0955
Vendor-Neutral Development and Cross-Center Validation of Flip Angle Modulated 2D Sequential CSE-MRI Technique for Liver Fat Quantification1Medical Physics, University of Wisconsin-Madison, Madison, WI, United States, 2Radiology, University of Wisconsin-Madison, Madison, WI, United States, 3Key Laboratory for Biomedical Engineering of Ministry of Education, Department of Biomedical Engineering, College of Biomedical Engineering & Instrument Science, Zhejiang University, Hangzhou, China, 4Athinoula A. Martinos Center for Biomedical Imaging, Massachusetts General Hospital, Charlestown, MA, United States, 5State Key Laboratory of Extreme Photonics and Instrumentation, College of Optical Science and Engineering, Zhejiang University, Hangzhou, China, 6Radiology, Harvard Medical School, Boston, MA, United States, 7Calimetrix, LLC, Madison, WI, United States, 8Biomedical Engineering, University of Wisconsin-Madison, Madison, WI, United States, 9Data Science Institute, University of Wisconsin-Madison, Madison, WI, United States, 10Electrical and Computer Engineering, University of Wisconsin-Madison, Madison, WI, United States, 11Radiology, University of Michigan, Ann Arbor, MI, United States, 12Division of Medical Physics, Department of Radiology, University Medical Center Freiburg, Faculty of Medicine, University of Freiburg, Freiburg, Germany, 13Medicine, University of Wisconsin-Madison, Madison, WI, United States, 14Emergency Medicine, University of Wisconsin-Madison, Madison, WI, United States
Synopsis
Keywords: Pulse Sequence Design, Fat, fat/water separation, data acquisition, liver, pulse sequence design, software tools
Motivation: 2D sequential chemical-shift-encoded acquisitions with centric encoding and flip-angle modulation (FAM) enables motion-robust and high-SNR liver fat quantification. Originally developed in a single vendor, the performance and relative simplicity of FAM motivate vendor-neutral implementation and validation.
Goal(s): Implement FAM in the vendor-neutral framework Pulseq, and determine its feasibility, bias, and reproducibility in a multi-center, multi-vendor study.
