0958
A preliminary investigation for a Localized Quadratic Encoded 3D bSSFP cardiac cine MRI1Department of Radiology, Mayo Clinic, Rochester, MN, United States, 2MR R&D, Philips Healthcare, Rochester, MN, United States
Synopsis
Keywords: Data Acquisition, Heart, 3D cardiac image, 3D cine image, localized quadratic encoding
Motivation: A gated 3D cardiac cine MRI will be useful to evaluate cardiac structure and function from different viewing angles, unlike conventional 2D scans covering only specific orientations.
Goal(s): To develop a retrospectively cardiac gated 3D imaging sequence for the cine scan with reasonable breath-hold time and reconstruction speed.
Approach: A bSSFP sequence was combined with Localized Quadratic Encoding RF pulses for the cardiac gated 3D imaging.
Results: The 3D cardiac cine imaging requires around 20 breath-holds and each breath-hold takes around 25 seconds. The images feature similar soft tissue contrast to the conventional 2D bSSFP scanning with isotropic resolution along different viewing angles.
Impact: The proposed method enables a 3D cardiac cine scan with reasonable breath-hold duration and much faster reconstruction speed.
Introduction:
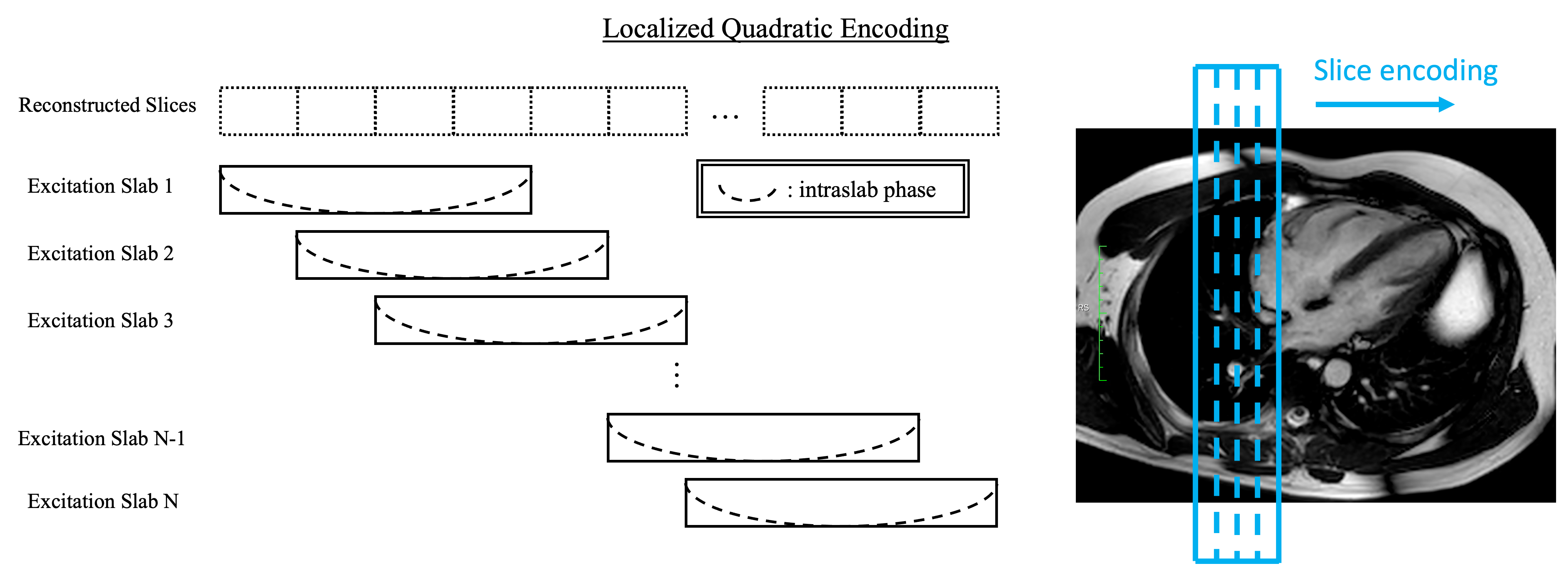
Cardiac cine MRI has been extensively used for evaluating structure and physiological function of the heart1. The most common cine protocol utilizes a two-dimensional(2D) cardiac gated balanced steady state free presession sequence (bSSFP) acquisition over several slices along the cardiac short axis, supplemented with two-, three-, and four-chamber views. As these acquisitions are obtained with 2D scans, it will be difficult to reformat the data retrospectively to depict the information along different viewing angles. On the other hand, a time-resolved 3D acquisition, with a nearly isotropic spatial resolution, offers flexibility for spatial reformatting. But motion gating and breath-holding time have been critical issues. Several methods were proposed incorporating compressed sensing(CS) to solve the problems2-4. While these methods are successful, long reconstruction time up to tens of hours, and the high demand of computational memory have hindered their application in the routine clinical practice. Therefore, an alternative method to allow reasonable acquisition speed and faster image reconstruction will be beneficial for performing a 3D cine acquisition.Localized quadratic encoding(LQE)5,6 is a hybrid 2D and 3D approach utilizing the quadratic phases after the frequency modulated RF excitation to encode the slices among the excited overlapping thin slabs as shown in Fig.1. This excitation scheme enables segmenting a 3D scan along the slice direction to allow the sequence to be compatible with multiple breath-holds to compensate respiratory motion. Here, we propose a combination of LQE and bSSFP sequence to provide a breath-hold retrospectively gated 3D cardiac cine imaging.
