthcare. NIH R01-CA249893. Karolinska Neuro MR Physics group for pulse programming assistance. Dr. Matthew Middione for providing the CODE sequence.References
1. Baliyan Vinit, Das Chandan J, Sharma Raju, Gupta Arun Kumar. Diffusion weighted imaging: technique and applications. World Journal of Radiology. 2016;8(9):785.
2. Geng Ruiqi, Zhang Yuxin, Starekova Jitka, et al. Characterization and correction of cardiovascular motion artifacts in diffusion-weighted imaging of the pancreas. Magnetic Resonance in Medicine. 2021;86:1956-1969.
3. Miller Karla L, Pauly John M. Nonlinear phase correction for navigated diffusion imaging. Magnetic Resonance in Medicine. 2003;50:343-353.
4. Aliotta Eric, Wu Holden H, Ennis Daniel B. Convex optimized diffusion encoding (CODE) gradient waveforms for minimum echo time and bulk motion–compensated diffusion-weighted MRI. Magnetic Resonance in Medicine. 2017;77(2):717–729.
5. Chen Nan Kuei, Guidon Arnaud, Chang Hing Chiu, Song Allen W. A robust multi-shot scan strategy for high-resolution diffusion weighted MRI enabled by multiplexed sensitivity-encoding (MUSE). NeuroImage. 2013;72:41-47.
6. Walsh David O, Gmitro Arthur F, Marcellin Michael W. Adaptive reconstruction of phased array MR imagery. Magnetic Resonance in Medicine. 2000;43:682-690.
Figures
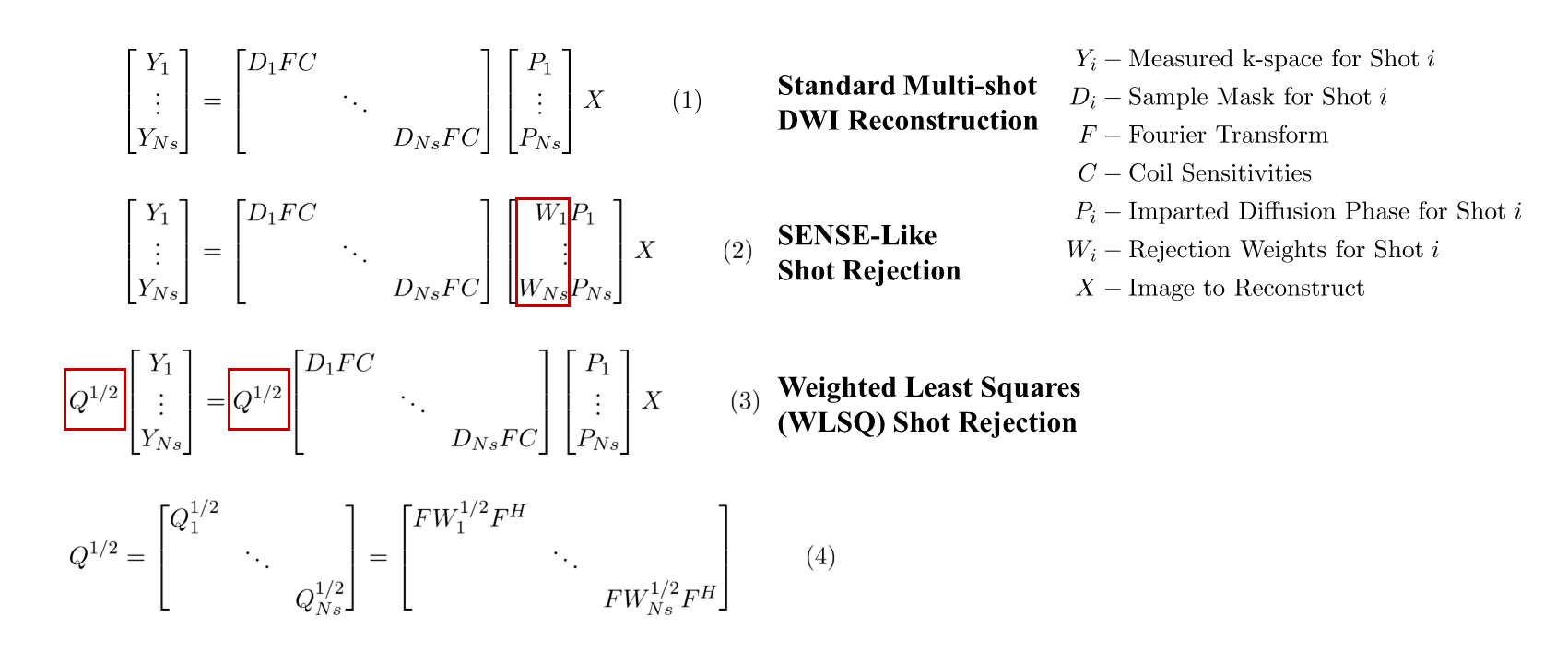
Figure 1: Linear systems for reconstructions that account for varying shot-to-shot phase. (1) Conventional multi-shot DWI. (2) SENSE-Like shot rejection. (3/4) WLSQ rejection. A single-shot reconstruction reconstructs each shot independently, followed by magnitude averaging.
