0984
Advancing Estimation of Microvascular Perfusion in the Choroid Plexus through Inversion Recovery Prepared IVIM MRI1Bernard and Irene Schwartz Center for Biomedical Imaging, Department of Radiology, New York University Grossman School of Medicine, New York, NY, United States, 2Center for Advanced Imaging Innovation and Research (CAI2R), Department of Radiology, New York University Grossman School of Medicine, New York, NY, United States, 3Vilcek Institute of Graduate Biomedical Sciences, New York University Grossman School of Medicine, New York, NY, United States
Synopsis
Keywords: Neurofluids, Diffusion/other diffusion imaging techniques, IVIM, diffusion, choroid plexus
Motivation: Measuring vascular perfusion in the Choroid Plexus (ChP) is challenging due to its smaller size and the pronounced partial volume effects from CSF.
Goal(s): To improve blood perfusion assessment of ChP utilizing Inversion recovery (IR) prepared IVIM imaging.
Approach: Higher in-plane resolution (1.5x1.5mm2) IVIM diffusion MRI data with and without the IR preparation were acquired. The signal was analyzed using inverse Laplace transform (ILT) to estimate diffusion compartments within ChP for IVIM-derived perfusion fraction analysis.
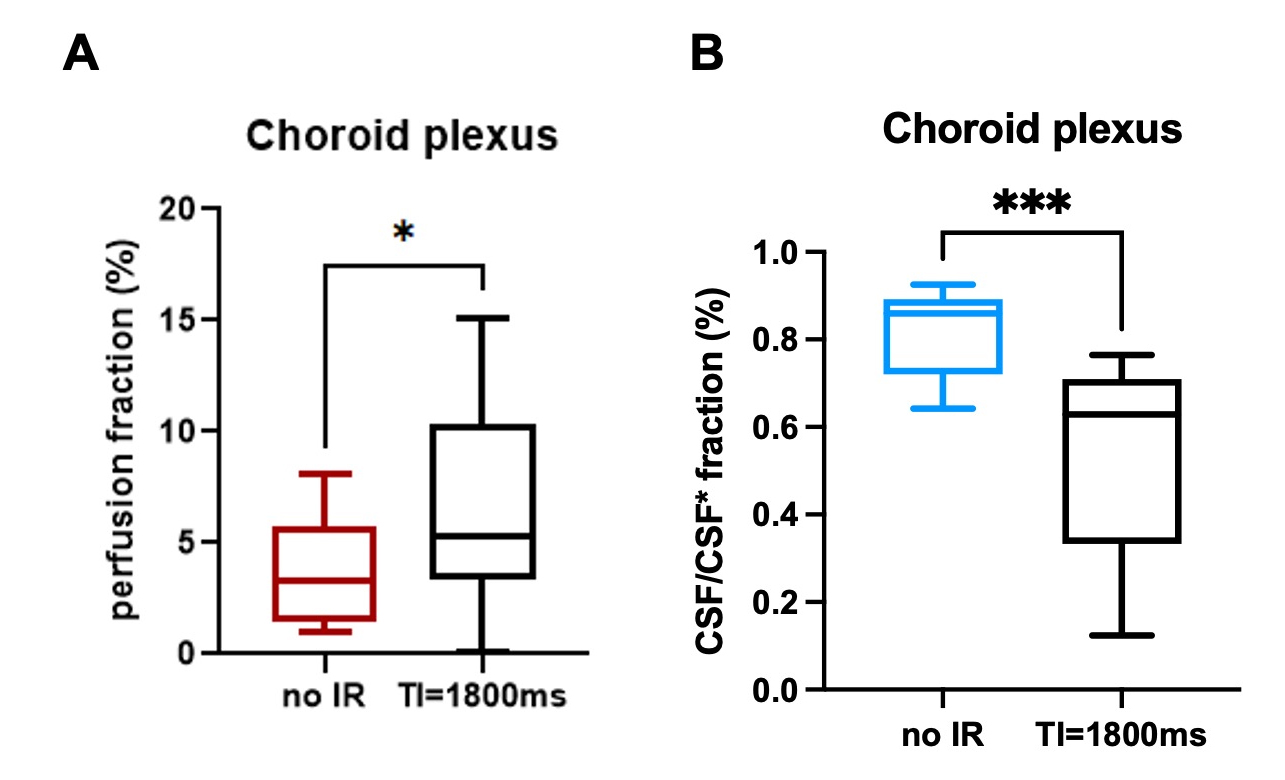
Results: ILT analysis of IR-prepared IVIM revealed three diffusion compartments within the ChP and reported higher perfusion fraction observed in IR-prepared IVIM versus IVIM without IR-preparation.