Methods:
Volunteer studies were performed with an IRB approved protocol on a 1.5T magnet (Ambition X, Philips Healthcare) after informed consent. A conventional bSSFP sequence was modified by substituting the sinc RF pulse with an LQE RF pulse. The sequence incorporated breath-holding instructions and retrospectively cardiac gating for the cine imaging. The scan slab orientation was sagittal, with frequency encoding in the craniocaudal direction and phase encoding in the anterior-posterior direction. Other imaging parameters were TE/TR=1.6/3.2ms, flip angle=450, views per segment=14, in-plane resolution=$$$1.7\times1.9mm^2$$$ , slice thickness = 1.8mm, excitation slab thickness=10.8mm with a total of 82 slabs to cover the whole heart, and SENSE factor=2 using a 25-channel body coil. Each slice of the image required eight heart beats to finish, and four slices were scanned within a breath-hold leading to a total of 21 breath-holds to finish scanning the entire heart.Coil compression was firstly performed on the raw data using singular-value-decomposition to transform the data to 10 synthetic coils7. The compressed data are gridded to 24 cardiac phases in this study before spatial processing. The localized quadratic phases of the slabs are then removed to restore the slice resolution. The parallel imaging reconstruction follows to remove aliasing artifacts. The reconstructed data can be reformatted to the requested orientations for display. Along each displayed orientation, a moving average kernel of 3 slices is applied for SNR improvement.
Results:
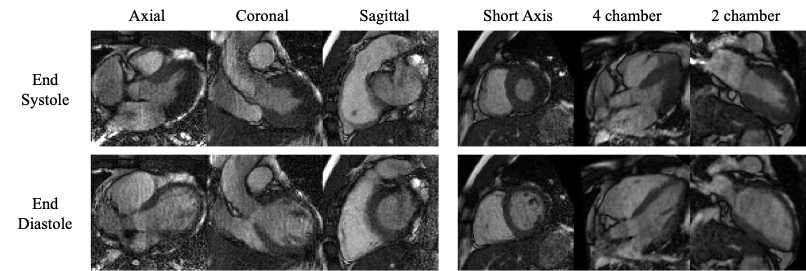
Fig.2. demonstrates the reformatted slices at both end systole and end diastole. Contrasts between the blood pool and the myocardium are similar to the conventional 2D scans. Fig.3. shows the time series along the reformatted orientations, demonstrating the proposed method’s capability to provide high spatial-temporal resolution and good SNR in the image. Mild inhomogeneous banding appears in both axial and coronal planes along right-left direction. These artifacts are mainly from the transient state of flow signals in each composite thin slab. However, they do not impede evaluation of important structural information. Along the short-axis, four-chamber, and two-chamber views, the flow artifacts are less prominent due to interpolation during spatial reorientation. As for the offline-reconstruction time, it took roughly one minute to perform slice reconstruction and 8.5 minutes for parallel imaging reconstruction of the whole volumetric time series (82-slices and 24 cardiac phases) using Python on a 6-core 2.9GHz Intel CPU.Discussion:
The proposed method divides a 3D scan into several thin slabs before recombination to allow using conventional breath-holding techniques, with the capability to tailor breath-holding duration to a patient’s individual capabilities. Its compatibility with the bSSFP sequence retains similar soft tissue contrasts to the conventional 2D cardiac cine protocols. A major advantage of this work is the shorter computation time, as it only involves decoding LQE and conventional parallel imaging. The proposed sequence can be an alternative for the 3D cardiac CINE imaging. However, one issue of the sequence is flow artifacts around the boundaries of the slabs. So far, the artifacts do not impose any problem veiling the tissue and will be investigated to mitigate its influence in the future.Acknowledgements
This work is suppored in part by Philips.References
1. Schulz-Menger J, et al. Standardized image interpretation and post-processing in cardiovascular magnetic resonance - 2020 update : Society for Cardiovascular Magnetic Resonance (SCMR): Board of Trustees Task Force on Standardized Post-Processing. J Cardiovasc Magn Reson. Mar 12 2020;22(1):19. doi:10.1186/s12968-020-00610-6
2. Feng L, et al. 5D whole-heart sparse MRI. Magn Reson Med. Feb 2018;79(2):826-838. doi:10.1002/mrm.26745
3. Usman M, Ruijsink B, Nazir MS, Cruz G, Prieto C. Free breathing whole-heart 3D CINE MRI with self-gated Cartesian trajectory. Magn Reson Imaging. May 2017;38:129-137. doi:10.1016/j.mri.2016.12.021
4. Jeong D, Schiebler ML, Lai P, Wang K, Vigen KK, Francois CJ. Single breath hold 3D cardiac cine MRI using kat-ARC: preliminary results at 1.5T. Int J Cardiovasc Imaging. Apr 2015;31(4):851-7. doi:10.1007/s10554-015-0615-0
5. Pipe JG. Spatial encoding and reconstruction in MRI with quadratic phase profiles. Magn Reson Med. Jan 1995;33(1):24-33. doi:10.1002/mrm.1910330105
6. Pipe JG. Analysis of localized quadratic encoding and reconstruction. Magn Reson Med. Jul 1996;36(1):137-46. doi:10.1002/mrm.1910360122
7. Zhang T, Pauly JM, Vasanawala SS, Lustig M. Coil compression for accelerated imaging with Cartesian sampling. Magn Reson Med. Feb 2013;69(2):571-82. doi:10.1002/mrm.24267
Figures