Approach: Pulseq-FAM was applied in two centers with two vendors on a phantom with controlled PDFF/T1water values, and in volunteers during free breathing.
Results: At both centers, Pulseq-FAM shows low bias and good reproducibility in the phantom, and excellent motion robustness and image quality in volunteers.
Impact: A vendor-neutral implementation of motion-robust liver fat quantification, as demonstrated in this study, may enable detection, staging, and treatment monitoring of steatotic liver disease with improved availability and standardization.
Background
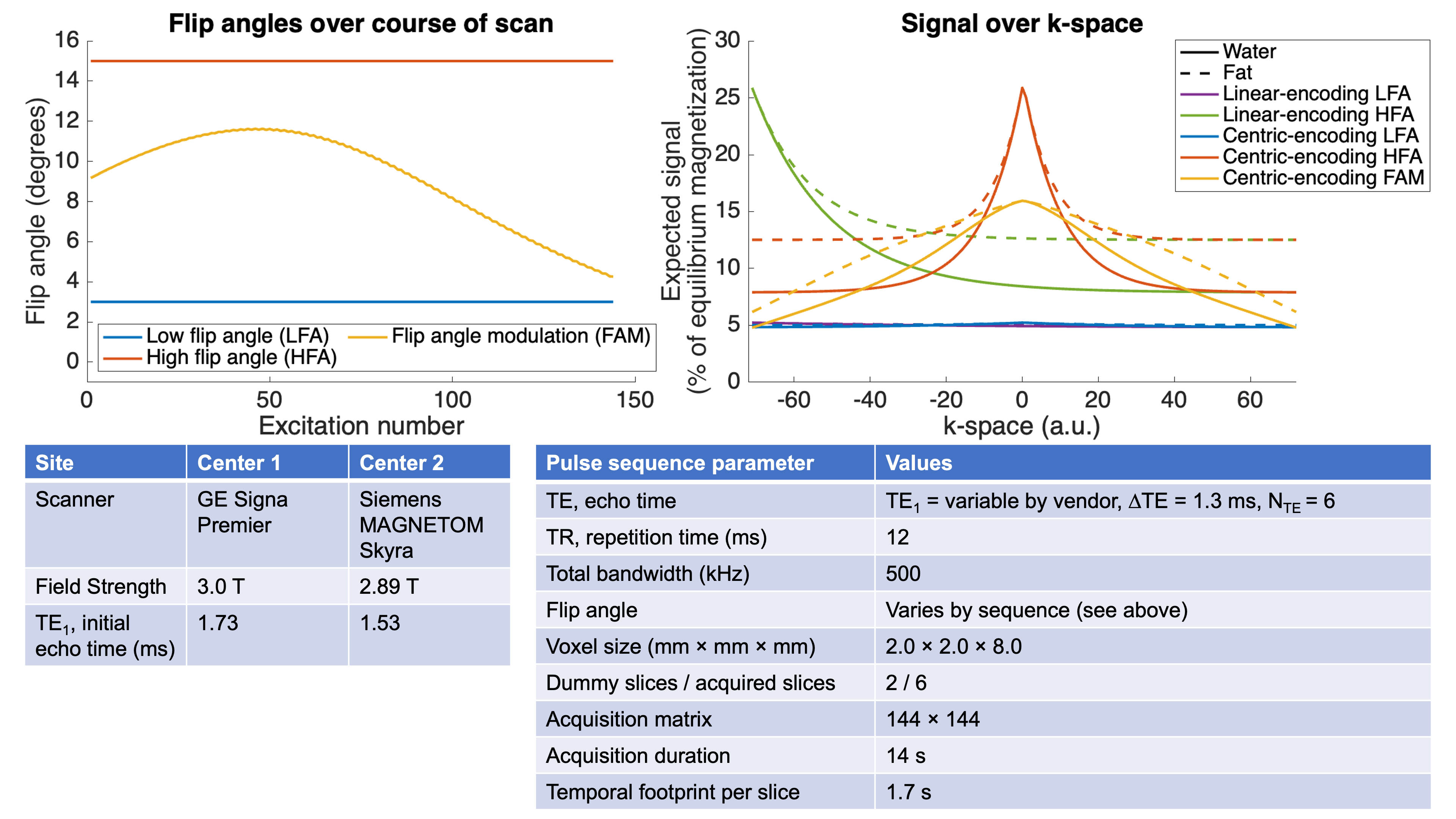
The increasing prevalence of steatotic liver disease necessitates the widespread implementation of non-invasive techniques for quantifying liver fat. Although breath-held methods for mapping of proton-density fat fraction (PDFF) have been implemented by all major vendors1, a free-breathing method is desirable for error-proof PDFF mapping that works for all patient populations. 2D sequential chemical-shift-encoded MRI with centric encoding and flip-angle modulation (FAM)2 is well-positioned to meet this need. FAM achieves an optimized combination of high SNR, low bias, and minimal blurring due to amplitude modulation in k-space (Figure 1), with good motion robustness due to its short temporal footprint. However, FAM was originally developed for a single vendor, which limits its widespread dissemination and standardization. Therefore, the purpose of this work is to develop and evaluate FAM in the vendor-neutral framework Pulseq3,4 to broaden access across populations and institutions and improve standardization.Methods
Pulse SequencesTo compare flip angle (FA) and encoding methods in terms of T1-bias, SNR, and imaging artifacts, we implemented five versions of a 2D sequential multi-echo spoiled gradient echo sequence in Pulseq: our proposed centric-encoding FAM method, and four conventional methods with constant FAs (centric/linear encoding and 3/15 degree FAs; see Figure 1). The 2D sequential acquisition promotes motion-robustness due to the 1.7s temporal footprint of each slice. In Pulseq-FAM, FAs were optimized and modulated over the course of the phase encoding TRs, by minimizing a previously published cost function2.
