0975
In-vivo evidence for cell body loss in cortical lesions in people with multiple sclerosis1Department of Neurology, Massachusetts General Hospital, Harvard Medical School, Boston, MA, United States, 2MS Center Amsterdam, Anatomy and Neurosciences, Amsterdam Neuroscience, Amsterdam UMC location VUmc, Amsterdam, Netherlands, 3Athinoula A. Martinos Center for Biomedical Imaging, Department of Radiology, Massachusetts General Hospital, Harvard Medical School, Charlestown, MA, United States
Synopsis
Keywords: Multiple Sclerosis, Neurodegeneration, High-Field MRI, Diffusion Modelling, Tissue Characterization
Motivation: Cortical lesions are linked to irreversible cortical atrophy as well as cognitive impairment in multiple sclerosis. High-gradient diffusion MRI is sensitive to the microstructural substrate of neurodegeneration in multiple sclerosis.
Goal(s): To identify in-vivo patterns of cell body density alterations, quantified by advanced diffusion MRI, in and surrounding focal cortical demyelination in people with multiple sclerosis.
Approach: The intra-cellular signal fraction, reflective of cell body density, was compared between cortical lesions, perilesional and normal-appearing cortex.
Results: Multiple sclerosis-related decreases in intra-cellular signal fraction were seen in cortical lesions compared to perilesional and normal-appearing cortex.
Impact: High-gradient diffusion MRI has the potential to identify cortical cell body loss in-vivo, potentially attributable to focal demyelination, relevant for cognition.
Introduction
Focal cortical demyelination has been linked to cognitive impairment and irreversible neurodegeneration in people with multiple sclerosis (MS)1,2. The microstructural effects of cortical lesions attributable to cortical atrophy and subsequently cognitive deterioration are not fully delineated. High-gradient diffusion MRI has shown potential to identify cell body density alterations, reflected by the soma and neurite density imaging (SANDI) model, preceding cortical volume loss3. Therefore, the aim of present study was to identify in-vivo alterations in SANDI measures in and surrounding focal cortical demyelination in people with MS.Methods
