0989
Altered perivascular CSF mobility in human cerebral amyloid angiopathy1Clinic for Neuroradiology, Universityclinic Bonn, Bonn, Germany, 2German Center for Neurodegenerative Diseases (DZNE), Bonn, Germany, 3Clinic for Neurology, Universityclinic Bonn, Bonn, Germany
Synopsis
Keywords: Neurofluids, Neurofluids, Brain Clearance
Motivation: Perivascular spaces (PVS) are mediating brain clearance, i.e. cerebrospinal fluid (CSF) - interstitial fluid exchange, and dilated PVS are a hallmark of cerebral amyloid angiopathy (CAA). However, until now, brain clearance function could not be assessed in humans in vivo.
Goal(s): Goal of this study was to assess perivascular cerebrospinal fluid (CSF) mobility in CAA patients.
Approach: A CSF mobility-specific 7-Tesla MRI sequence was applied for the first time in patients with CAA and healthy control (HC) subjects.
Results: The study revealed perturbed CSF mobility in enlarged perivascular spaces in CAA compared to HC subjects, suggesting impaired perivascular clearance in CAA.
Impact: With the finding of a perturbed CSF mobility in enlarged PVS in CAA patients, the study provides proof-of-principal for in vivo measurements of perivascular CSF mobility as a crucial component of the brain clearance pathway in health and disease.
Background
Cerebral amyloid angiopathy (CAA) is a common age-related pathology characterized by the progressive accumulation of amyloid-β around cerebral blood vessels. CAA is a major cause of spontaneous intracerebral hemorrhage and age-related cognitive decline. Dilated perivascular spaces (PVS) in the white matter centrum semiovale (CSO) visible by MRI are a hallmark of CAA. PVS represent a major conduit for the clearance of parenchymal waste products, including amyloid-β, along perivascular routes into the cerebrospinal fluid (CSF) and the lymphatic system. Accordingly, impaired brain clearance and subsequent vascular amyloid-β deposition have emerged as critical early steps in the pathogenesis of CAA. A recent rodent study revealed increased CSF flow in the large CSF compartments and along the large arteries at the base of the skull [1]. However, CSF dynamics in humans as well as smaller PVS within the brain parenchyma – the actual location of CSF-interstitial fluid (ISF) exchange – has not been addressed so far. Therefore, this study aimed to quantify the CSF mobility in parenchymal PVS in patients with probable CAA diagnosed in accordance with the modified Boston Criteria and age-matched healthy control (HC) subjects.Methods
