0945
Wideband joint black- and bright-blood late gadolinium enhancement imaging in patients with cardiac implantable devices1Department of Diagnostic and Interventional Radiology, Lausanne University Hospital and University of Lausanne, Lausanne, Switzerland, 2IHU LIRYC, Electrophysiology and Heart Modeling Institute, Université de Bordeaux – INSERM U1045, Bordeaux, France, 3Department of Cardiovascular Imaging, Hôpital Cardiologique du Haut-Lévêque, CHU de Bordeaux, Bordeaux, France, 4Department of Cardiac Pacing and Electrophysiology, Hôpital Cardiologique du Haut-Lévêque, CHU de Bordeaux, Bordeaux, France, 5CIBM, Center for Biomedical Imaging, Lausanne, Switzerland
Synopsis
Keywords: Pulse Sequence Design, Tissue Characterization
Motivation: Wideband bright-blood late gadolinium enhancement (LGE) enables artifact-free imaging of myocardial scars in patients with implantable cardioverter defibrillators (ICDs). Unfortunately, the poor scar-blood contrast makes it difficult to depict subendocardial scars.
Goal(s): To improve myocardial scar visualization and localization in ICD patients.
Approach: We propose a 2D breath-hold single-shot ECG-triggered gradient echo wideband joint black- and bright-blood (wideband SPOT) LGE sequence to improve scar visualization and localization, while limiting ICD-artifacts. Wideband was implemented in an adiabatic inversion pulse and in an adiabatic T2 preparation.
Results: Wideband SPOT successfully suppressed ICD-artifacts while improving scar detection, and provided same image quality than reference wideband bright-blood.
Impact: This new technology will enable radiologists and cardiologists to detect and localize myocardial scars more accurately in ICD patients by eliminating ICD hyperintensity artifacts and enhancing scar tissue with unprecedented contrast.
INTRODUCTION
Characterization of myocardial scars in ICD patients can be provided by wideband phase-sensitive inversion recovery (PSIR) LGE1 imaging, capable of reducing hyperintensity ICD-artifacts. However, the poor scar-blood contrast makes it challenging to depict subendocardial scars. Here we propose a joint black- (BL) and bright-blood (BR) wideband LGE technique to improve myocardial scar visualization and localization while limiting ICD-artifacts.METHODS
Sequence: A 2D breath-hold single-shot ECG-triggered gradient echo readout joint wideband BL and BR (wideband SPOT) LGE2 sequence was implemented on a 1.5T system (MAGNETOM Aera, Siemens) (Figure 1A). In odd heartbeats, BL images were acquired using a non-selective adiabatic hyperbolic secant 180° inversion recovery (IR) pulse (duration=10.24ms) followed by an adiabatic T2 preparation3 (T2prep) (TE duration=27ms). In even heartbeats, BR images were acquired using a T2prep. Co-registered BL and BR images were acquired five times per slice position during mid-diastole and then averaged.To eliminate ICD-artifacts1, the IR bandwidth was increased from 0.8 to 9.2kHz (Figure 1B) with a peak B1 amplitude of 30mT, and the T2prep refocusing bandwidth from 1.6 to 5.0kHz with a peak B1 amplitude of 30mT.
Sequence parameters were: 1.4x1.4mm2 in-plane resolution, 8mm slice thickness, FA=15°, GRAPPA x2, TE/TR=2.08/4.8ms, readout bandwidth=751 Hz/pixel, FOV=300mm x 225mm. The inversion time (TI) was determined from a prior standard TI scout.
Animal Experiments: Reference standard and wideband PSIR, as well as standard and wideband SPOT LGE images were acquired in a female sheep (Charmoise, 2 years old) with ischemic scars in the left ventricle. These images were acquired in a randomized order both with and without the presence of an ICD, 15min after the administration of 0.2mmol/kg gadoterate meglumine. The ICD was taped near the left shoulder, 10cm away from the heart. Breath-holds were performed via a respirator. After MRI, the sheep was euthanized to perform histology and confirm scar presence and localization with respect to MR images without ICD.
Patient Experiments: 5 male subjects (63 ± 9 years old) with known myocardial scars and MRI-conditional ICD underwent CMR with reference standard PSIR, and wideband SPOT 15min after injection of 0.2mmol/kg gadoterate meglumine, in random order.