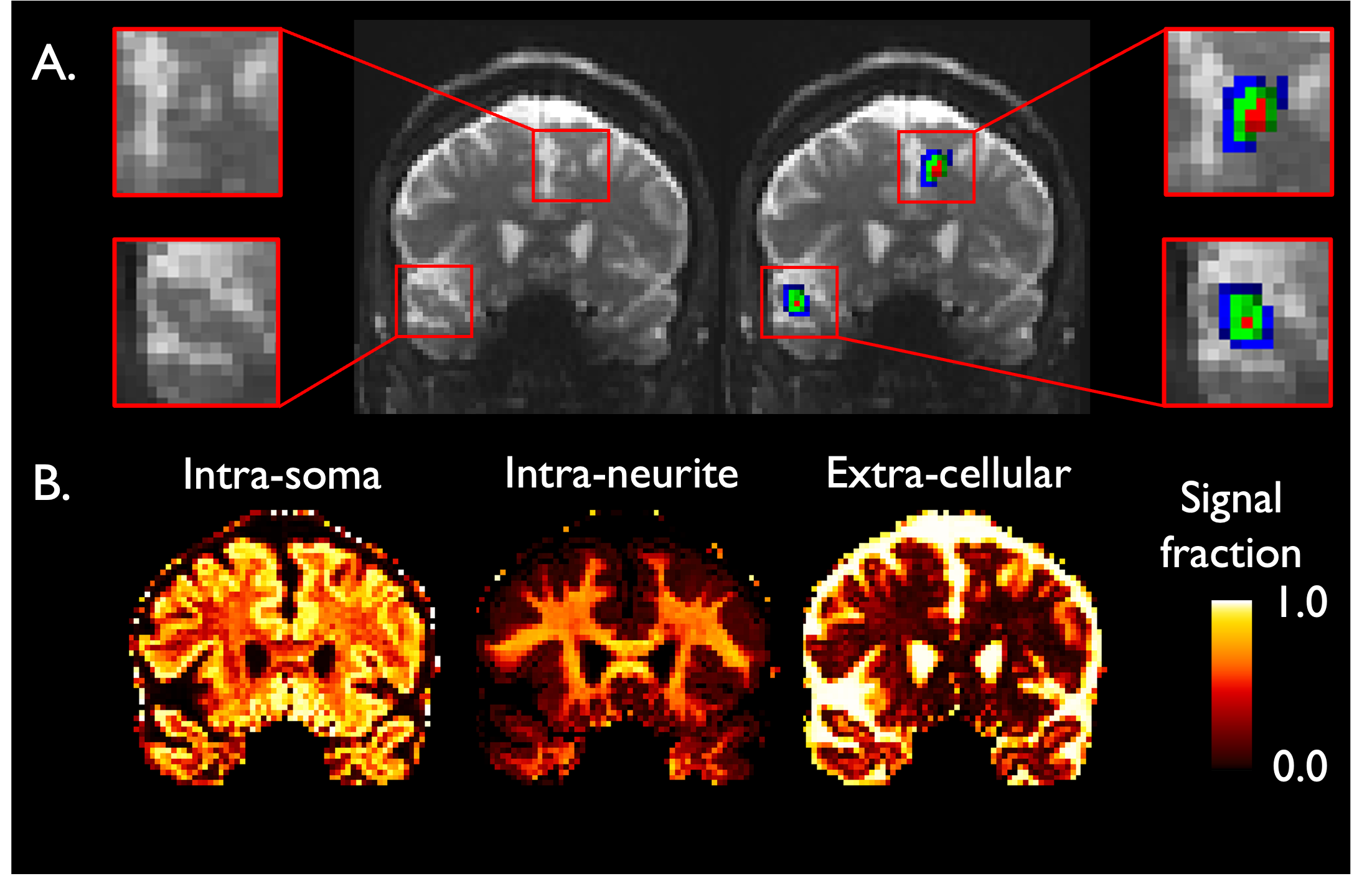
This cross-sectional study included 41 people with MS and 34 age- and sex-matched healthy controls (HC) who underwent 3T MRI (MAGNETOM Connectom, Siemens Healthcare) equipped with 300mT/m gradients using a multi-shell diffusion MRI acquisition protocol consisting of eight b-values (diffusion time=19ms) at 2mm isotropic resolution3. All people with MS underwent neuropsychological testing. An average cognition Z-score was calculated based on Z-scores of seven predefined cognitive domains. Cortical lesions were segmented on artificial intelligence-generated double inversion recovery images derived from MEMPRAGE and FLAIR sequences4. Perilesional tissue was segmented as two expanding shells each measuring 2mm in thickness surrounding every lesion (‘inner’ and ‘outer’ perilesional layers; Figure 1A). Perilesional layers were intersected with cerebrospinal fluid (CSF) and white matter masks to exclude CSF and white matter contamination. The SANDI model5 was fitted to the diffusion data to obtain estimates of intra-cellular (fsoma), intra-neurite (fneurite) and extra-cellular (fextra) signal fractions in cortical lesions and normal-appearing cortex (Figure 1B). SANDI measures were compared between MS and HC. Within people with MS, SANDI measures were compared between cortical lesions, inner and outer peri-lesional layers and normal-appearing cortex by applying paired t-tests. Linear regression models were performed for the correlation between relevant SANDI measures and average cognition.Results
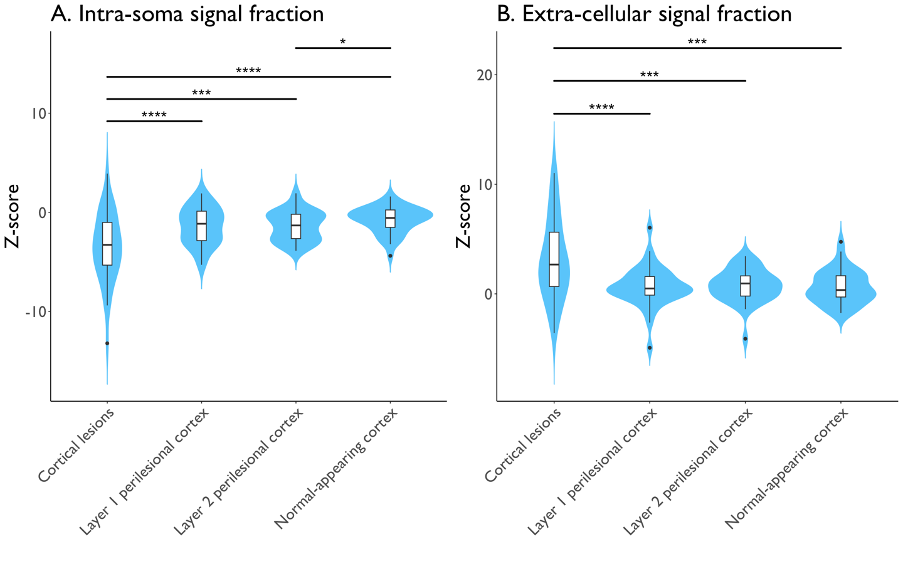
40 out of 41 people with MS (97.6%) had at least one cortical lesion. People with MS showed lower normalized cortical volumes compared to HC (P<0.001). The entire cortex of people with MS (0.56±0.03) showed lower fsoma compared to HC (0.58±0.03) (Pcorr=0.030). The fextra of the entire cortex in people with MS (0.26±0.04) tended to be lower compared to HC (0.25±0.02) (Pcorr=0.085). Cortical fneurite did not show significant alterations in