Acquisitions & Analysis
These acquisitions were performed on two different vendors’ systems (GE Signa Premier 3.0T, Waukesha, WI, and Siemens MAGNETOM Skyra 2.89T, Erlangen, Germany) at two different centers, where the same phantom was scanned. This commercial PDFF-T1 phantom (Calimetrix LLC, Madison, WI) included gel-based vials with known PDFF values (0,10,20,30%) and T1water (200,600,1000,1400ms), to cover a wide, clinically-relevant range of values with and without contrast.
The phantom was positioned with vials along the bore of each scanner and scanned with multi-channel head coils. Ten acquisitions were performed with each sequence without repositioning to evaluate voxel-wise standard deviations (SDs) as a surrogate for SNR. PDFF maps were calculated for each acquisition using a confounder-corrected reconstruction algorithm5. Cylindrical ROIs were drawn on each vial of the phantom in two slices corresponding to the center of each vial, and the means of voxel-wise SDs within each ROI were recorded. Bias was also measured by calculating the difference in ROI means between a Pulseq sequence and a commercially-available PDFF mapping sequence (IDEAL-IQ, GE HealthCare). In addition, Bland-Altman analysis was used to evaluate cross-center reproducibility.
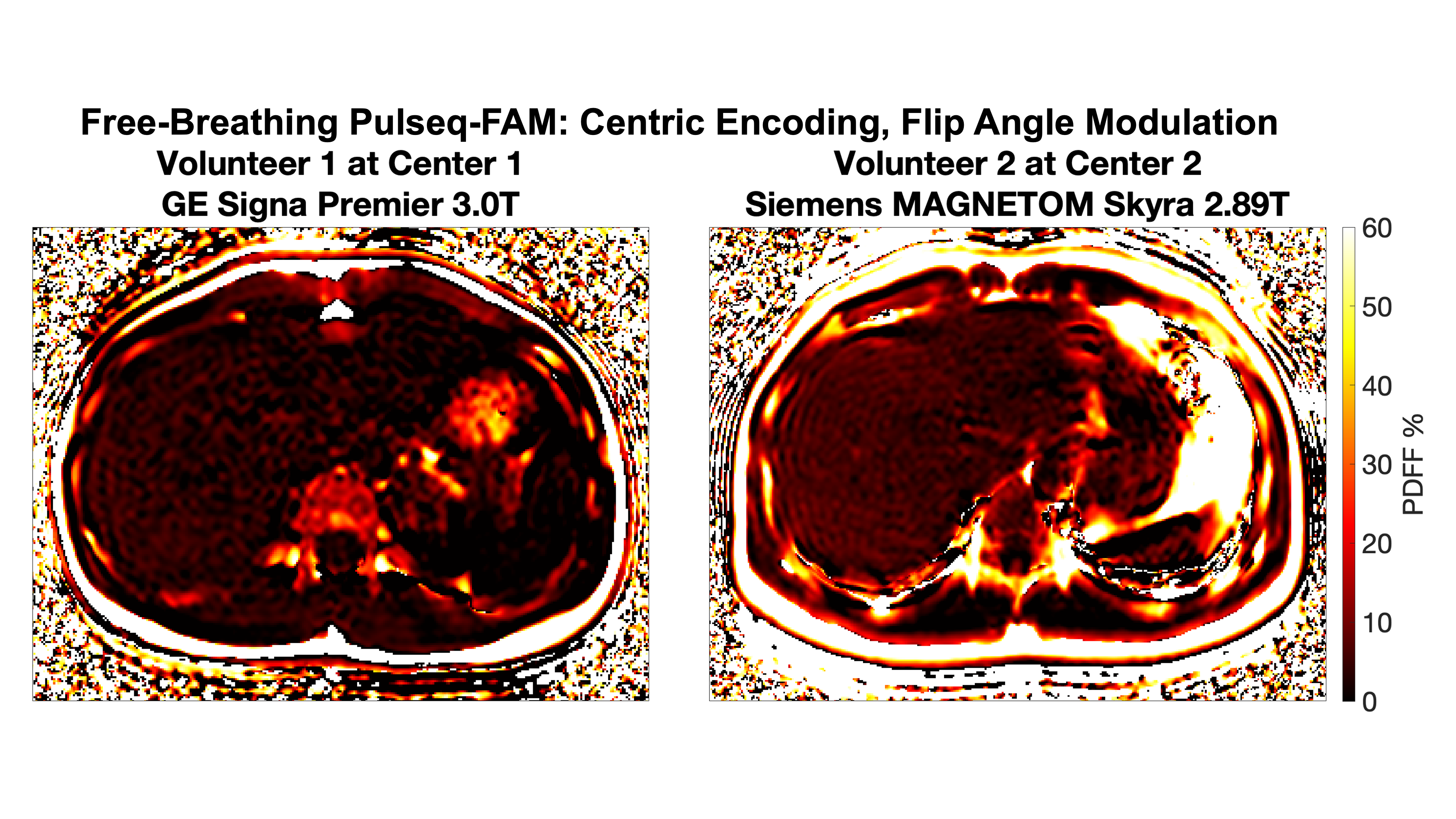
Finally, each site imaged a different healthy volunteer during free-breathing to evaluate in-vivo feasibility and respiratory-motion robustness.
