0990
CSF Outflow and Egress in Optic Nerve: Non-contrast MRI Revelations1Radiology, University of California San Diego, San Diego, CA, United States
Synopsis
Keywords: Neurofluids, Neurofluids
Motivation: The rose of cerebrospinal fluid (CSF) in neural health is recognized, yet its outflow and egress within the optic nerve, especially amidst new findings about the glymphatic system, remains less explored.
Goal(s): Investigate CSF interactions within the optic nerve using advanced MRI techniques, highlighting implications for conditions like glaucoma.
Approach: Utilized advanced Time-Slip sequences on a 3-T MR imager, targeting specific brain regions to study CSF outflow and egress.
Results: Clear CSF egress pathways through the optic nerve were found, with distinct outflow influenced by participants’ optical attributes.
Impact: Enhances understanding of CSF outflow and egress, providing pivotal insights for addressing neuro-ophthalmological disorders like glaucoma.
Introduction
The cerebrospinal fluid (CSF) plays essential roles in safeguarding neural structures and waste removal (1). Recent studies have introduced the concept of a “glymphatic system”, suggesting that the CSF enters the brain through the perivascular space and moves through the brain parenchyma, aiding in waste removal (2, 3). This process has been further elucidated by contrast MRI studies, which have identified the parasagittal dura (PSD) as a potential pathway for brain clearance (3, 4). Furthermore, advanced non-contrast, spin-labelling MRI techniques have highlighted the unique route of the upper PSD in directing CSF to the superior sagittal sinus (5). However, its outflow and egress, especially its interaction within the optic nerve, remains enigmatic, prompting