A 7.0 Tesla MRI sequence was applied that was recently developed specifically for perivascular CSF mobility quantification (Fig. 1) and had shown promising results in pre-clinical studies [2-3]. The high-resolution CSF mobility sequence (0.50mm3) combines a long echo time (TE = 515 ms) for CSF isolation with a T2-prepared module with flow-sensitizing gradients (low b-value diffusion encoding) (Fig. 2). Within the CSF mobility sequence, seven image sets (4:15 min each), one without and six with differently orientated crushers (b0-b6), were acquired to create a diffusion tensor imaging (DTI)-like tensor. Image reconstruction of the 12x poisson-disk undersampled data was achieved using “pics” from the BART Toolbox for Computational Magnetic Resonance Imaging. The b0-b6 images were interpolated to a 0.17 mm3 resolution and co-registered. Subsequently, DTI postprocessing was performed using Python 3.10 to assess diffusion-like parameters such as the CSF mobility [mm²/s], which is equivalent to the apparent diffusion coefficient (ADC) on traditional DTI data. Parcellated atlases from T1w imaging data were constructed using the Freesurfer software package (Version 6.0). White matter segmentations, derived from the Freesurfer parcellation, were further processed to compute segmentations of the centrum semiovale (CSO). PVS within the CSO segmentation were semiautomatically segmented using a Meijering filter-based approach on the interpolated b0 image. PVS segmentations were used to classify PVS as either medium-to-large sized (large sized) if the segmentation still existed after a simple (double) erosion of the corresponding PVS segmentation. Finally, the CSF mobility was extracted for the PVS in the CSO of eight CAA patients and nine HC subjects.Results
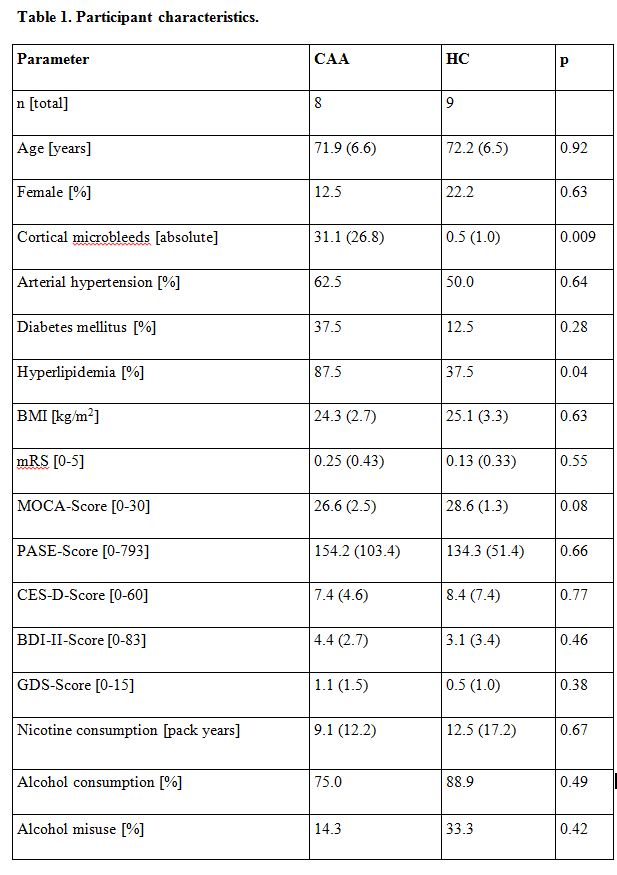
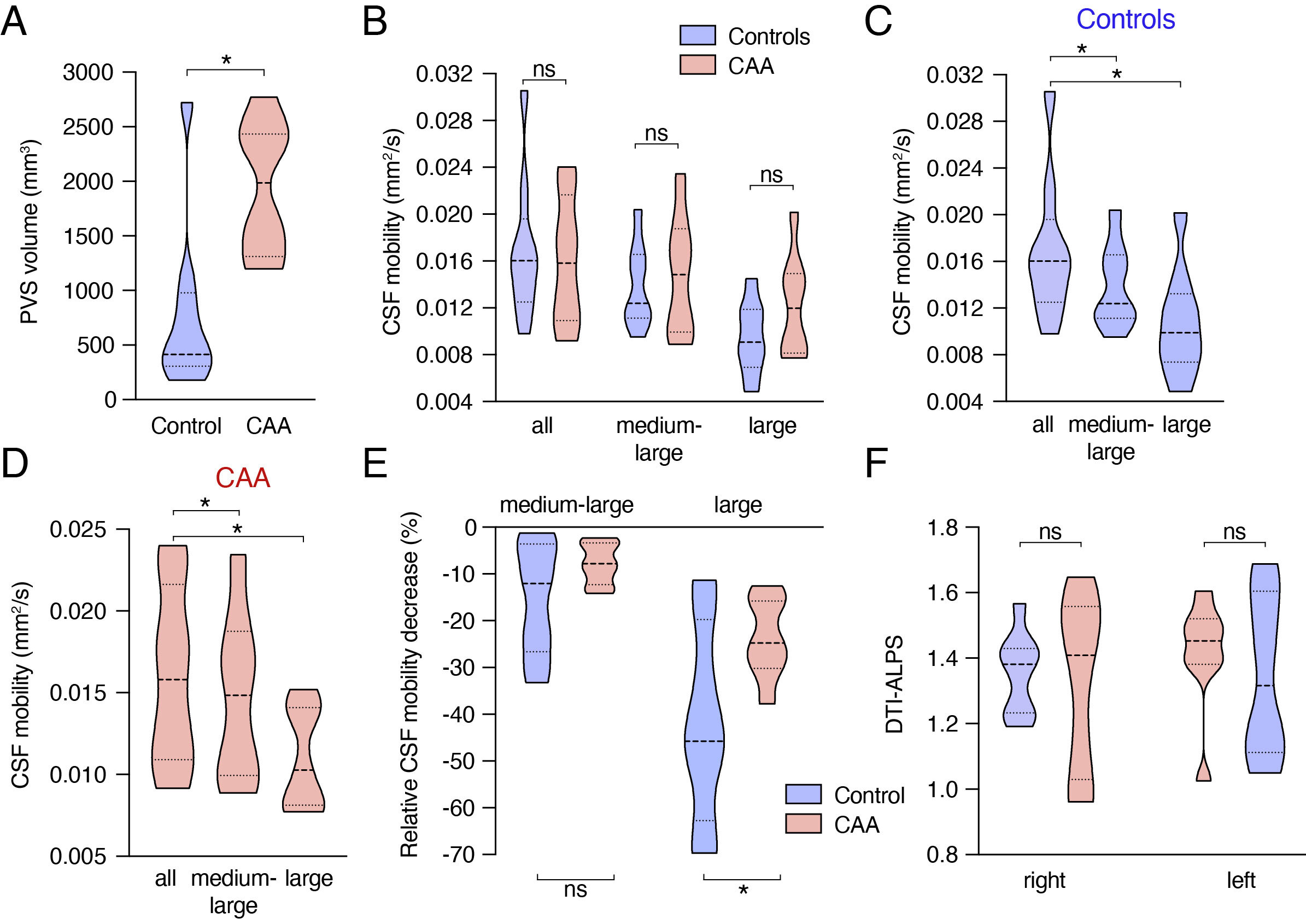