Impact: This study provides a novel approach to investigate the microvascular perfusion in Choroid Plexus (ChP) with CSF signal removed. IR preparation does not completely remove the free-diffusion compartment but increases the microvascular perfusion fraction estimation in ChP.
Introduction
Choroid plexus (ChP), situated within the ventricles of the brain, is a highly vascularized structure responsible for CSF production1,2, serving as the primary site of the blood-CSF barrier, and enabling water exchange between the capillary bed and the CSF3. Given its distinctive function, investigating ChP perfusion can provide valuable insights into the vascular functional dynamics of the ChP and its connection to CSF production and waste clearance. However, assessing microvascular perfusion in the ChP poses a considerable challenge. The ChP’s relatively small size, poor image contrast, and its location within the CSF-filled ventricles lead to inevitable interference and substantial partial volume effects from the CSF in current image resolution4,5. Intravoxel-incoherent motion (IVIM) has emerged as an alternative technique sensitive to microvascular perfusion in diffusion-weighted images6. However, at low b-values, the perfusion signal can become mixed with signal from freely moving CSF7,8. Therefore, the objective of this study is to assess vascular perfusion in the ChP using Inversion recovery (IR) preparation within IVIM framework to effectively attenuate the CSF signal, and subsequently compare the results with those obtained through conventional IVIM without IR preparation.Materials and methods
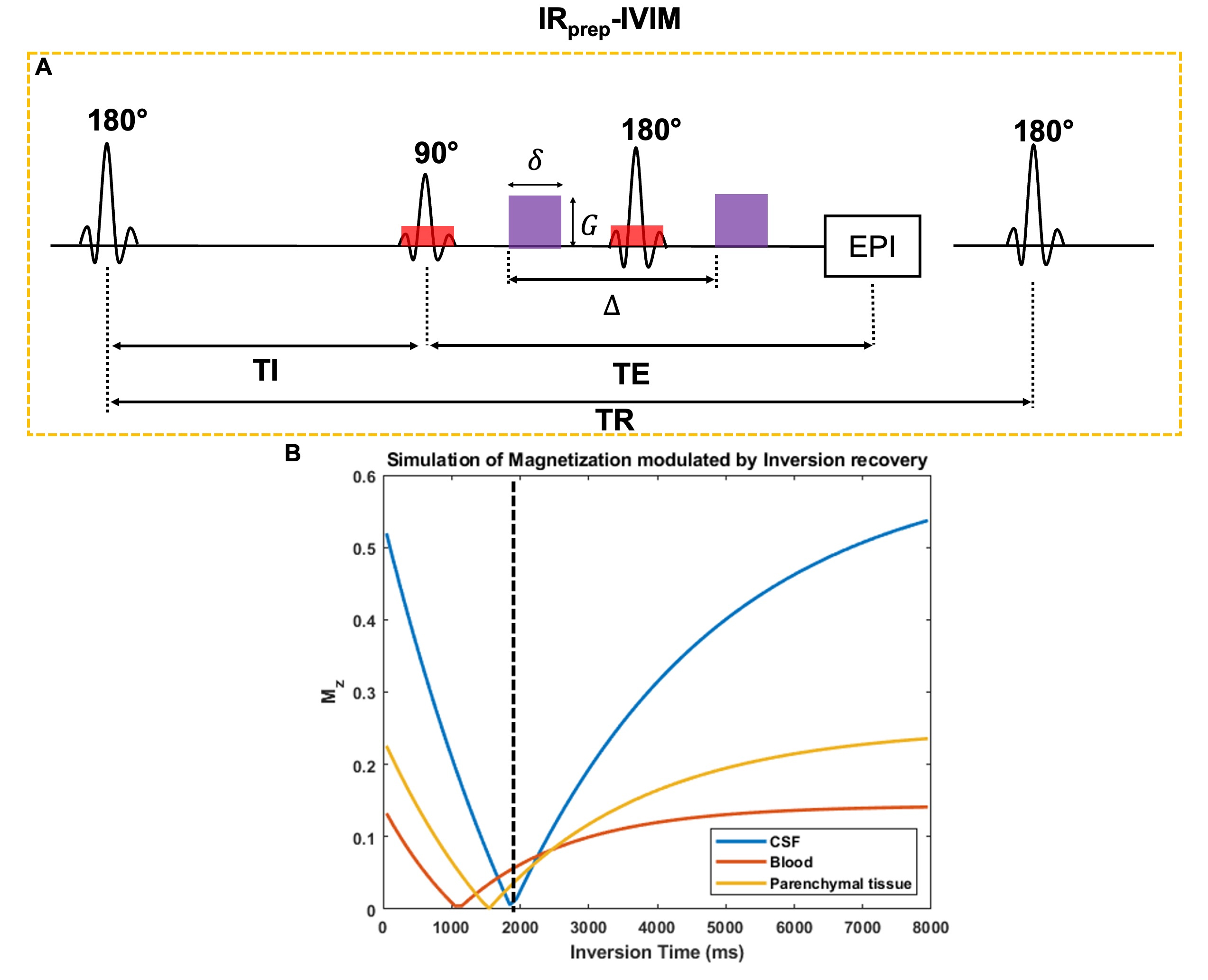
In this study, a total of 14 subjects (averaged age: 68.1±12.2 years, F/M=9/5) were enrolled. For anatomical reference, T2-FLAIR and SWI were acquired to examine the vascular and structual abnormalities in ChP using the following parameters: (1) T2-FLAIR: TE/TR=438/4800ms, voxel size: 1mm*1mm*1.2mm. (2) Flow compensated SWI: TE/TR=22.5/38ms, voxel size: 0.3mm*0.3mm*1.5mm. (3) IRprep-IVIM data was acquired using a Stejskal-Tanner diffusion-weighted spin-echo echo-planar imaging (EPI) pulse sequence (TR/TE/TI = 8000/72/1800 ms, voxel size: 1.5mm*1.5mm*3mm). (4) A paired IVIM sequence (without IR module but with same TR) was also acquired to compare the results with IRprep-IVIM. Fifteen b–values (0, 10, 20, 30, 40, 50, 100, 150, 200, 300, 400, 500, 650, 800 and 1000 s/mm2) were implemented. The diffusion direction was in slice direction only. The total acquisition time including both with and without the IR module, was 5 mins 32s. To account for T1 effects