MS.Compared to the cortex of HC, fsoma was lower in cortical lesions (Pcorr<0.001), perilesional layers (both Pcorr<0.001), and normal-appearing cortex (Pcorr=0.012), and fextra was significantly higher in cortical lesions (Pcorr<0.001) and the outer perilesional layer (Pcorr=0.014). Within people with MS, cortical lesions showed a significant lower fsoma with higher variability and higher fextra compared to perilesional and normal-appearing cortex (Pcorr<0.001 for all; Figure 2). The fsoma of the outer layer of perilesional cortex was lower compared to the normal-appearing cortex (Pcorr=0.028).
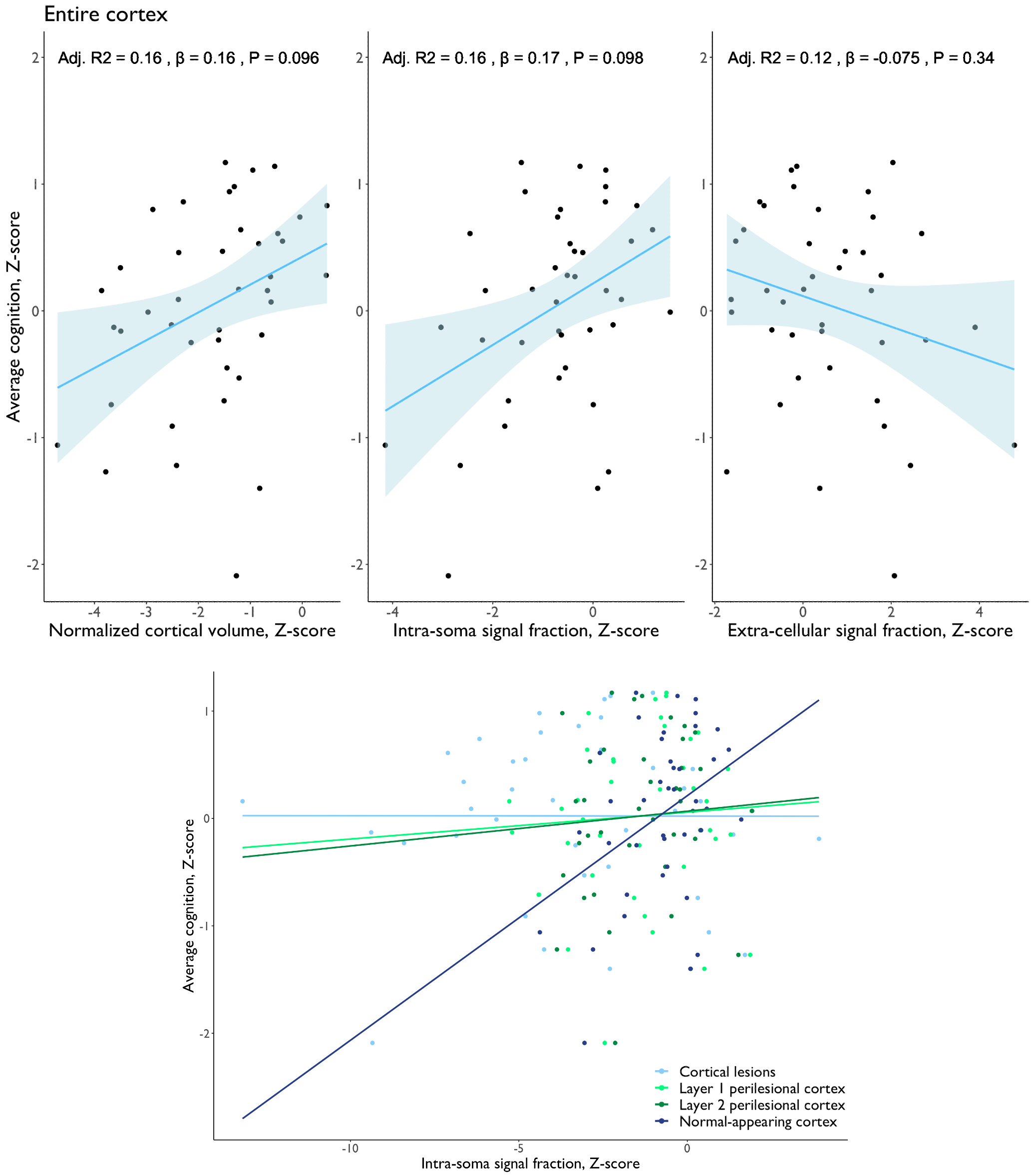
Our cohort of predominantly relapsing-remitting MS had a mean Z-score of average cognition of 0, reflecting no to mild overall cognitive impairment in our sample. Still, linear regression models showed trends towards positive relationships between average cognition and normalized cortical volume (P=0.096) and fsoma (P=0.098; Figure 3). Normal-appearing cortex fsoma was more strongly associated with average cognition than lesional fsoma.
Discussion
Cortical lesions had lower cell body density reflected by lower fsoma compared to normal-appearing cortex. The variability in cell body density was greater in cortical lesions than normal-appearing cortex, reflecting the heterogeneity of cortical pathology. Based on histopathology and PET-MRI studies, demyelinated cortex is characterized by reduced neuronal density but increased inflammatory activity compared to normal-appearing and healthy cortex6,7. Our results provide in-vivo evidence of reduced neuronal density occurring within and just outside cortical lesions. The gradient of decreasing cell body density moving inward from normal-appearing cortex toward cortical lesions highlights the sensitivity of high-gradient diffusion MRI for detecting focal neurodegeneration within the cortex, possibly earlier than detectable cortical thinning. The trends seen between volume loss, lower fsoma and worse cognition emphasize the clinical potential of cortical diffusion measures for identifying people with MS at risk for