1005
Deep Learning techniques to predict treatment outcomes in newly diagnosed epilepsy1Department of Neuroscience, Monash University, Melbourne, Australia, 2Department of Neurology, The Alfred Hospital, Melbourne, Australia, 3Department of Radiology, The Alfred Hospital, Melbourne, Australia
Synopsis
Keywords: Diagnosis/Prediction, Epilepsy, medication; depp learning
Motivation: Epilepsy is a complex neurological disorder with a high degree of heterogeneity. Selecting the appropriate antiseizure medication(ASM) is a time-consuming trial-and-error process that requires expert knowledge from neurologists.
Goal(s): Our goal was to utilise Deep Learning(DL) techniques with neuroimaging information to predict the treatment outcome of ASM.
Approach: We developed a DL model that utilises multi-modal information (MRI scans and clinical characteristics) to predict seizure outcomes of initial ASM for patients with newly diagnosed epilepsy.
Results: Our model achieved AUROC/AUPRC of 0.72/0.71 respectively in predicting treatment outcomes, demonstrating the potential of brain MRI scans as a biomarker for treatment response.
Impact: The model showed promise for development of decision-support systems that could help neurologists select the best ASM, potentially improving treatment outcomes. Clinical translation will require larger datasets and external validation, but this work implies that MRI contains additional prognostic information.
Introduction
Traditional anti-seizure medications (ASMs) are not always effective in treating epilepsy, and many patients continue to experience seizures despite treatment1. Recently, there has been growing interest in using deep learning (DL) algorithms to predict treatment outcomes for various disorders, including epilepsy. However, existing DL models for epilepsy prediction often lack interpretability, generalisability, and struggle to account for the heterogeneity of presentations of epilepsy in patients. Our research aims to address these limitations by developing a novel DL-based model that utilises multimodal information to accurately determine the treatment outcome in newly diagnosed epilepsy patients, thereby personalising treatment options.Research Methods and Design
DatasetWe retrospectively studied a cohort of 96 patients with newly diagnosed epilepsy from The Alfred Hospital, Melbourne who were heterogeneous in terms of their seizure type, seizure focus location, age, sex, underlying pathology, and comorbidities, and assessed their seizure control at 1 year after commencement of the prescribed ASM. All the patients were diagnosed according to the criteria defined by the ILAE including a comprehensive neurological evaluation, EEG recordings, and diagnostic MRI scans.
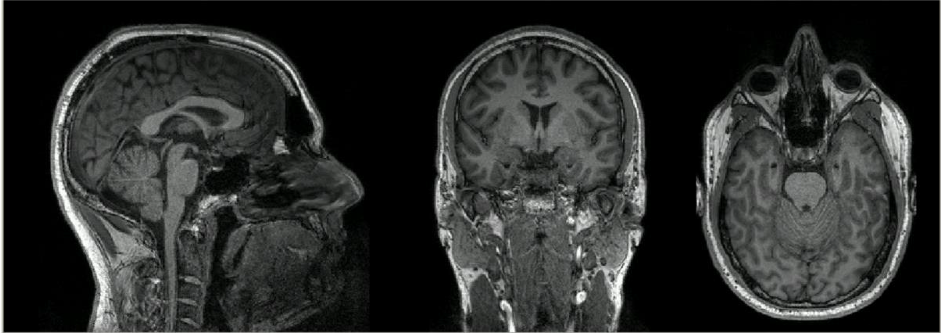
All the eligible patients were scanned on a 3T Siemens Magnetom Prisma or Skyra MRI machine at the Alfred Hospital, Melbourne and one of the images can be located in figure 2.
The images were acquired using a T1-weighted Magnetization-Prepared Rapid Acquisition Gradient Echo(MPRAGE) sequence, with the following parameters : repetition time(ms):2300.0, echo time(ms):3.03, inversion time (ms):900, flip angle= 9 degrees, slices:192 and slice thickness(mm):0.90.