Age, gender, lifestyle factors as well as cognitive and physical health scores did not differ between both groups (Fig. 3). CAA patients had significantly higher PVS volumes than HC (Fig. 4). Descriptive analysis of CSF mobility stratified by group and PVS size revealed a drop in CSF mobility and larger group differences in enlarged PVS (CCAA = 0.016 (0.008) mm²/s, CHC = 0.016 (0.005) mm²/s, CCAA_L= 0.012 (0.006) mm²/s, CHC_L= 0.009 (0.004) mm²/s). To futher explore the correlation between CSF mobility and PVS size in both groups, mobility changes were expressed in medium-to-large PVS and large PVS as percental values relative to CSF mobility in PVS of all sizes (Fig.4). This analysis revealed that the relative drop in CSF mobility within large PVS was significantly attenuated in CAA compared to HC (HC = -45.7 %, CAA = -24.8 %, p < 0.05).Discussion
The study provides the first in vivo evidence for increased CSF mobility in enlarged parenchymal PVS in human CAA. Interestingly, such an increased CSF flow was also recently reported in a rat model of CAA in extraparenchymal large arteries at the base of the brain [3]. That study also found that flow vectors in large CSF spaces were diverted away from the parenchyma in transgenic animals, suggesting that reduced CSF flow into parenchymal PVS may be expected. Instead, we found an increased CSF mobility in parenchymal PVS. The current study can neither reveal the pathophysiological link between both findings, nor does CSF mobility allow drawing conclusions on direction of CSF flow or net flow.Conclusion
The presented CSF mobility measurements represent a central part of the overall clearance pathway as they cover the immediate events upstream of perivascular CSF - ISF exchange. Therefore, this novel MR toolbox for non-invasive, in vivo, perivascular CSF mobility quantification may allow for comparative investigations of brain clearance in health and disease.Acknowledgements
This study was supported by the EU - Joint Platform for Neurodegenerative Diseases (JPND).References
[1] Chen X, Liu X, Koundal S, et al. Cerebral amyloid angiopathy is associated with glymphatic transport reduction and time-delayed solute drainage along the neck arteries. Nat Aging. 2022;2(3):214-223. doi:10.1038/s43587-022-00181-4
[2] Van Osch MJP, Petitclerc L, Hirschler L. Probing cerebrospinal fluid mobility for human brain clearance imaging MRI: water transport across the blood-cerebrospinal fluid barrier and mobility of cerebrospinal fluid in perivascular spaces. Veins Lymphat. 2022;11(1). doi:10.4081/vl.2022.109422.
