0956
Self-gated 2D lung imaging using single petal rosette trajectory1Department of Internal Medicine II, Ulm University Medical Center, Ulm, Germany
Synopsis
Keywords: Data Acquisition, New Trajectories & Spatial Encoding Methods
Motivation: Major limitation of lung MRI is respiratory motion which can be overcome by retrospective self-gating approaches.
Goal(s): Achieving sufficient SNR values in the parenchyma is crucial for clinical evaluations and the assessment of physiological parameters.
Approach: This abstract presents a single-petal rosette UTE trajectory that is evaluated for k-space-, as well as image-based, retrospective self-gated lung imaging in comparison to the radial UTE trajectory.
Results: Higher SNR values and sharpness are obtained when using the SPR trajectory, compared to radial UTE sampling approaches at constant temporal resolution.
Impact: This abstract presents a single-petal rosette UTE trajectory (SPR) for 2D self-gated lung imaging, yielding higher SNR and sharpness in comparison to radial UTE sampling approaches.
Purpose
Ultrashort T2* relaxation times, found e.g. in lung tissue1 require MR imaging approaches with short echo times (TE). Ultrashort echo time (UTE) sequences enable data acquisition with minimization of TE by acquisition of the data during ramping of the read-out gradient as opposed to only sampling when the gradient plateau is reached.To eliminate respiratory motion, retrospective gating techniques are frequently applied to lung imaging, overcoming the highly limited maximum scan duration for a breath-hold acquisition of a few seconds. In this contribution, we applied a single petal rosette trajectory (SPR), which more efficiently covers k-space by additional data sampling during the required rephrasing of a UTE acquisition. The performance of the suggested trajectory and variants thereof for self-gated free-breathing acquisitions is investigated in volunteers and compared to radial UTE imaging.
Methods
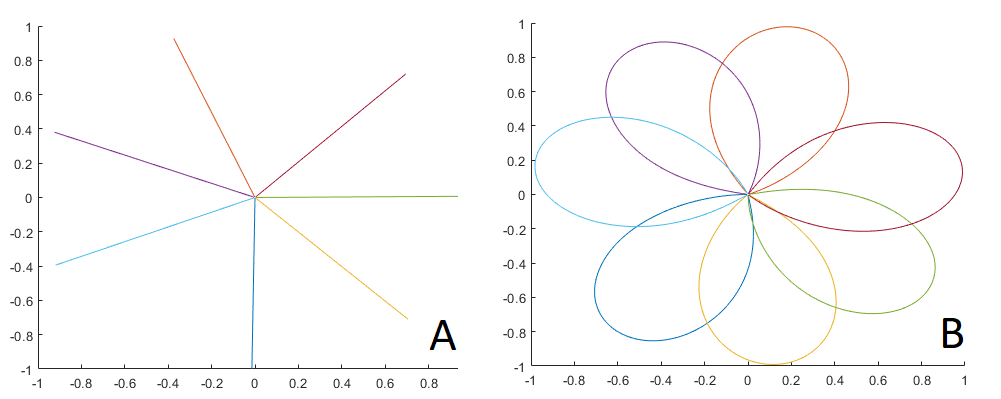
The suggested approach was tested in 5 healthy volunteers with no reported respiratory disorders, who provided informed written consent prior to the MR examination. Images were acquired during a single breath-hold, each for inspiration and expiration, as well as during a free breathing scan of 2-3 minutes at a 3 T whole-body clinical imaging system (Ingenia 3.0T CX, Philips Healthcare, Best, The Netherlands) using a 32 (16 anterior, 16 posterior) torso coil (dStream Torso, Philips Healthcare). All data were acquired in coronal slice orientation centred at the bifurcation of the trachea.The SPR trajectory2 is parametrized by