Image Preprocessing
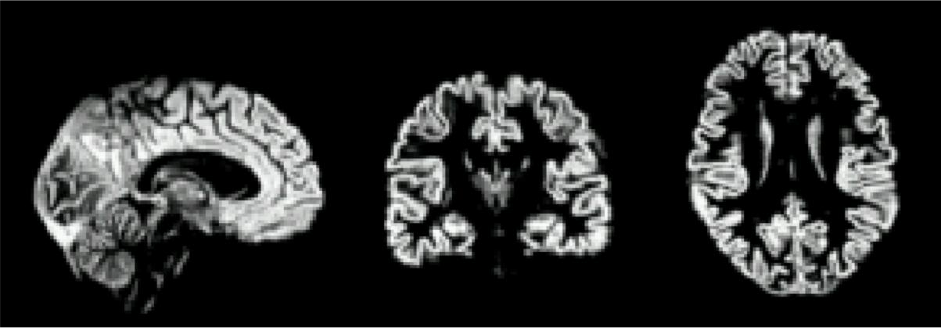
We performed tissue segmentation using voxel-based morphometry to obtain grey-matter concentration(GMC) using FSL-VBM which can be seen in figure 3. The grey matter concentration was non-linearly registered to the ICBM-MNI152 standard template with a voxel dimension of 1 mm3. After registration of the images, we performed intensity scaling, histogram normalisation and resizing of all the non-linearly registered grey matter images from training and validation datasets, to a dimension of 128x128x128.
Model Training
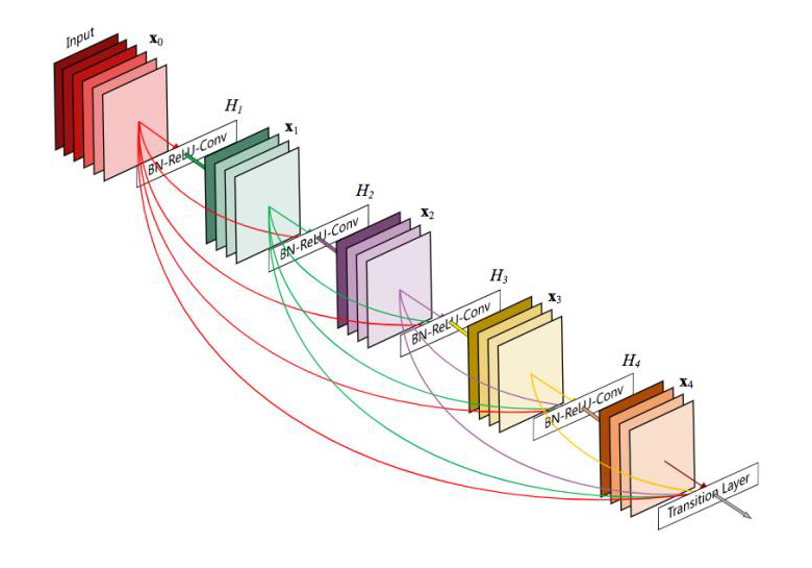
Our study employed a DenseNet121 model2 with 15 input channels to accommodate multimodal inputs, including image features, ASM indicator labels, and clinical features. A generic architecture of the model is mentioned in figure 1. The model had 2 output channels to calculate the probability of seizure freedom (defined as no seizure while taking the first antiseizure medication at 12 months) and non-seizure freedom for each subject. We used the Adam optimizer with an initial learning rate of 1e-4 and L2 norm regularization with a weight decay of 1e-5. Early stopping was implemented to prevent overfitting, where the training loop was terminated once the model performance on the validation set stopped improving over a certain number of epochs, as described by Bai et al. (2021)3 and Prechelt et al. (2002)4. Models were trained on batches of 20 samples for a maximum of 80 epochs during each fold.
Model evaluation and statistics
We used area under the receiver-operating characteristic curve(AUROC) and area under precision-recall (AUPRC) curve as the evaluation metrics to judge the performance of the model in classifying the patients into seizure freedom and non-seizure freedom categories. AUROC and AUPRC were chosen as they are threshold-invariant metrics, eliminating the need for threshold calibration giving a more comprehensive assessment of our model's predictive performance.
