1006
4D Dynamic Brain PET Prediction Using Anatomical and Statistical Models1Washington University in St.Louis, Creve Coeur, MO, United States, 2Washington University in St.Louis, St. Louis, MO, United States, 3Washington University in St. Louis, St. Louis, MO, United States
Synopsis
Keywords: Diagnosis/Prediction, Machine Learning/Artificial Intelligence, 4D Dynamic PET, PCA
Motivation: The reduction in PET scan duration not only improves the efficiency of the scanning process but also contributes to a more comfortable experience for patients.
Goal(s): Leveraging the temporal models in conjunction with previously predicted weights of PCs, we aim to reconstruct entire 4D dynamic PET frames using an inverse PCA method.
Approach: A novel technique has been developed to generate pseudo-T1 images from noisy 4D PET data, as well as the reverse process, obtaining the initial components of 4D dynamic PET images from MRI data.
Results: The results endorsed that only 5 minutes observation is enough to predict whole 70 minute data.
Impact: We predicted later PET frames from noisy initial frames using a novel approach combining anatomical and statistical temporal PCs from MRI data. This method has clinical potential for insights into dynamic processes, radiation reduction, and identifying abnormalities in medical imaging.
Introduction
Several applications demand dynamic PET imaging, but the extended acquisition time has constrained its clinical utility. Shortening PET scanning offers several benefits, such as enhanced scanner efficiency, improved patient comfort, and decreased susceptibility to motion artifacts, especially in elderly and pediatric patients. To our knowledge, there is limited previous research on employing deep learning for expediting dynamic PET image acquisition or generating late dynamic frames from early ones. Our primary goal is to reduce scanning time while preserving result quality and minimizing bias.Method
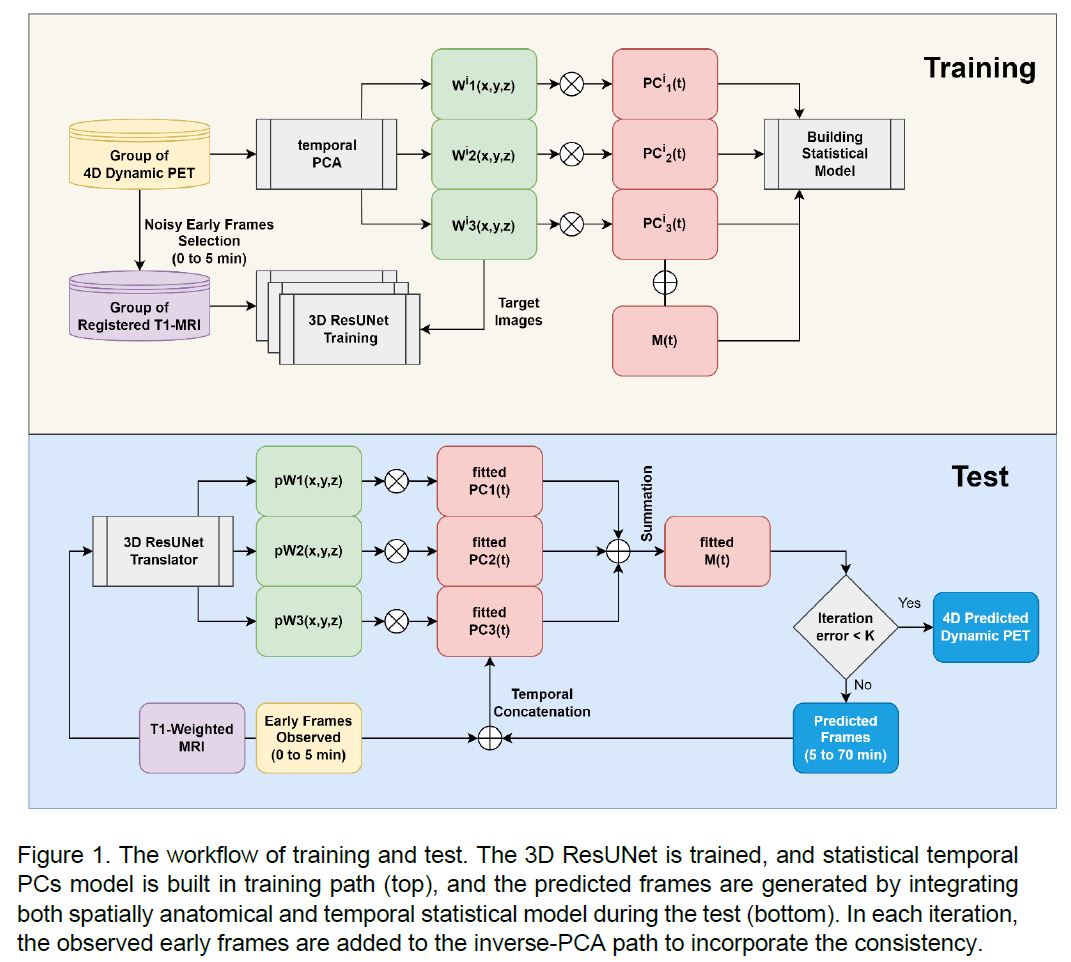
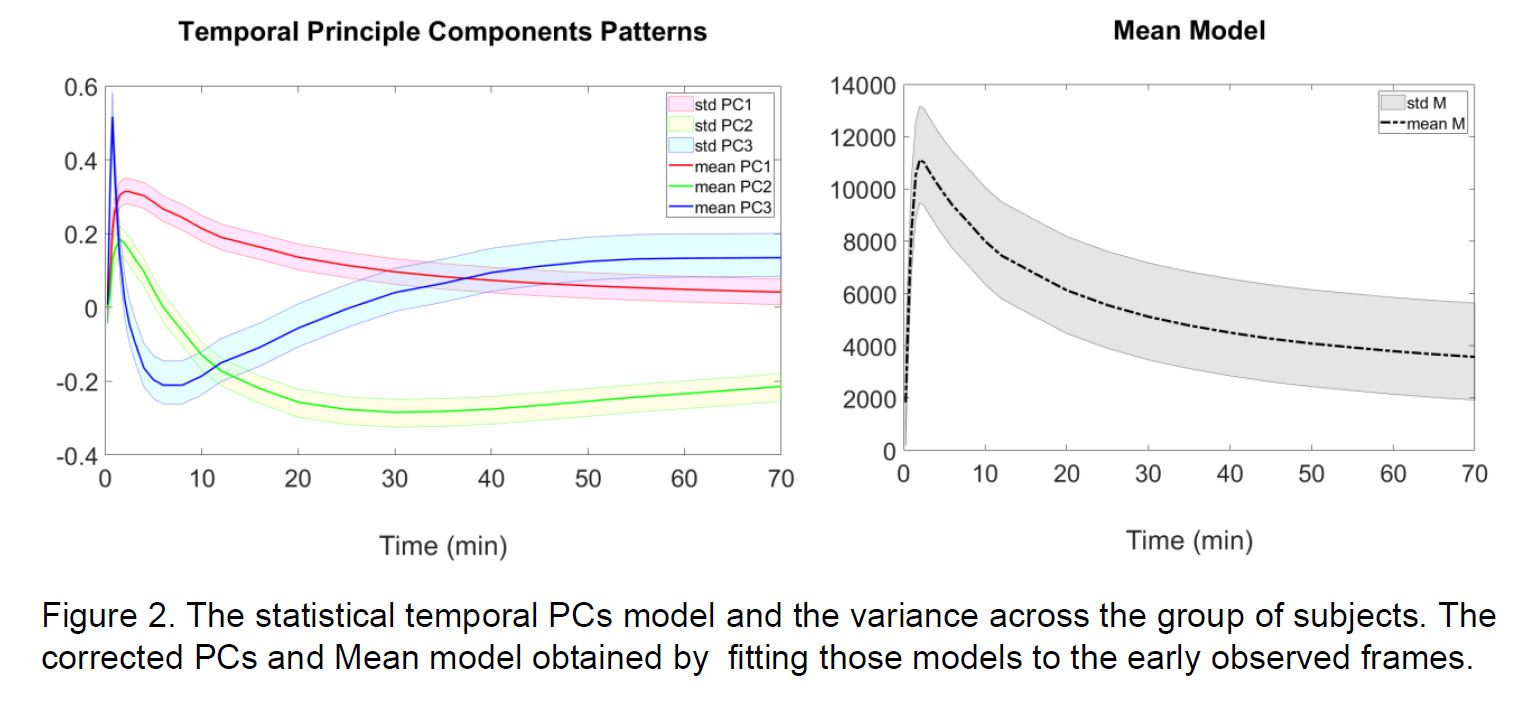
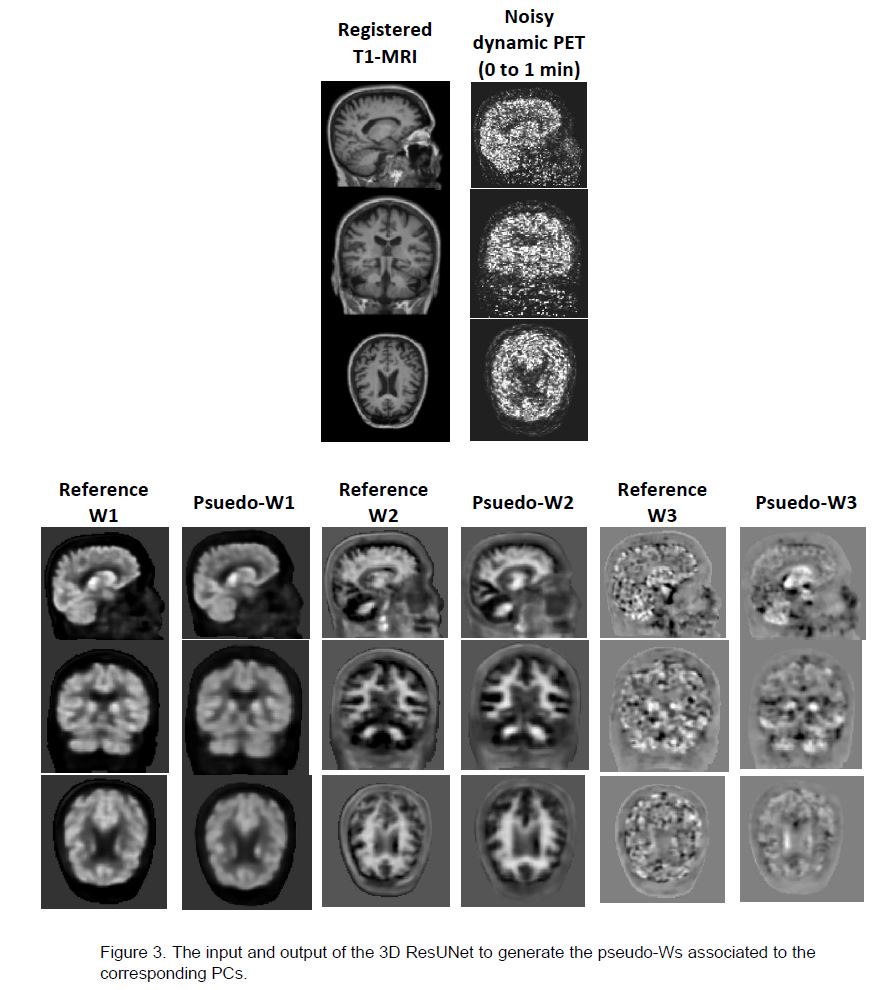
With assumption that different tissues exhibit unique tracer uptake patterns, we aim to establish statistical temporal models for the specific tracer to decompose the 4D data based on these models. By incorporating spatial weights of principal components (PCs), we predicted 4D dynamic PET using early frame observations. We first extracted PCs from spatial denoised 4D PET images using a CNN 1. Our prior study demonstrated the importance of spatial denoising in reducing the number of PCs from 20 noisy PCs to 4 PCs in preserving more than 95% of the information in the entire 4D data. Subsequently, we constructed a mean statistical temporal PCs model for the brain, assuming tissue activity follows similar time activity patterns across subjects using the same tracer. Those models encompassed the mean and covariance of each PCs across the group of training subjects 