$$k(t) = k_{\text{max}} \sin(\omega t) \text{e}^{it} ,$$
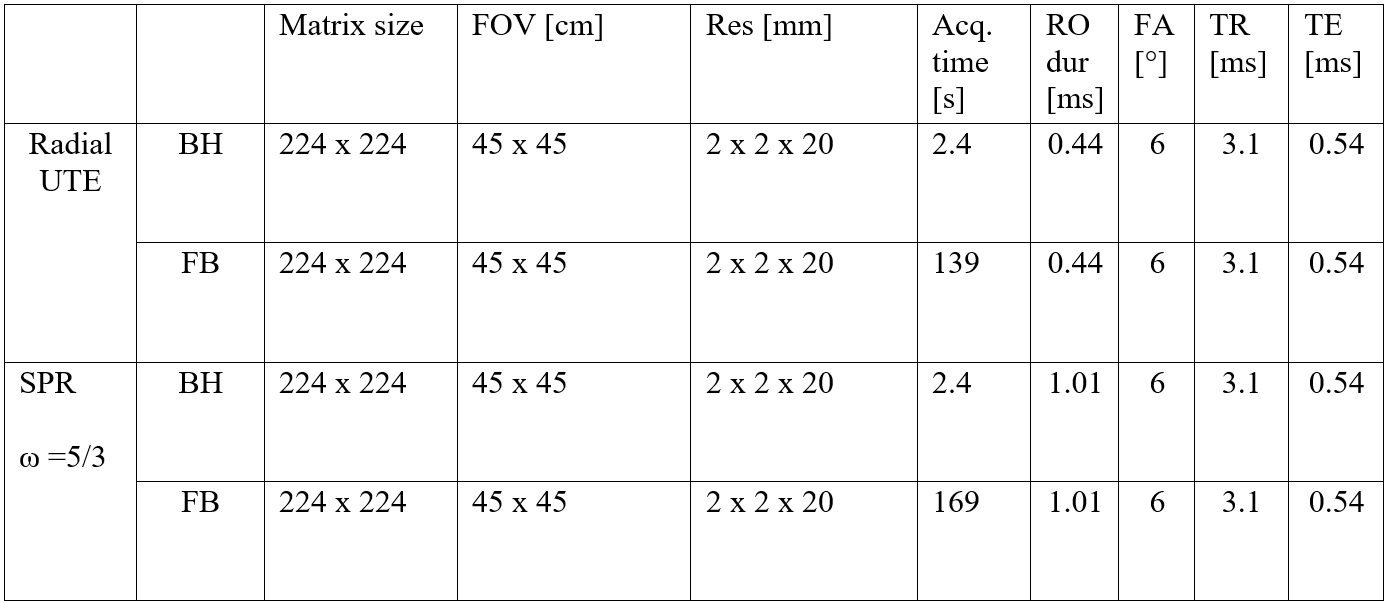
with k being the position in k-space, kmax the outmost position of sampling k-space and $$$\omega$$$ the angular frequency, which was chosen as 5/3. The radial UTE acquisition followed the radial UTE center-out sampling pattern3. In both approaches, an angular increment following the tiny golden angle sampling scheme ($$$\varphi_7$$$ = 23.6281°)4 was used. The number of readouts for both approaches was determined to Nyquist sample k-space for the radial UTE sequence. All relevant scan parameters are listed in table 1.
For image reconstruction, an in-house built reconstruction framework, implemented in MATLAB (The MathWorks, Natick, Massachusetts, USA) was used. The k-space density functions for the SPR trajectory were calculated using a Voronoi tessellation5. The gating was performed using a k0-based self-gating approach (SGksp) (SG signal derived from temporal evolution of DC-signal, subsequently bandpass filtered and combined with principal component analysis to get the respiratory navigator signal), as well as two image-based approaches (SGimg) (navigator signal derived from high-temporal resolution images by gradient analysis of the lung-liver interface (LLI), respiratory stages were determined by a histogram-based approach (SGimg,hist), as well as an absolute value-based approach (SGimg,abs)). The self-gating reconstructions are described in further detail in Metze et al.6 A temporal resolution of 100 ms was chosen for all self-gated reconstructions.
The parenchyma was segmented semi-automatically and SNR was calculated according to
$$\text{SNR} = \sqrt{2-\frac{\pi}{2} } \frac{\text{SI}_{\text{ROI}}}{\omega_{\text{BG}}},$$
with SIROI being the signal intensity of a region of interest (ROI) and $$$\omega_{\text{BG}}$$$ the standard deviation of background noise. Additionally, image sharpness was assessed by a standard metric7, identifying the positions of pixels corresponding to 25 and 75% of the maximum signal intensity of an intensity profile, chosen across the LLI.