interest given the potential implications for disorders like glaucoma. The optic nerve’s unique positioning, being sheathed within meningeal layers (6) continuous with those of the CNS, presents opportunities for CSF interaction. This study, leveraging advanced imaging techniques, seeks to elucidate these outflow and egress.Methods
The study was approved by the Institutional Review Board. All MR imaging data were obtained with a clinical 3-T MR imager (Vantage Galan 3T, Canon Medical Systems, Japan) in 6 healthy subjects without any neuro-ophthalmological disease (3 males and 3 females; mean age 28 9.87 years; range, 19 – 48 years), 2 of these volunteers wore glasses (nearsighted). 2D Time-SLIP with tag-on and tag-off acquisitions using TEeff of 300 ms (to eliminate the contamination of blood signals) with varying TI periods. The tag was placed on the optic nerve (5-mm tag) and then on the mid brain (100-mm tag).Results
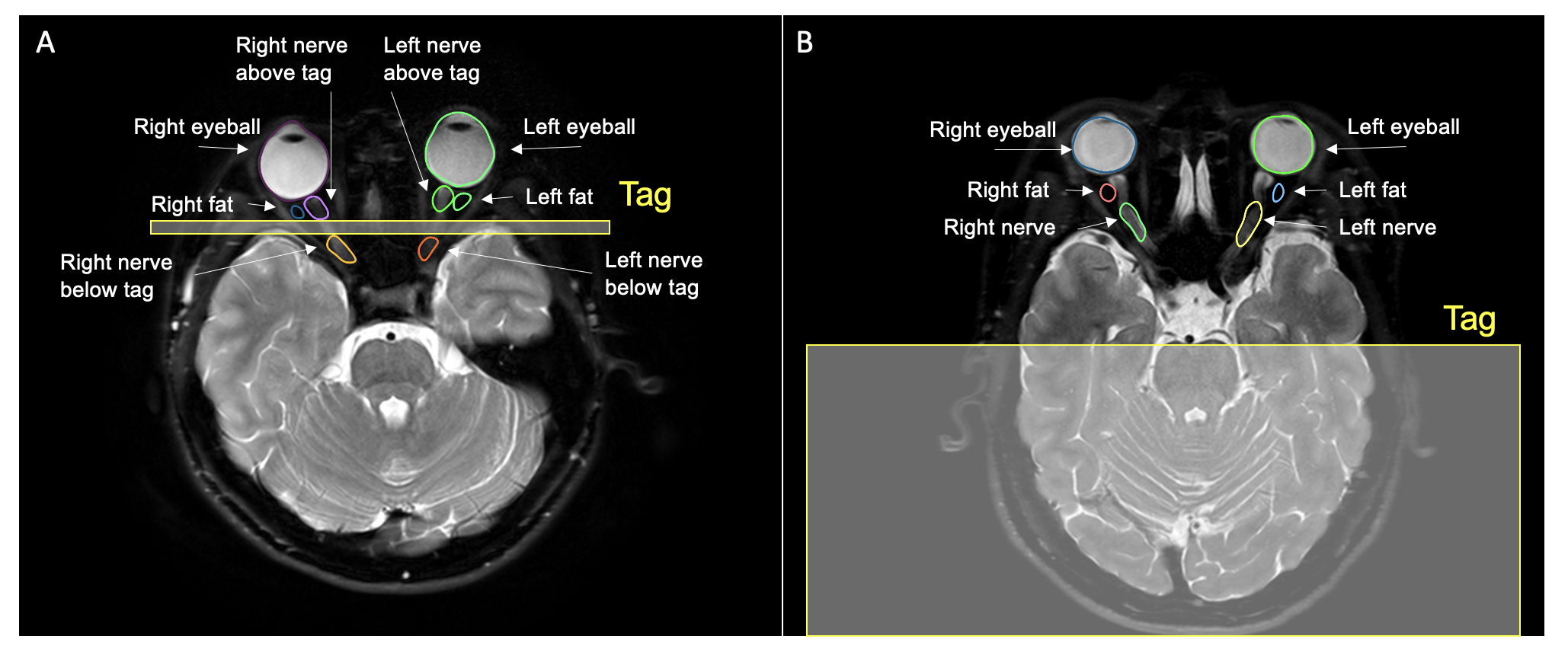
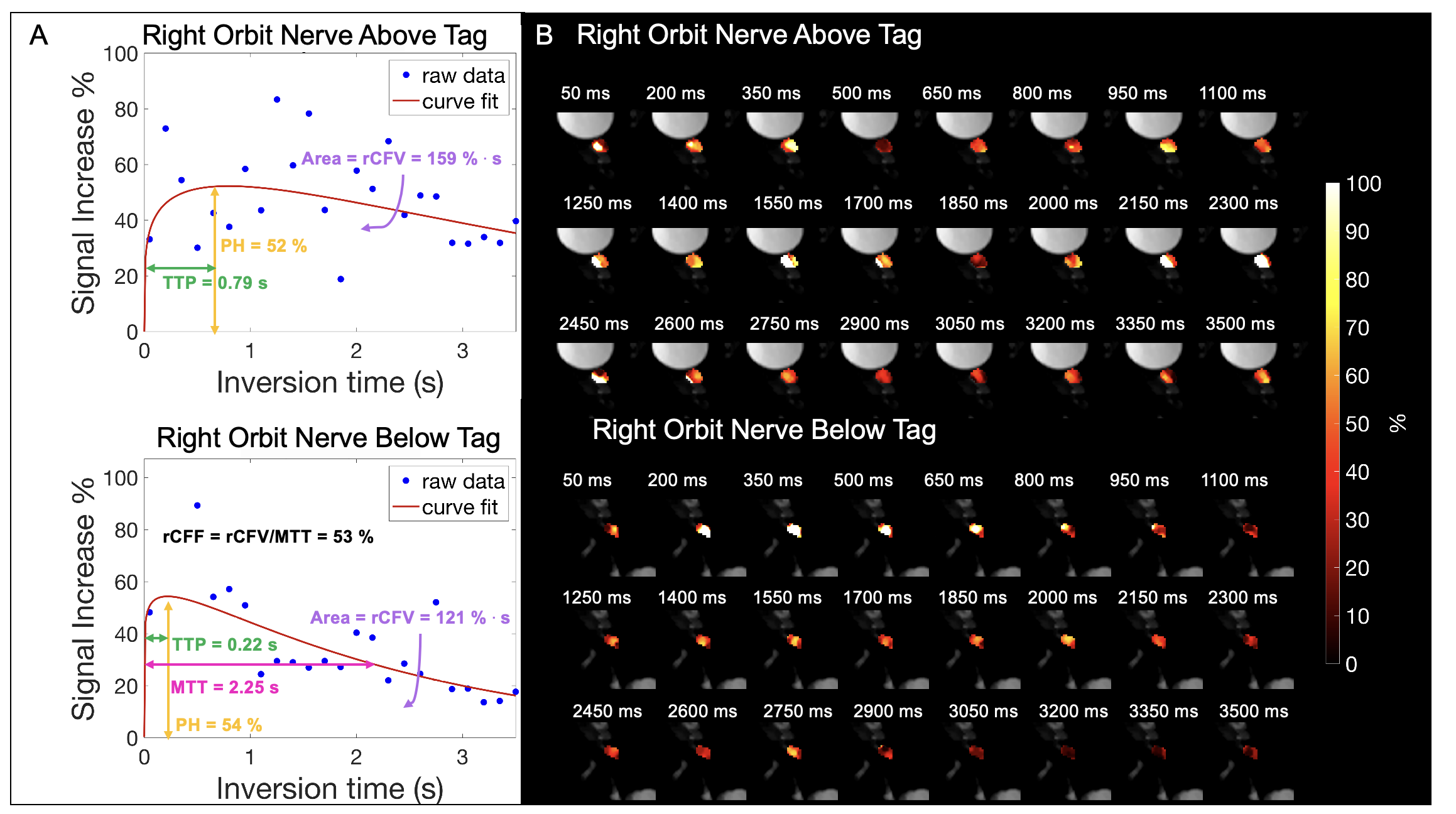
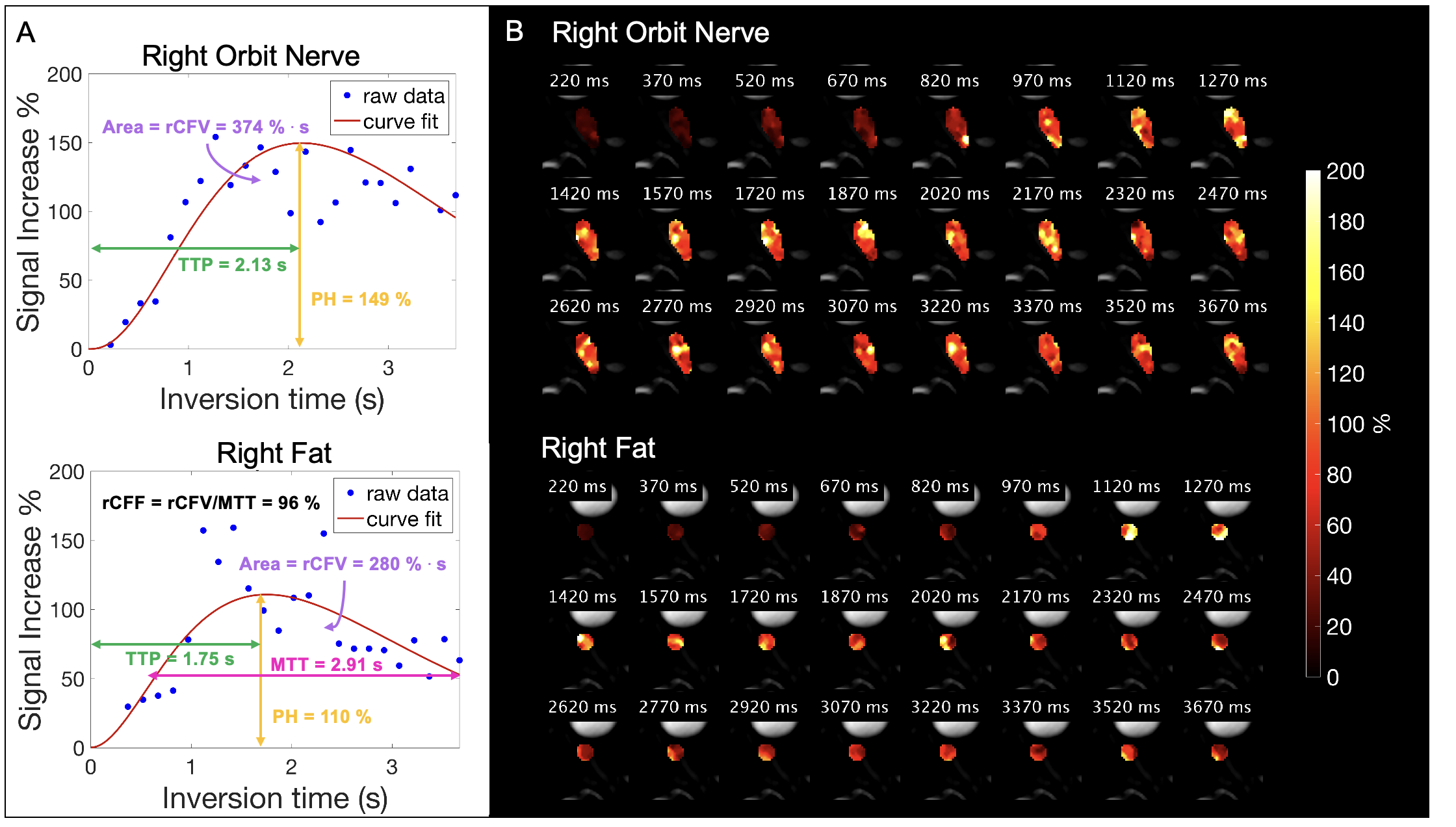
Clear indications of CSF egress through the optic nerve were identified. Visual representation in Figure 1A indicates the tagged region on the optic nerve with Figure 1B showcasing the tag on the mid-brain, accompanied by the specific regions of interest (ROIs). Using 2D Time-SLIP with the optic nerve tagged, we detected prominent CSF signals around the eyeball’s perimeter, extending to the nerve and the adjacent fat tissue. We observed the tagged CSF moved bidirectionally. The Signal Intensity Ratio (SIR) plots are detailed in Figure 2A, while Figure 2B presents the corresponding fusion images of SIR over tag-off image. Shifting the tag to the mid-brain resulted in observable CSF egress in all ROI’s. The