2,3. Gram-Schmidt orthonormalization computations were employed to keep zero-mean reconstructed images (see Figure 2). To estimate the weights of each voxel with respect to these PCs, we leveraged the CNN's ability to transform anatomical information obtained from registered T1-weighted MRI scans and early observed noisy dynamic frames to simulate voxel-wise pseudo-weights (pWs) associated with the PCs (see Figure 3). This was accomplished through the utilization of three distinct 3DResUNet networks for domain translation tasks. These networks capture intricate spatial and temporal relationships within dynamic PET data. By employing a statistical mean model of PCs 4, along with pWs, and integrating correction terms derived from early frame observations, we predicted later 4D PET frames, albeit with some degree of uncertainty. Further improvement was achieved by concatenating observed early frames with predicted frames and iteratively applying the decomposition using corrected PCs. Building upon the PCA decomposition outlined in Figure 1, we reconstructed the 4D dynamic PET images through an inverse-PCA process.Results
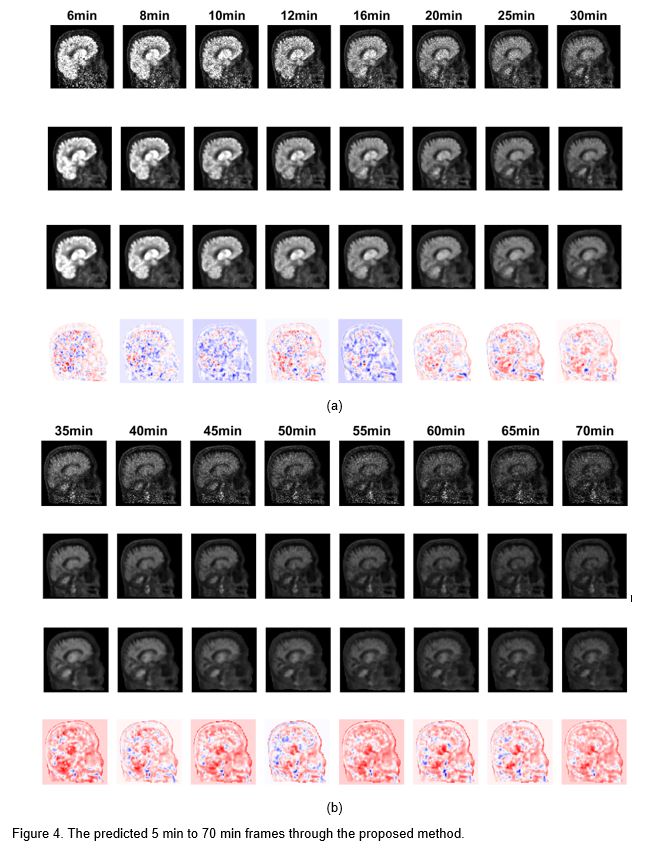
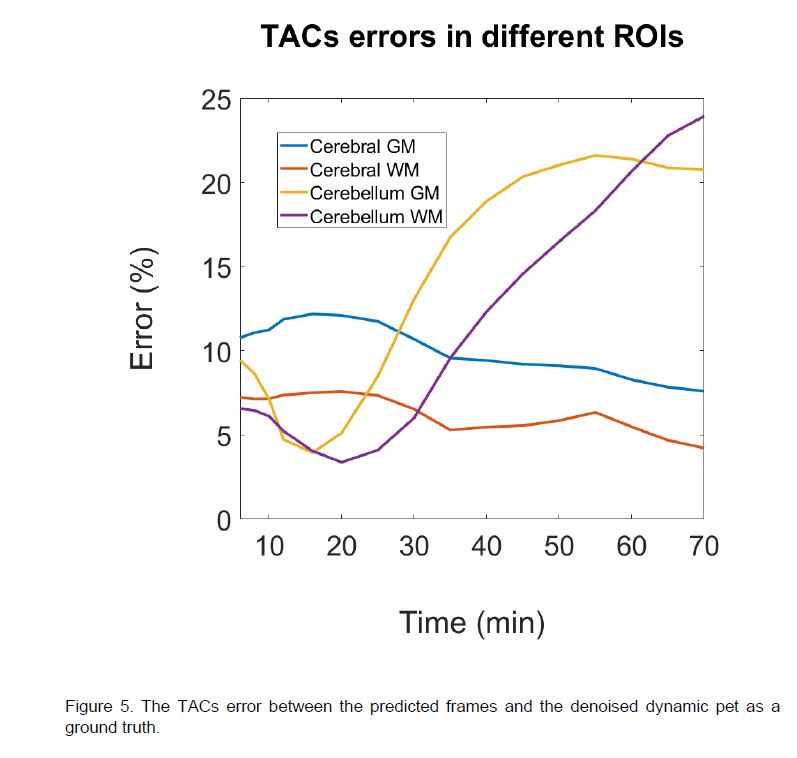
We analyzed data from 77 patients who underwent 4D 18F_AV45 brain PET imaging with MRI scanners. FLIRT registration was applied to the MRI data. Reconstruction involved 26 non-uniform list-mode data samples over 70 minutes, with the first 10 frames (0-5 minutes) as