Results
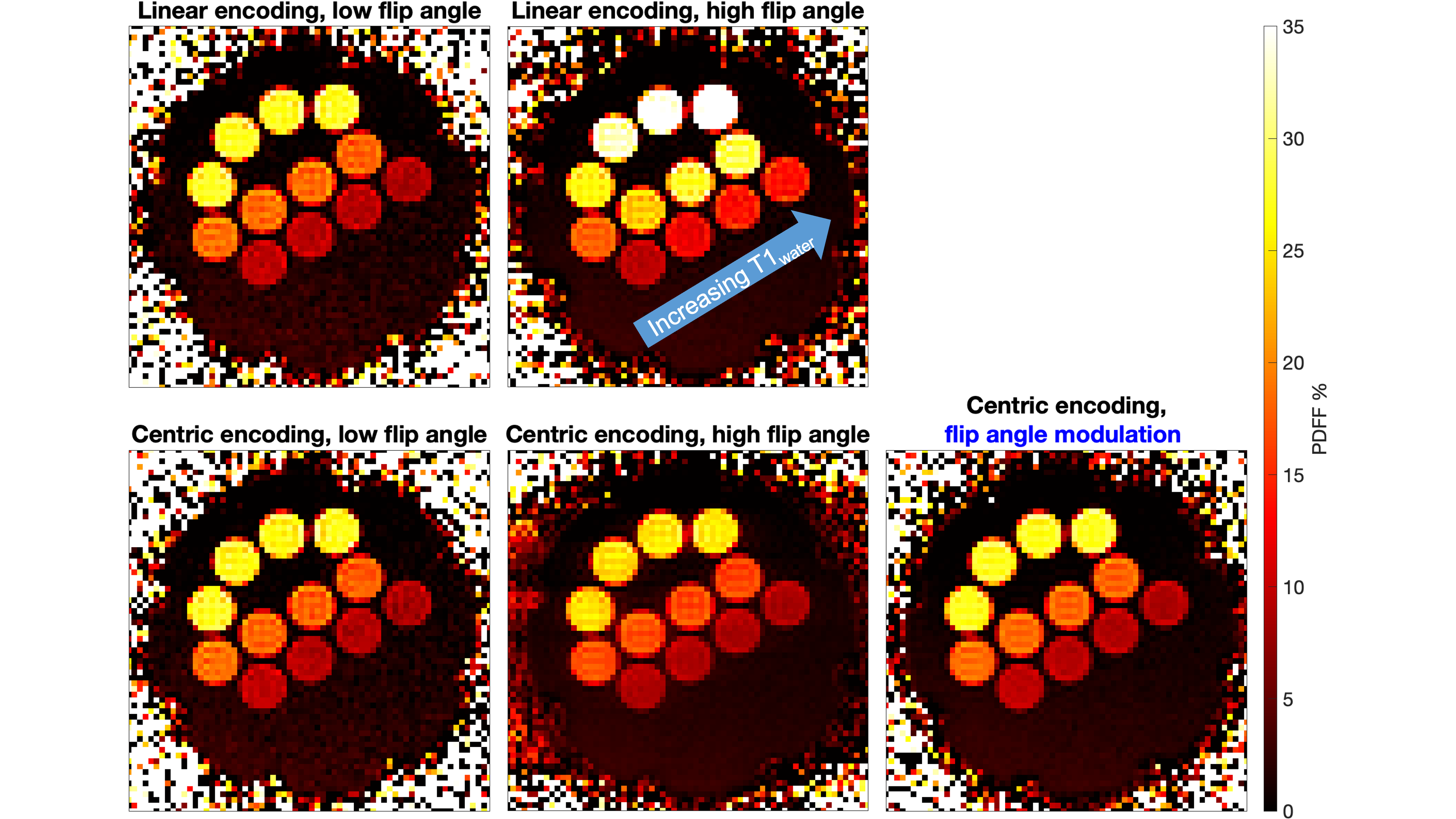
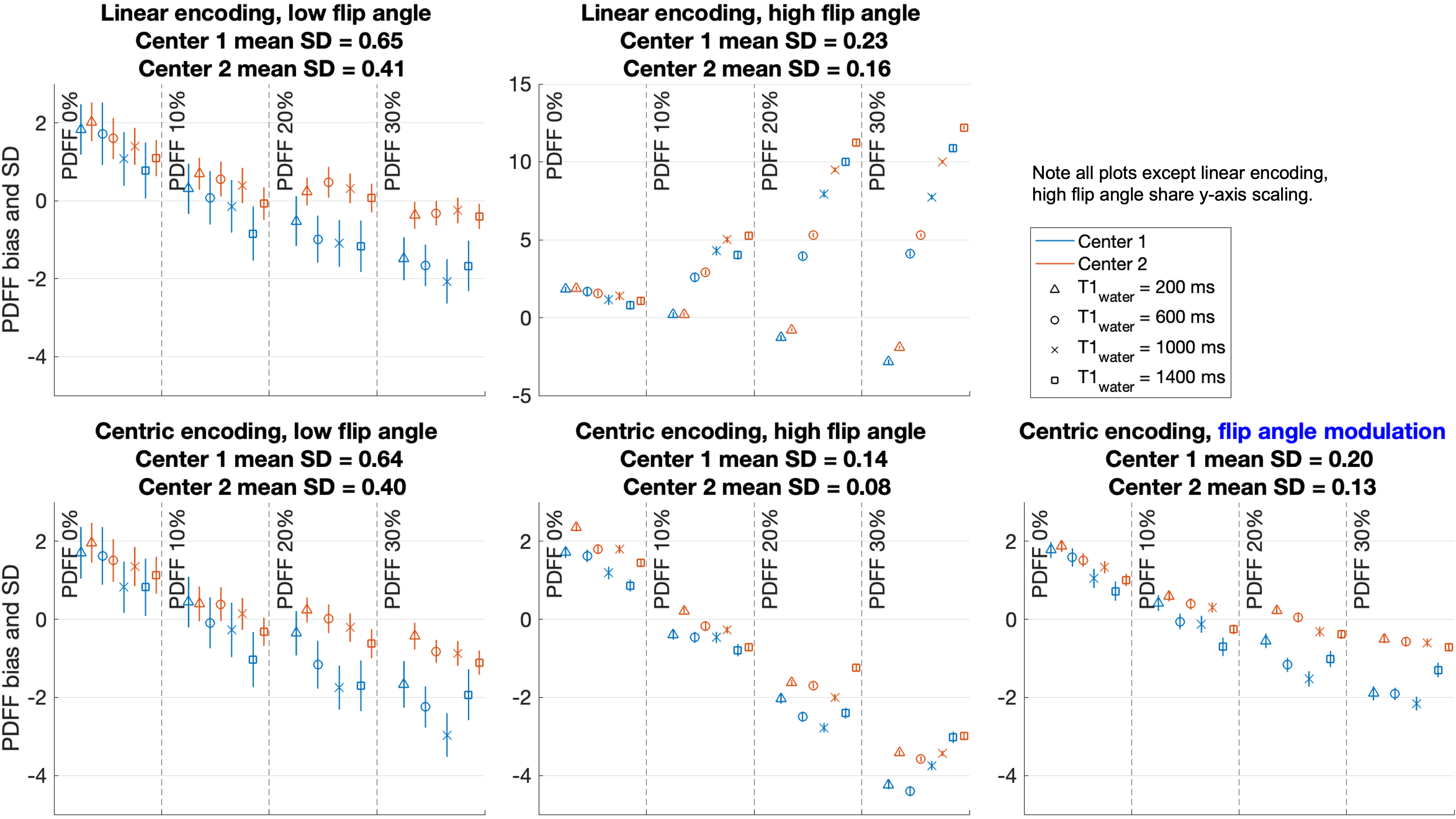
Images from phantom acquisitions are shown in Figure 2. As predicted by k-space profiles (Figure 1), low flip angle (LFA) methods and FAM demonstrate low T1-bias in the PDFF-T1 phantom (Figure 3). High flip angle (HFA) acquisitions demonstrate substantial bias due to heavy T1 weighting (linear-encoding HFA) or image blurring (centric-encoding HFA).LFA methods have the highest voxel-wise SDs (worst SNR) in PDFF maps due to their lower signal near the center of k-space. The centric-encoded HFA acquisition has the lowest voxel-wise SDs; however, it leads to substantial blurring and bias, as described above.