Time to Peak (TTP) on the optic nerve and fat was increased, measuring 2.06s +/- 0.13, and 1.97s +/- 0.3, respectively, compared to 0.675s +/- 0.2, and 0.54s +/- 0.33 when the tag was on the optic nerve. The SIR and fusion images for these ROIs are illustrated in Figures 3A and 3B.A particularly striking observation emerged when comparing the participants based on their use of glasses. Those who wore glasses displayed significantly lower Peak Height (PH) and Relative CSF volume (rCFV) values in the eyeball (PH% =25 +/- 3.38, rCFV % . s = 54.7 +/- 9.75) and in the optic nerve regions both above (PH%= 42.4 +/- 14, rCFV % . s = 131 +/- 39.8) and below (PH% = 40.1 +/- 17, rCFV % . s = 107 +/- 42) the tag. In contrast, participants without glasses had substantially higher readings (eyeball: PH% = 103 +/- 18, rCFV % . s = 220.9 +/- 22.7; optic nerve above: PH%= 132 +/- 12, rCFV % . s = 388 +/- 101; and optic nerve below: PH%= 163 +/- 23, rCFV % . s = 547 +/- 88).Discussion
The optic nerve’s pivotal role as a conduit for CSF egress, especially its outflow and egress movement from the mid-brain, underscores its central relevance in neuro-ophthalmological fluid outflow. The implications of this become evident when we look at interventions such as the use of silicone oil tamponades in retinal treatments. While these tamponades are employed for complex retinal detachments, there’s growing concern about the unintended migration of silicone oil into the brain ventricles (7-11). How does silicone oil navigate this pathway? If CSF can traverse through the optic nerve, as our observations have indicated, it’s plausible that analogous transport routes or outflow might facilitate the progression of substances like silicone oil. Further highlighting the optic nerve’s significance, our data revealed discernible variations in the PH and rCFV values based on the participants’ use of glasses. This raises intriguing questions about the nexus between optical corrections, such as nearsightedness, and CSF outflow.Conclusion