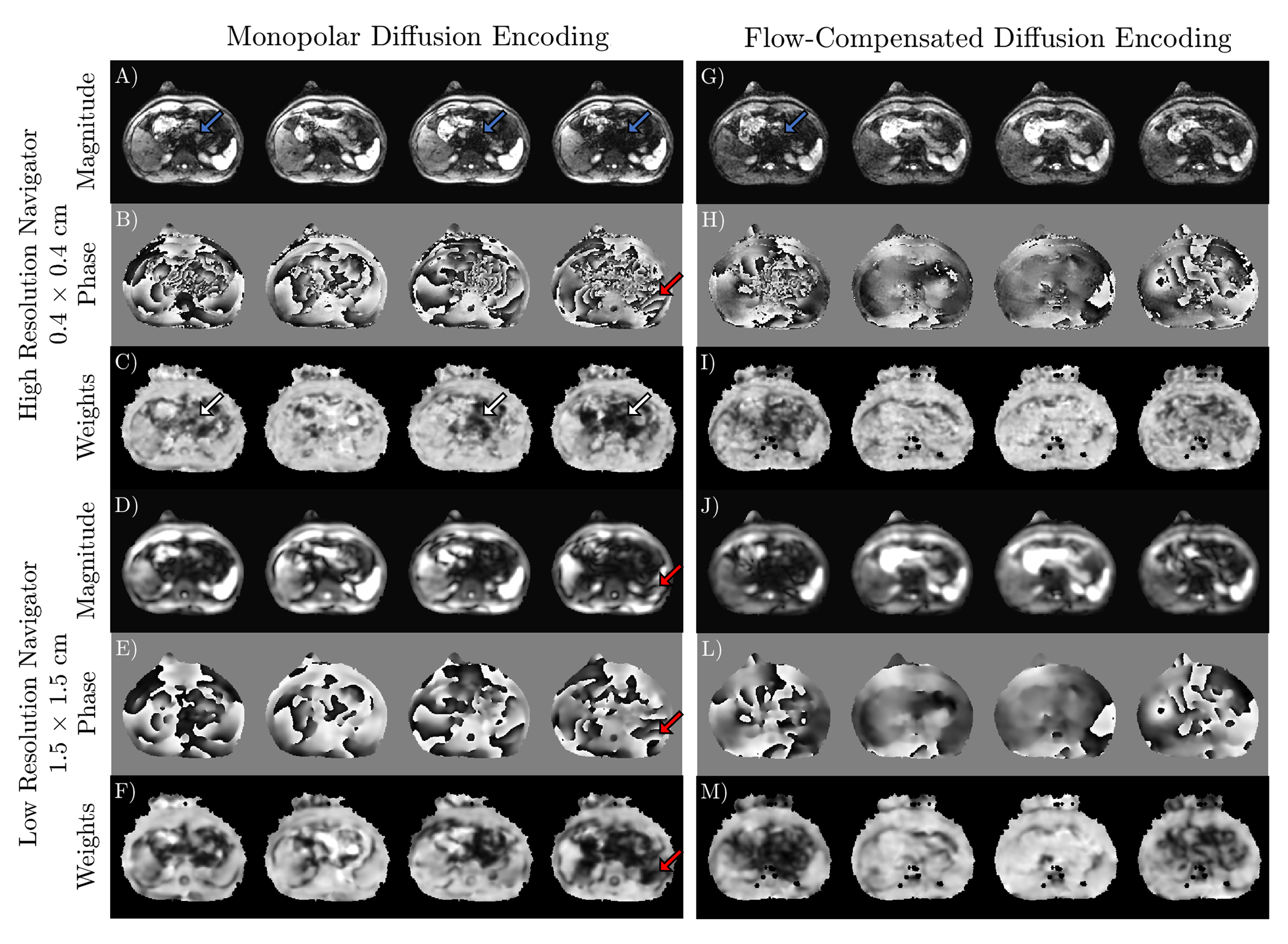
Figure 2: Phase navigator images and weights reconstructed at two different resolutions for conventional (A-F) and flow-compensated diffusion encoding (G-M). Red arrows indicate a region where the local phase imparted by diffusion gradients has high resolution. Low signal magnitudes in the low-resolution phase navigators relative to other shots indicate that the phase is poorly estimated in this region. Blue arrows point to examples of subvoxel dephasing in the pancreas, that are weighted down (white arrows).