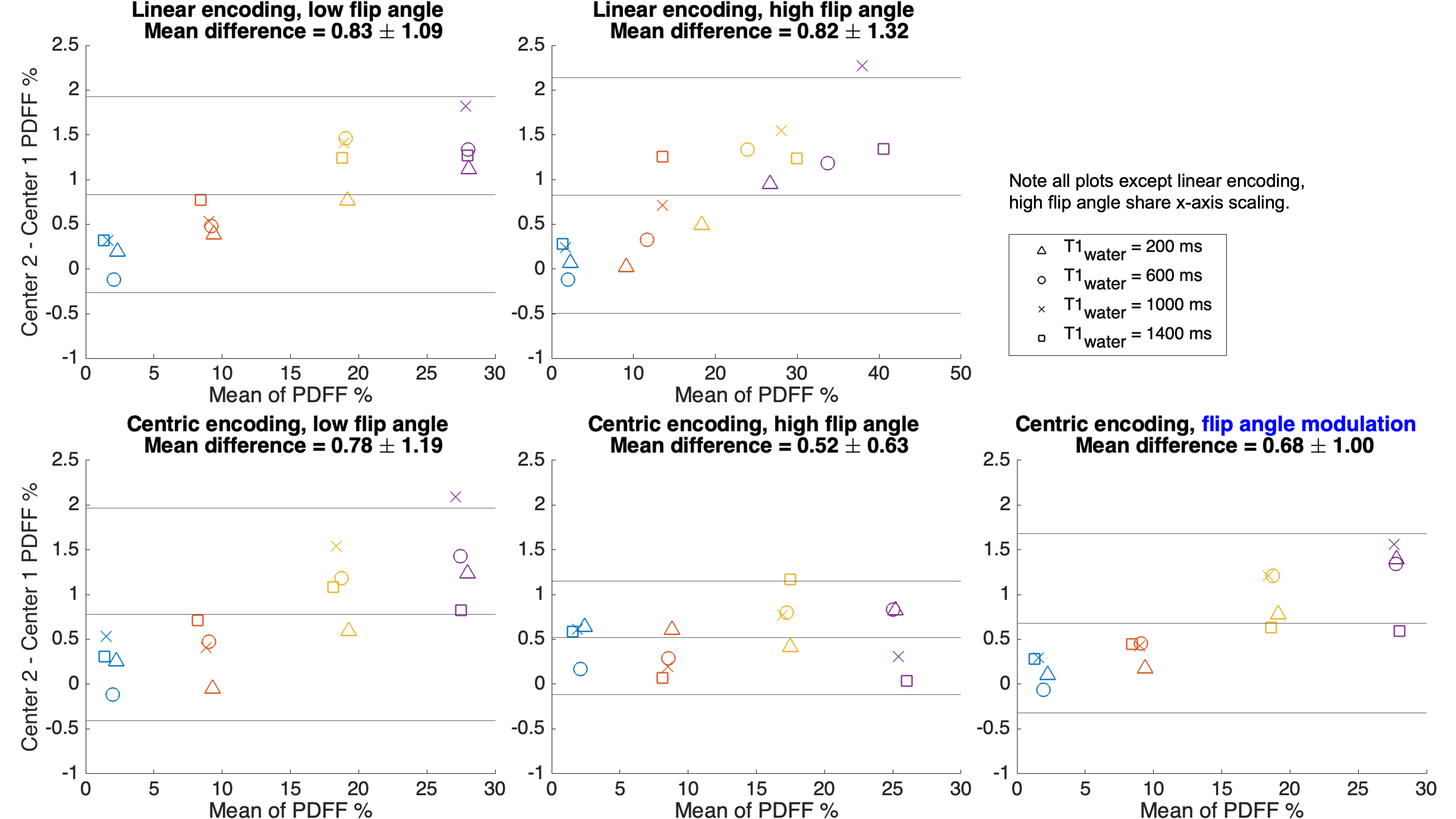
Methods with lower SDs also showed better cross-center reproducibility (Figure 4). FAM shows relatively low SDs and good reproducibility, approaching the SNR of centric-encoded HFA, without the associated bias and blurring.