We found 1) CSF in the midbrain communicates with the optical nerve roots, and 2) CSF to move bi-directionally in the orbit nerve. The interplay between CSF egress outflow and visual parameters provides a promising avenue for future neuro-ophthalmological research and potential therapeutic strategies.Acknowledgements
This work was supported by an NIH grant RF1AG076692 (M.M.) and a grant by Canon Medical Systems, Japan (35938).References
[1] Nedergaard M. Science, 2013; 340(6140), 1529–1530.
[2] Iliff JJ, Wang M, Zeppenfeld DM, et al. J of Neurosci, 2013; 33(46) ,18190–18199.
[3] Absinta M, Ha SK, Nair G, et al. eLife, 2017; 6:e29738.
[4] Ringstad G, and Eide PK. Nat Commun, 2020; 11:354.
[5] Miyazaki M, Malis V, Kungsamutr, Yamamoto A, McDonald MA, McEvoy LK, Bae W. Magn Reason Med Sci. (2023).
[6] Killer, H.E., Laeng, H.R., Flammer, J., & Groscurth, P. The British Journal of Ophthalmology, 2003; 87(6), 777-781.
[7] Potts, M.B., Wu, A.C., Rusinak, D.J., Kesavabhotla, K., & Jahromi, B.S.. World Neurosurgery, 2018; 115, 201-205.
[8] Guo, L.Y., Jamiolkowski, R.M., Hassan, M., & Leng, T. American Journal of Ophthalmology Case Reports, 2022; 25, 101399.
[9] Grzybowski, A., Pieczynski, J., & Ascaso, F.J. Acta Opthalmologica, 2014; 92, 201-204.
[10] Knecht, P., Groscurth, P., Ziegler, U., Laeng, H.R., Jaggi, G.P., & Killer, H.E. British Journal of Ophthalmology, 2007; 91(10), 1293-1295.
[11] Gnanalingham, J., Mcreary, R., Charles, S., & et al. Case Reports, 2017; bcr-2017-220555.
Figures