Results
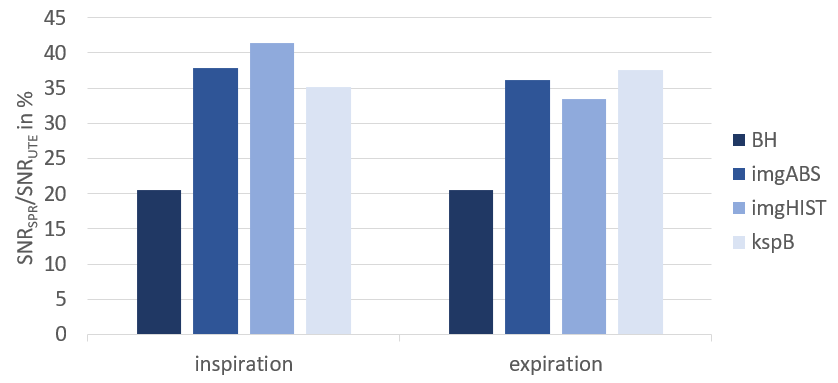
Data acquisition could be completed for all volunteers.SNR improved by 20% for breath-hold acquisitions when comparing SPR and radial UTE images. For the self-gated reconstructions, the SNR in the lung parenchyma increased between 33% and 41% as can be appreciated in figure 2.
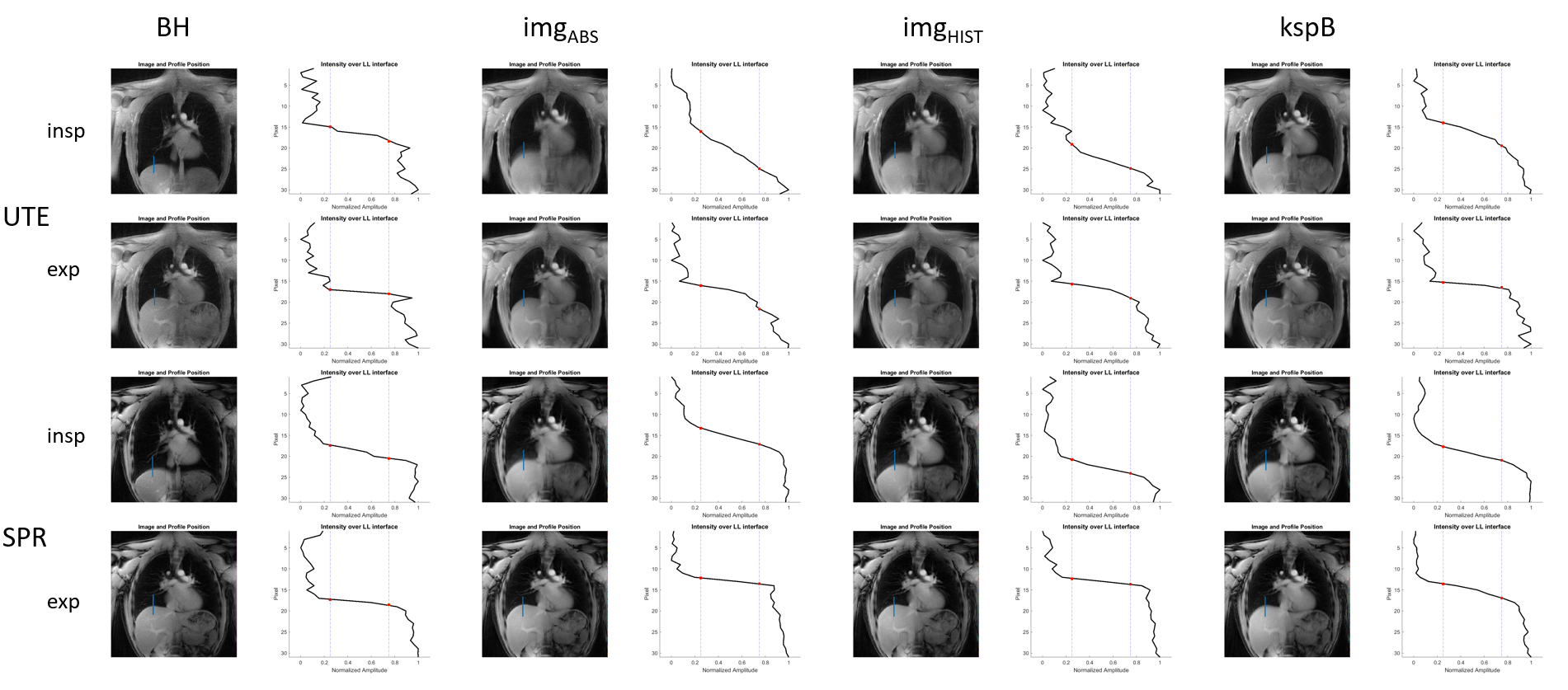
Figure 3 shows the line profile placed over the LLI for breath-hold and self-gated images of one volunteer for both radial UTE and SPR trajectory, for inspiration and expiration, respectively.