In vivo data (Figure 5) further demonstrate the good image quality and motion robustness of FAM. Liver imaging results were consistent with phantom data in terms of the image quality, SNR, and lack of T1-bias of FAM relative to the alternative FA schemes and encoding methods (not shown).
Discussion
We successfully developed a vendor-neutral (Pulseq) implementation of a motion-robust PDFF mapping method based on a 2D sequential acquisition with centric encoding and flip-angle modulation (FAM). In a cross-center, two-vendor study, Pulseq-FAM demonstrated low bias and strong reproducibility in phantoms, and excellent image quality and motion robustness in vivo.Importantly, implementation of FAM was straightforward in Pulseq. The differences between the five sequences used above were implemented by simply changing two variables for flip angles and phase encode ordering. The success of Pulseq-FAM suggests possible future work in using parallel imaging acceleration to further shorten its temporal footprint, evaluation across more centers and field strengths, and fine-tuning for system-specific timings to improve harmonization of TEs.
Altogether, this work has demonstrated vendor-neutral, reproducible, motion-robust PDFF mapping, which may enable detection, staging, and monitoring of steatotic liver disease with improved availability and standardization.
Acknowledgements
The authors acknowledge support from NIH grants R44EB025729 and R01EB031886.The authors also gratefully acknowledge David Harris and the University of Wisconsin Department of Radiology support staff for logistical assistance.
Dr. Hernando and Dr. Reeder are co-founders of Calimetrix, LLC, which manufactured and loaned to the authors the phantom used in this study.
Dr. Reeder is the John H. Juhl Endowed Chair of Radiology.
Jiayi Tang is a shareholder of GE HealthCare.
GE HealthCare provides research support to the University of Wisconsin.
References
- Yokoo T, Serai SD, Pirasteh A, et al. Linearity, Bias, and Precision of Hepatic Proton Density Fat Fraction Measurements by Using MR Imaging: A Meta-Analysis. Radiology. 2018;286(2):486-498. doi:10.1148/radiol.2017170550
- Zhao R, Zhang Y, Wang X, et al. Motion-robust, high-SNR liver fat quantification using a 2D sequential acquisition with a variable flip angle approach. Magn Reson Med. 2020;84(4):2004-2017. doi:10.1002/mrm.28263
- Layton KJ, Kroboth S, Jia F, et al. Pulseq: A rapid and hardware-independent pulse sequence prototyping framework. Magn Reson Med. 2017;77(4):1544-1552. doi:10.1002/mrm.26235
- Nielsen JF, Noll DC. TOPPE: A framework for rapid prototyping of MR pulse sequences. Magn Reson Med. 2018;79(6):3128-3134. doi:10.1002/mrm.26990
- Hernando D, Hines CDG, Yu H, Reeder SB. Addressing phase errors in fat-water imaging using a mixed magnitude/complex fitting method. Magn Reson Med. 2012;67(3):638-644. doi:10.1002/mrm.23044
Figures