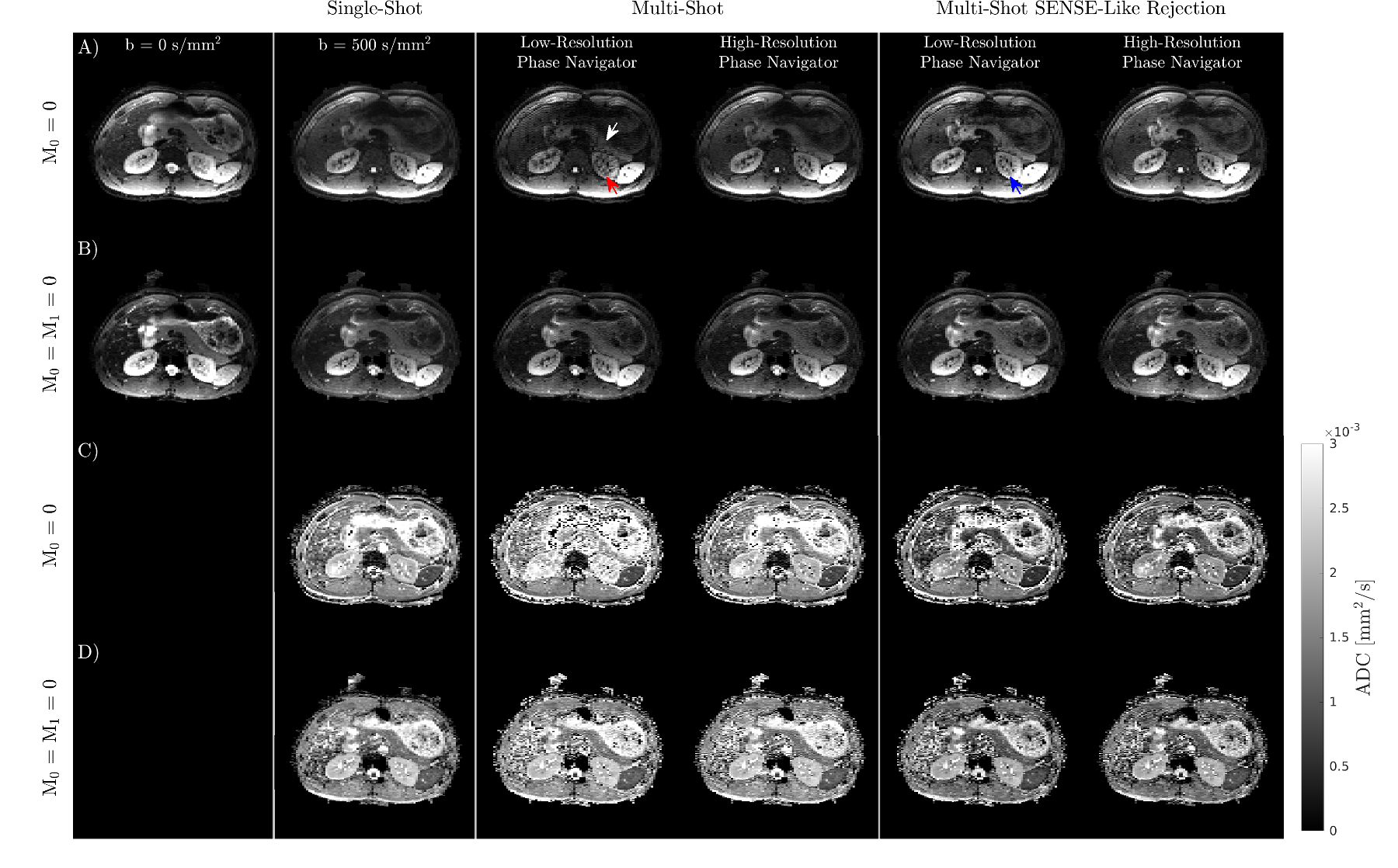
Figure 3: Comparison of different reconstructions. Insufficient phase navigator resolution causes signal loss in the pancreas (white arrow), and banding in the left kidney (red arrow). Banding is eliminated using a higher resolution phase navigator or by applying shot rejection (blue arrow). Shot rejection enables similar image contrast in the pancreas regardless of phase navigator resolution. Images and ADCs from (A, C) conventional / (B, D) flow-compensated diffusion encoding.