observations and the next 65 minutes predicted. We fitted the mean and each temporal PC model to the initial 5-minute data for inverse-PCA reconstruction. A CNN was trained using a diverse dataset of PC weights from 4D dynamic PET and T1-weighted MRI scans. Average MAE for T1 translation was 96.54%, 95.04%, and 96.22% for pW1, pW2, and pW3, respectively. The whole-brain MAE for predicting the last frame (65-70 minutes post-injection) was 35±7.7%. Total errors in TACs for specific tissues, cerebellum white matter, and gray matter were 12±2.7% and 19±2.7%, respectively (see Figure 5).Discussion
According to the temporal PCs model, the weights associated with the last frames predominantly correspond to the 2nd PCs, and the spatial weight images suggest that this PC is primarily associated with white matter regions, while the first weights image[HA1] linked to the PC1 is linked to gray matter. Furthermore, we observed that the 3rd PCs have a significant impact on early frame vessels and non-brain regions. It is important to note that the accuracy of these predictions generally improves with an increased number of observed frames. Extending the observation time from 5 minutes to 10 minutes resulted in an average decrease of 13±4.1% in the whole brain MAE. [HA1]what do you mean? First PC?Conclusion
Our objective is to develop a framework capable of predicting later frames from noisy early 4D PET frames. We achieved this goal by generating pWs from MRI data and iteratively combining them with statistical temporal PCs to predict the complete 4D PET dataset. This method holds significant promise for clinical applications, enabling clinicians to gain insights into dynamic physiological processes using early frame PET and routine MR anatomical scans. Moreover, the predicted image derived from anatomical and healthy subjects may be utilized to compare and identify abnormalities in patients.Acknowledgements
No acknowledgement found.References
[1] H Yousefi, C Ying, M Hamdi, R Laforest, H An, “An MR-assisted Spatiotemporal Approach for 4D Dynamic Brain PET Denoising” 2023 ISMRM & ISMRT Annual Meeting & Exhibition, Toronto, CA
[2] H Yousefi, C Ying, M Hamdi, R Laforest, H An, “4D Dynamic Brain PET Denoising with Spatiotemporal Regularization” 2023 AAPM 65th Annual Meeting & Exhibition, Houston, Tx, USA
[3] H. Yousefi, F. Mohammadi, N. Mirian and N. Amini, "Tuberculosis Bacilli Identification: A Novel Feature Extraction Approach via Statistical Shape and Color Models," 2020 19th IEEE International Conference on Machine Learning and Applications (ICMLA), Miami, FL, USA, 2020, pp. 366-371, doi: 10.1109/ICMLA51294.2020.00065.
[4] H. Yousefi, M. Fatehi, M. Bahrami and R. A. Zoroofi, "3D statistical shape models of radius bone for segmentation in multi resolution MRI data sets," 2014 21th Iranian Conference on Biomedical Engineering (ICBME), Tehran, Iran, 2014, pp. 246-251, doi: 10.1109/ICBME.2014.7043930.
Figures