cognitive decline. Longitudinal studies are needed to understand the temporal relationship between diffusion microstructural alterations in lesional and normal-appearing cortex, regional volume changes, and cognitive impairment. Also, larger studies in people with MS with a greater degree of cognitive impairment are needed to determine the full extent of our findings across the disease spectrum.Conclusion
Normal-appearing cortex in people with MS is characterized by widespread cell body loss that is most pronounced in cortical lesions. The detection of diffusion microstructural alterations in lesional and normal-appearing cortex highlights the potential of high-gradient diffusion MRI to identify focal cortical pathology relevant for cognition in people with MS potentially prior to the onset of cortical volume loss.Acknowledgements
No acknowledgement found.References
1. Harrison DM, Roy S, Oh J, et al. Association of Cortical Lesion Burden on 7-T Magnetic Resonance Imaging With Cognition and Disability in Multiple Sclerosis. JAMA Neurol. 2015;72(9):1004-12.
2. Treaba CA, Herranz E, Barletta VT, et al. The relevance of multiple sclerosis cortical lesions on cortical thinning and their clinical impact as assessed by 7.0-T MRI. J Neurol. 2021;268(7):2473-2481.
3. Krijnen EA, Russo AW, Salim Karam E, et al. Detection of grey matter microstructural substrates of neurodegeneration in multiple sclerosis. Brain Commun. 2023;5(3):fcad153.
4. Bouman PM, Noteboom S, Nobrega Santos FA, et al. Multicenter Evaluation of AI-generated DIR and PSIR for Cortical and Juxtacortical Multiple Sclerosis Lesion Detection. Radiology. 2023;307(2):e221425.
5. Palombo M, Ianus A, Guerreri M, et al. SANDI: A compartment-based model for non-invasive apparent soma and neurite imaging by diffusion MRI. Neuroimage. 2020;215:116835.
6. Bevan RJ, Evans R, Griffiths L, et al. Meningeal inflammation and cortical demyelination in acute multiple sclerosis. Ann Neurol. 2018;84(6):829-842.
7. Herranz E, Louapre C, Treaba CA, et al. Profiles of cortical inflammation in multiple sclerosis by. Mult Scler. 2020;26(12):1497-1509.
Figures