induced by the IR, the diffusion data were normalized with their individual S0 values. To analyze the diffusion spectrum, an inverse Laplace transform (ILT) was applied on both IVIM datasets to derive the diffusivity and its distribution within each of three tissue compartments (i.e., vascular, stroma, CSF) within the ChP9.Results
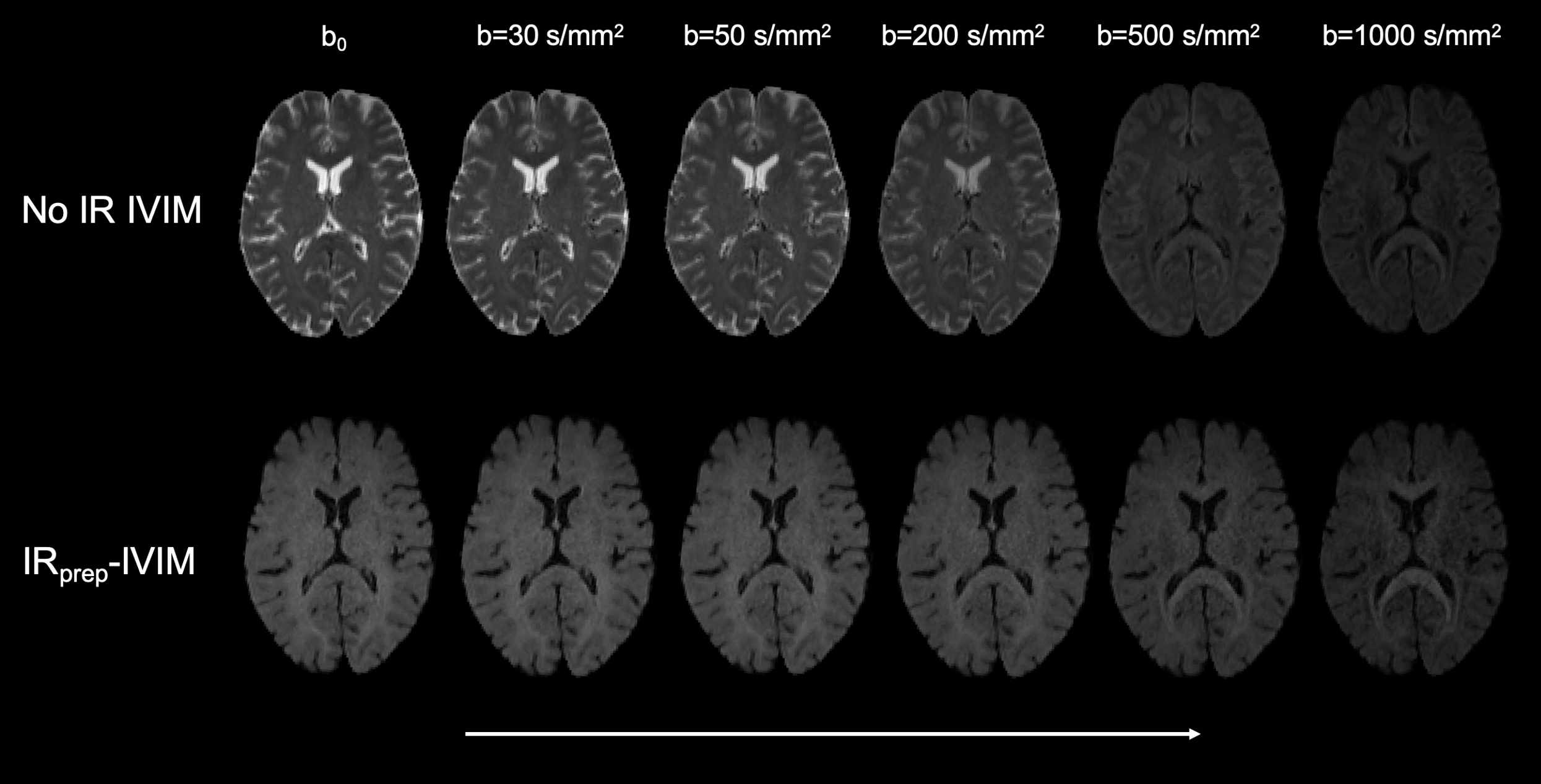
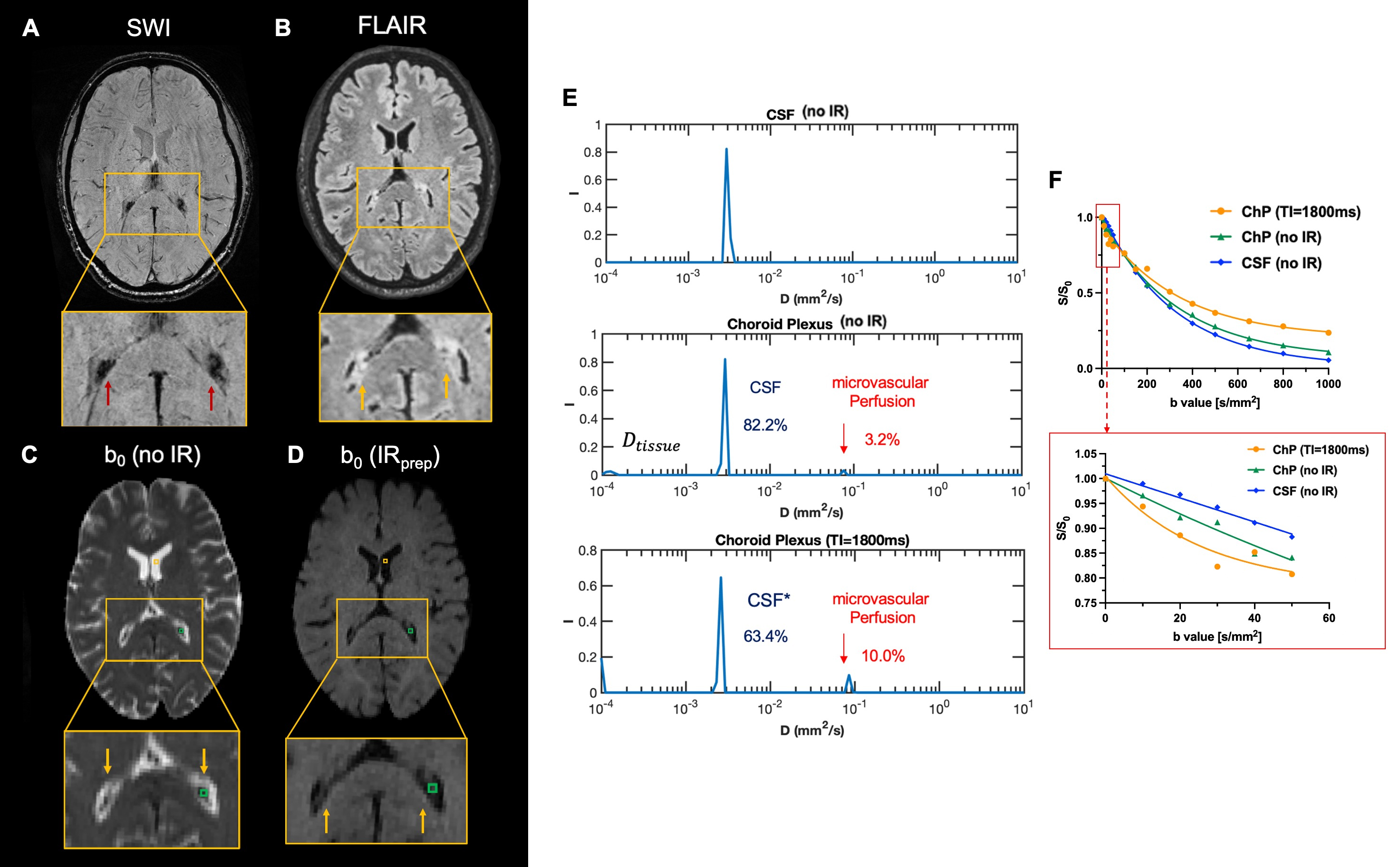
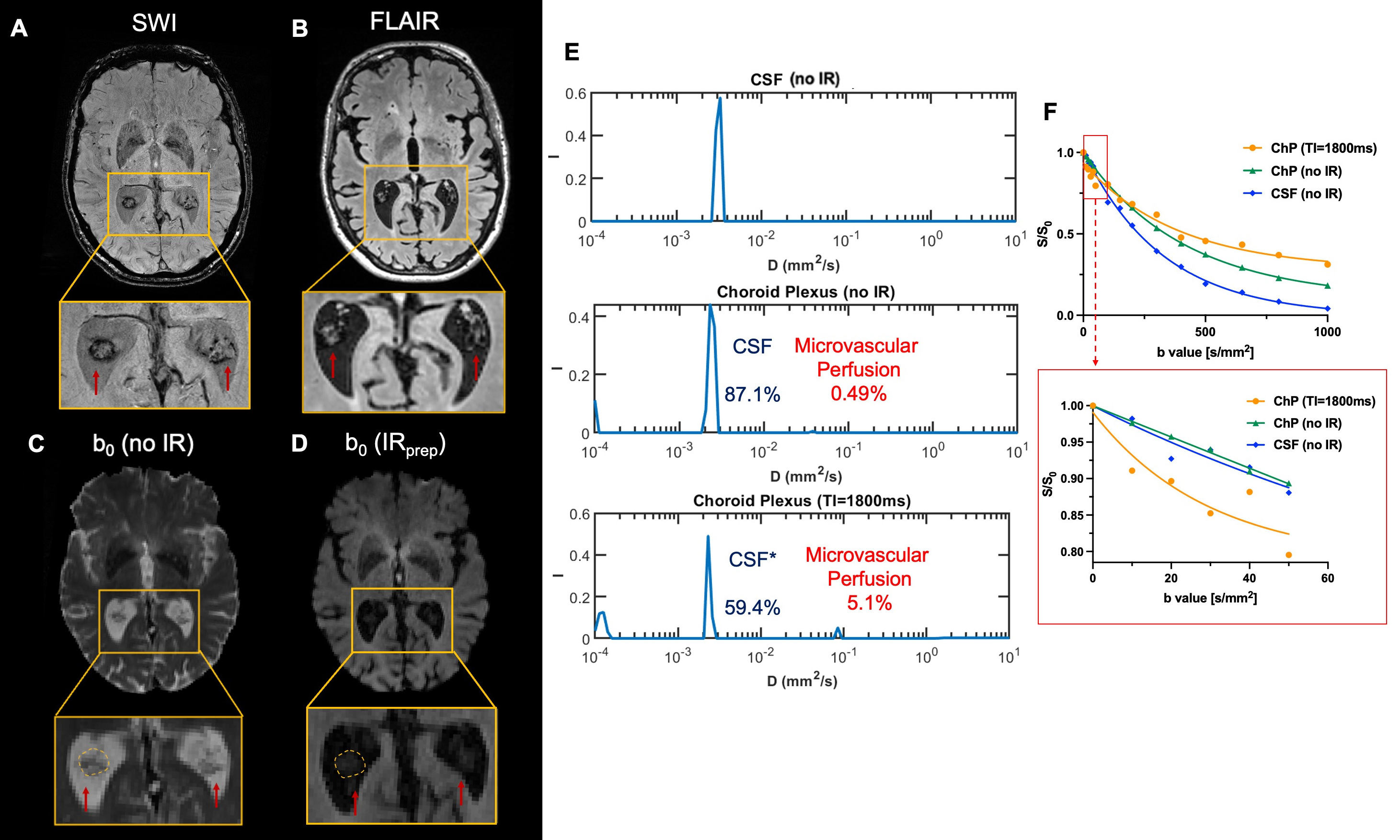
Figure 1 shows the simulation IVIM data with and without the inversion recovery (IR) preparation. Notably, the b0 images reveal the effective suppression of the signal originating from CSF. Representative images in Figure 2 illustrate the IVIM signal decay for free CSF within ventricle at different b values in two datasets: with and without IR. Figure 3 shows stronger IVIM effects were observed in ChP with IR. ILT analysis further revealed three tissue compartments within the ChP, which potentially indicates the stromal tissue diffusion, CSF and microvascular perfusion. Notably, while the bulk CSF signal is eliminated following IR, ILT sill revealed fluid-like structures characterized by higher diffusivity, but discernibly distinct from CSF within the stroma tissue. Figure 4 shows another example of an elderly subject with enlarged choroid plexus