Figure 4: Reconstructions for multiple slices and all rejection formulations in second volunteer.
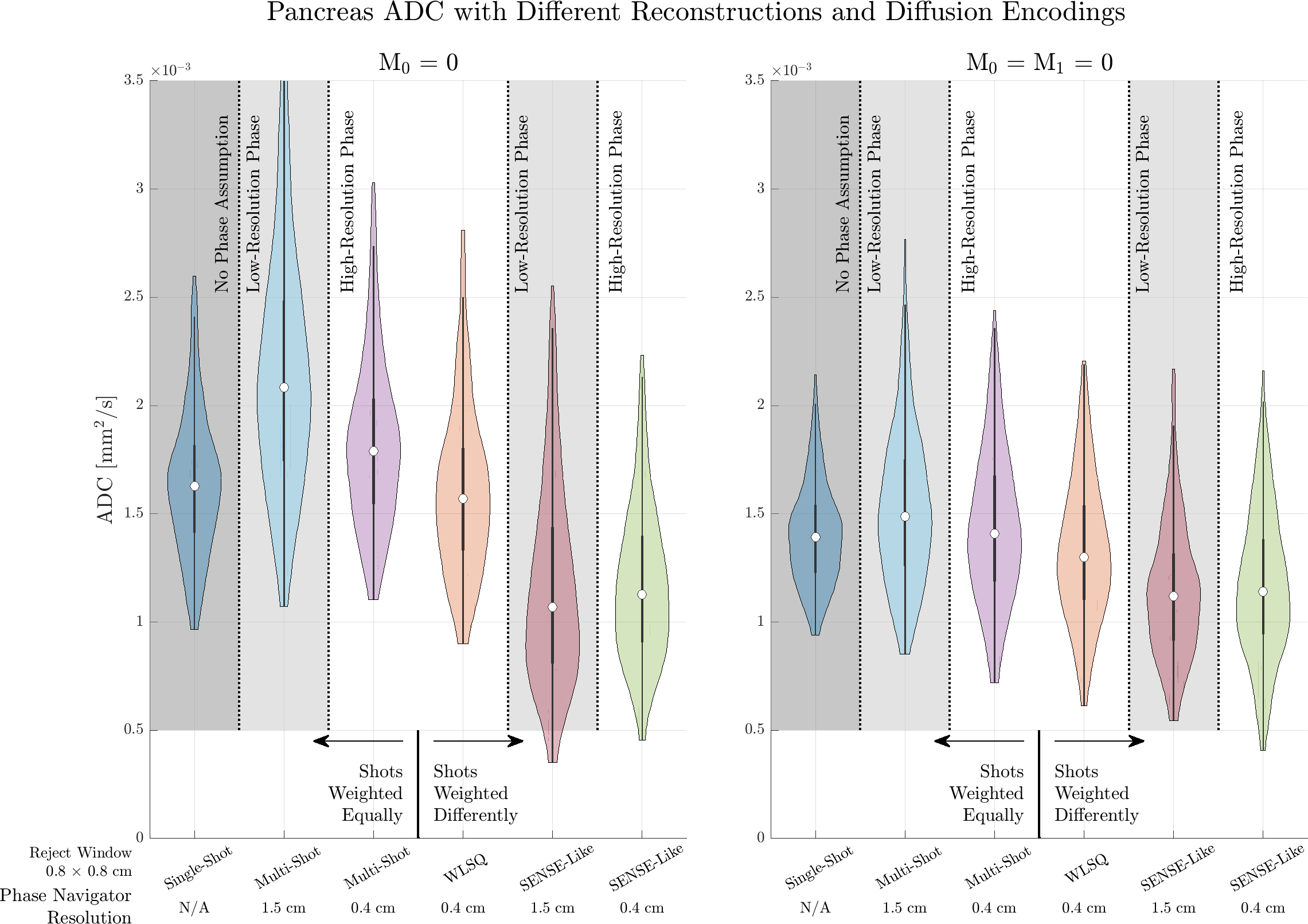
Figure 5: Violin plots comparing ADC estimates in the pancreas obtained with monopolar and flow-compensated diffusion encoding, and different reconstructions for the slice shown in Figure 3.