Results
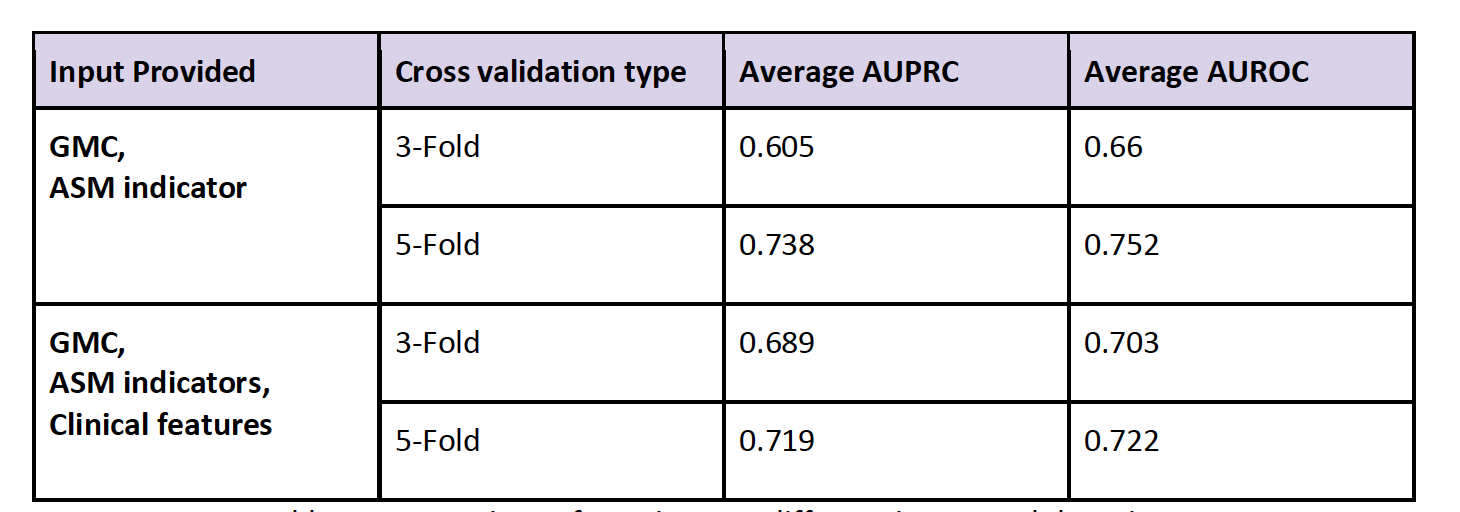
Our end-to-end deep learning model enabled us to predict the treatment outcome for each of the ASMs for a patient using the GMC derived from MRI scan and clinical characteristics of the patient. The base model with GMC and ASM indicators as input variables gave an average AUPRC/AUROC of 0.60/0.66 respectively, indicating “poor” but above chance performance with 3-fold cross-validation. Using 5-fold cross-validation improved the AUPRC/AUROC of 0.74-0.75 respectively, indicating “fair” performance5. Whereas the model trained with GMC, ASM indicators and clinical features has consistently provided “fair” performance across different training samples, indicating better generalisability due to added features. The summary statistics are provided in Table 1.Discussion
We proposed to utilise the relevant clinical information and included the patient’s MRI scan of the brain to effectively identify appropriate ASMs for our study cohort. While this is a challenging task, given the complexity in the morphology, biochemistry and connectivity of neurons, our model has achieved an AUROC and AUPRC of 0.72-0.75 on a varied, heterogenous group of patients. The strength that our model offers is the ease of scaling to more modalities by the addition of multi-modal information in the model. As of now, we have limited ourselves to using a single MRI sequence and some relevant clinical characteristics. In the future, we could trivially add multiple MRI sequences, where available, with very few changes required for our codebase.Acknowledgements
We acknowledge the contribution of the participants from The Alfred Hospital, Melbourne for their participation. This project was funded by NHMRC Ideas grant no. GNT2010382.References
1. Chen, Zhibin, et al. "Treatment outcomes in patients with newly diagnosed epilepsy treated with established and new antiepileptic drugs: a 30-year longitudinal cohort study." JAMA neurology 75.3 (2018): 279-286.
2.Huang, Gao, et al. "Densely connected convolutional networks." Proceedings of the IEEE conference on computer vision and pattern recognition. 2017.
3. Bai, Yingbin, et al. "Understanding and improving early stopping for learning with noisy labels." Advances in Neural Information Processing Systems 34 (2021): 24392-24403.
4. Prechelt, Lutz. "Early stopping-but when?." Neural Networks: Tricks of the trade. Berlin, Heidelberg: Springer Berlin Heidelberg, 2002. 55-69.
5. Nahm, Francis Sahngun. "Receiver operating characteristic curve: overview and practical use for clinicians." Korean journal of anesthesiology 75.1 (2022): 25-36.
Figures