along with a reduced perfusion fraction. A comparison between conventional IVIM and IRprep-IVIM technique revealed a higher perfusion fraction and reduced CSF fractions in the IRprep-IVIM data.Conclusion and discussion
In this study, we employed the IRprep-IVIM to investigate microvascular perfusion in ChP, effectively eliminating the CSF signal,z and compared the results with non-IR prepared IVIM data. Instead of using bi-exponential models for IVIM analysis, we analyzed the data using ILT that allows for the analysis of IVIM signals without assuming a specific number of diffusion compartments. Our findings revealed a departure from a two-compartment model, which typically involves tissue and microvascular perfusion, in the IVIM signal of the choroid plexus. Instead, a three-compartment model emerged, suggesting the presence of stromal diffusion, CSF, and microvascular components. Even after the IR process, which effectively suppressed the bulk CSF signals, we observed a peak (CSF*) in the signal that exhibited similar diffusivity with CSF9. This peak might correspond to interstitial fluid or other cyst-like structure with similar diffusivity but distinct T1 relaxation times, or residual unsupressed CSF. Consequently, the employed inversion time may not entirely eliminate this signal. An alternative explanation is that the IVIM signal encodes CSF exchange between ventricle and ChP10,11,12. To validate these observations, further investigations using time-dependent IVIM analysis are warranted. In summary, our study presents a novel approach to explore ChP vascular perfusion with minimizing the impact of CSF partial volume, potentially shedding light in the intricate hemodynamics of ChP.Acknowledgements
This work was performed under the rubric of the Center for Advanced Imaging Innovation and Research (CAI2R, www.cai2r.net), an NIBIB National Center for Biomedical Imaging and Bioengineering (NIH P41 EB017183).References
1. Cserr, HELEN F. "Physiology of the choroid plexus." Physiological reviews 51.2 (1971): 273-311.
2. Damkier, Helle H., Peter D. Brown, and Jeppe Praetorius. "Cerebrospinal fluid secretion by the choroid plexus." Physiological reviews 93.4 (2013): 1847-1892.
3. MacAulay, Nanna. "Molecular mechanisms of brain water transport." Nature Reviews Neuroscience 22.6 (2021): 326-344.
4. Zhao, Li, et al. "Non-invasive measurement of choroid plexus apparent blood flow with arterial spin labeling." Fluids and Barriers of the CNS 17 (2020): 1-11.
5. Eisma, Jarrod J., et al. "Choroid plexus perfusion and bulk cerebrospinal fluid flow across the adult lifespan." Journal of Cerebral Blood Flow & Metabolism 43.2 (2023): 269-280.