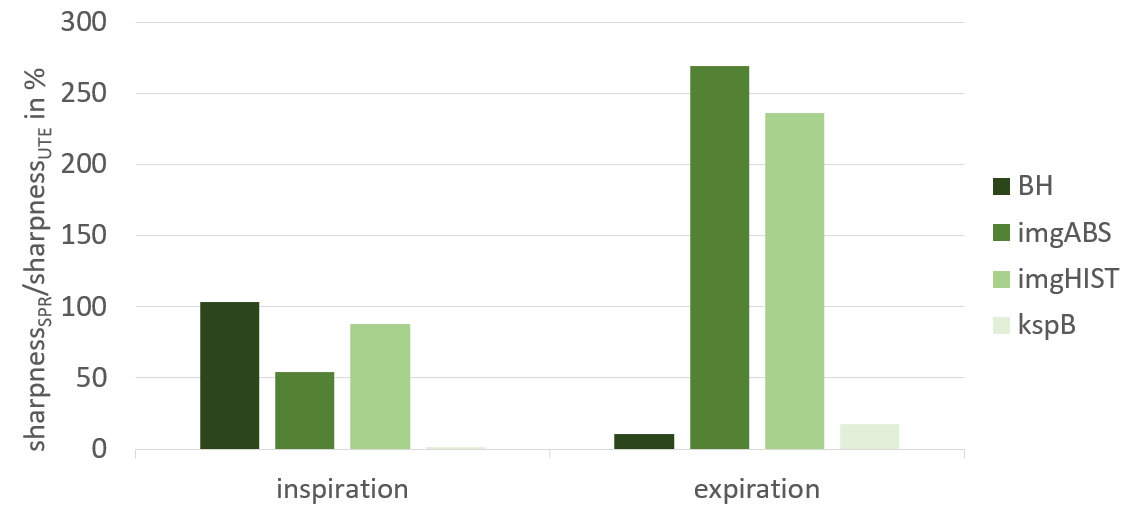
While sharpness for images reconstructed using SGksp only differs by less than 20%, the image based self-gating approaches increase sharpness by up to 270% for the expiratory phase, as can be seen in figure 4.
Discussion and Conclusion
The SPR trajectories cover more k-space data without increasing repetition time or total scan duration, since each petal ends in k0, thus removing the necessity of a rephasing gradient applied prior to spoiling. The resulting oversampling of k-space yields improved SNR compared to radial UTE sampling.The higher sampling density of k-space per interleave decreases aliasing artifacts in the high-temporal resolution images, thus increasing performance of especially image-based self-gating approaches, which can be appreciated in the sharpness analysis.
Considering the previously outlined compatibility of the SPR trajectory with image-based self-gating approaches, suitability of the SPR trajectory with the nuSG algorithm7 suggests itself to be further evaluated. Additionally, an implementation for 3D imaging within the framework of stack-of-stars might be worth pursuing.
Acknowledgements
The authors
thank the Ulm University Center for Translational Imaging MoMAN for its support.
This work was supported by the German Research Foundation funding agreement
465599659. Technical support from Philips Healthcare is gratefully
acknowledged.
References
- Wild JM, Marshall H, Bock M, et al. MRI of the lung (1/3): methods. Insights Imaging. 2012;3(4):345-53.
- Noll DC. Multishot Rosette Trajectories for Spectrally Selective MR Imaging. IEEE. 1997;16(4): 0278–0062.
- Bergin CJ, Pauly JM, Macovski A. Lung parenchyma: projection reconstruction MR imaging. Radiology 1991;179(3):777–781.
- Wundrak S, Paul J, Ulrici J, et al. Golden ratio sparse MRI using tiny golden angles. Magn Reson Med 2016; 75:2372-2378.
- Rasche V, Proksa R, Sinkus R, et al. Resampling of data between arbitrary grids using convolution interpolation. IEEE Trans Med Imaging. 1999;18(5):385-92.
- Metze P, Frantz H, Straubmüller F, et al. Non-Uniform Self-Gating in 2D Lung Imaging. Front. Phys. 2022;10:836178.
- Wundrak S, Paul J, Ulrici J, et al. A Self-Gating Method for Time-Resolved Imaging of Nonuniform Motion. Magn Reson Med. 2016;76:919–25.
Figures