[3] Harrison IF, Siow B, Akilo AB, et al. Non-invasive imaging of CSF-mediated brain clearance pathways via assessment of perivascular fluid movement with diffusion tensor MRI. Elife. Published online 2018. doi:10.7554/eLife.34028.0013.
Figures
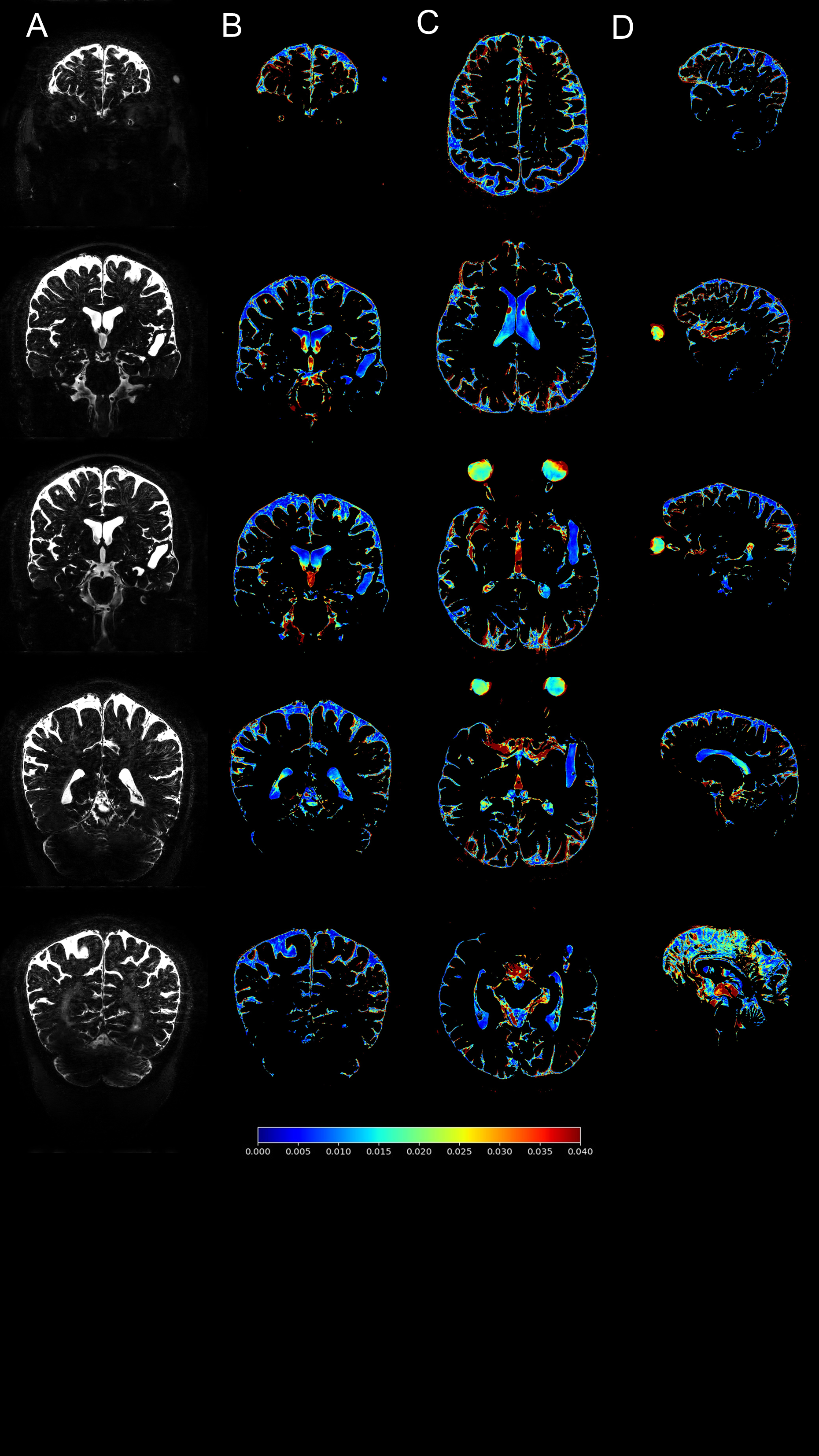
Figure 1, Example of cerebrospinal fluid (CSF) mobility sequence
(A) Coronal b0 image as well as corresponding CSF mobility map in coronal (B), axial (C) as well as sagittal (D) orientation. The color encodes CSF mobility in [mm²/s].