6. Le Bihan, Denis. "What can we see with IVIM MRI?." Neuroimage 187 (2019): 56-67.
7. Rydhög, Anna, et al. "Estimation of diffusion, perfusion and fractional volumes using a multi-compartment relaxation-compensated intravoxel incoherent motion (IVIM) signal model." European Journal of Radiology Open 6 (2019): 198-205.
8. Rydhög, Anna S., et al. "Separating blood and water: Perfusion and free water elimination from diffusion MRI in the human brain." Neuroimage 156 (2017): 423-434.
9. Wong, Sau May, et al. "Spectral diffusion analysis of intravoxel incoherent motion MRI in cerebral small vessel disease." Journal of Magnetic Resonance Imaging 51.4 (2020): 1170-1180.
10. Li, Anna M., and Jiadi Xu. "Cerebrospinal fluid‐tissue exchange revealed by phase alternate labeling with null recovery MRI." Magnetic resonance in medicine 87.3 (2022): 1207-1217.
11. Li, Anna M., et al. "Age‐dependent cerebrospinal fluid‐tissue water exchange detected by magnetization transfer indirect spin labeling MRI." Magnetic resonance in medicine 87.5 (2022): 2287-2298.
12. Jiang, Dengrong, et al. "Quantification of T1 and T2 of subarachnoid CSF: Implications for water exchange between CSF and brain tissues." Magnetic resonance in medicine 90.6 (2023): 2411-2419.
Figures