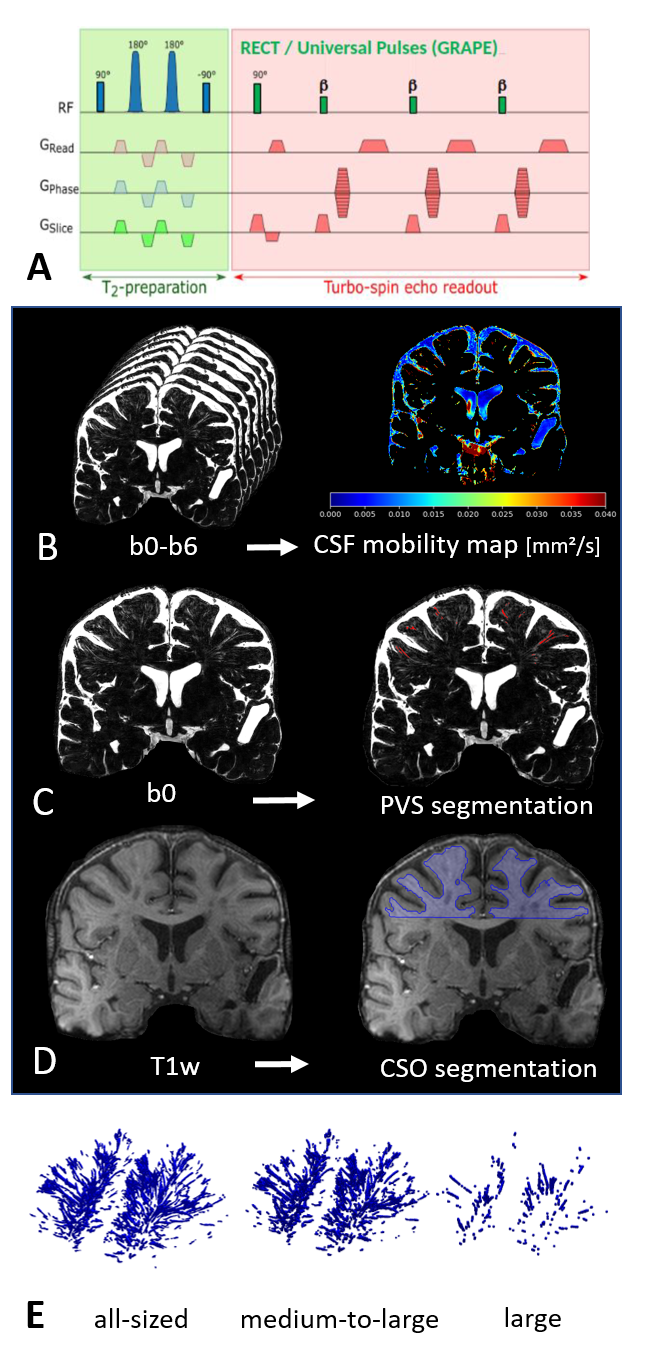
Figure 2, Workflow of Image Acquisition and Postprocessing
(A) Schematic of the cerebrospinal fluid (CSF) mobility sequence. Seven image stacks (b0-6) are acquired that are used to calculate a DTI-like tensor (B). Semi-automatic segmentation of the perivascular spaces (PVS) is performed with a Meijering filter-based approach on the b0 image (C) and segmentation of the centrum semiovale (CSO) is conducted automatically by fressurfer on the T1-weighting (D). (E) depicts the PVS segmentation mask of all PVS as well as stratified by PVS size.