An expert radiologist scored the subjective image quality (1-non-diagnostic, 2-less than adequate, 3-adequate, 4-excellent) and the overall ICD-artefact severity (1-severe, 2-large, 3-moderate, 4-minimal). The number of scar tissue segments identified in the AHA model4 was also assessed. For the animal study only, scar-myocardial, scar-blood and blood-myocardium relative contrast ratios5 were analyzed from images (PSIR and BL) acquired without ICD.
RESULTS
Animal: MR images are shown in Figure 2A and image scores in Figure 2B-D. In the presence of ICD, standard PSIR LGE images were degraded in the vicinity of the myocardium but preserved the ability to identify the infarct. Standard SPOT LGE images were, on the other hand, severely affected by hyperintensity artifacts over a large portion of the anterior left ventricular wall. Wideband PSIR and wideband SPOT LGE suppressed hyperintensity artifacts, with improved scar visualization using SPOT (contrast ratios in Figure 2E-G).The results of the histology (Figure 3) showed and confirmed the presence of dense fibro-fatty replacement with diffuse surviving myocardial fibers. These results correspond to the scar tissues visible on the MR images.
Patients: MR images are shown in Figure 4, with the fusion of wideband BL and BR images (wideband SPOT), as well as chest X-rays to localize the ICD. Reference standard PSIR LGE images were severely degraded by hyperintensity artefacts in four out of five patients, resulting in an overall low image quality (1.60 ± 0.89) and low artefact severity scores (1.8 ± 1.3), affecting the visualization of scar segment (1.0 ± 1.0) (Figure 5A-D). Wideband SPOT LGE successfully suppressed hyperintensity and ripple artefacts, improved image quality (3.80 ± 0.45) and artefact severity scores (3.80 ± 0.45), enabling better detection (with wideband BL) and localization (with wideband BR) of scar segments (2.60 ± 1.14).
DISCUSSION AND CONCLUSION
Our results from the animal study suggest that wideband SPOT in presence of ICD provides same image quality and artifact severity scores than reference standard PSIR without the presence of ICD. Our results from both the animal and patient studies showed that wideband SPOT LGE is more sensitive in detecting myocardial scars than reference PSIR LGE. This may allow for more precise and reliable assessment of myocardial scars, and impact on diagnosis and treatment of ICD patients. Furthermore, findings from histology of the sheep’s heart were in agreement with wideband SPOT LGE findings, demonstrating the validity of our proposed imaging technique. Further clinical validation in patients with both ischemic and non-ischemic heart disease is now warranted.Acknowledgements
This work was supported by funding from the French National Research Agency under grant agreements Equipex MUSIC ANR-11-EQPX-0030, ANR-21-CE17-0034-01, Programme d’Investissements d’Avenir ANR-10-IAHU04-LIRYC, ANR-22-CPJ2-0009-01, and from the European Research Council (ERC) under the European Union’s Horizon 2020 research and innovation program (grant agreement N°101076351).References
1. Rashid S, Rapacchi S, Vaseghi M, et al. Improved Late Gadolinium Enhancement MR Imaging for Patients with Implanted Cardiac Devices. https://doi.org/101148/radiol13130942. 2014;270(1):269-274. Accessed June 1, 2022. https://pubs.rsna.org/doi/abs/10.1148/radiol.13130942
2. Bustin A, Sridi S, Kamakura T, Jais P, Stuber M, Cochet H. Free-breathing joint bright- and black-blood cardiovascular magnetic resonance imaging for the improved visualization of ablation-related radiofrequency lesions in the left ventricle. EP Europace. 2022;24(Supplement_1). doi:10.1093/EUROPACE/EUAC053.594
3. Nezafat R, Stuber M, Ouwerkerk R, Gharib AM, Desai MY, Pettigrew RI. B1-insensitive T2 preparation for improved coronary magnetic resonance angiography at 3 T. Magn Reson Med. 2006;55(4):858-864. doi:10.1002/MRM.20835
4. Cerqueira MD, Weissman NJ, Dilsizian V, et al. Standardized myocardial sementation and nomenclature for tomographic imaging of the heart: A Statement for Healthcare Professionals from the Cardiac Imaging Committee of the Council on Clinical Cardiology of the American Heart Association. Circulation. 2002;105(4):539-542. doi:10.1161/HC0402.102975/FORMAT/EPUB
5. Sridi S, Nuñez-Garcia M, Sermesant M, et al. Improved myocardial scar visualization with fast free-breathing motion-compensated black-blood T1-rho-prepared late gadolinium enhancement MRI. Diagn Interv Imaging. 2022;103(12):607-617. doi:10.1016/J.DIII.2022.07.003
Figures
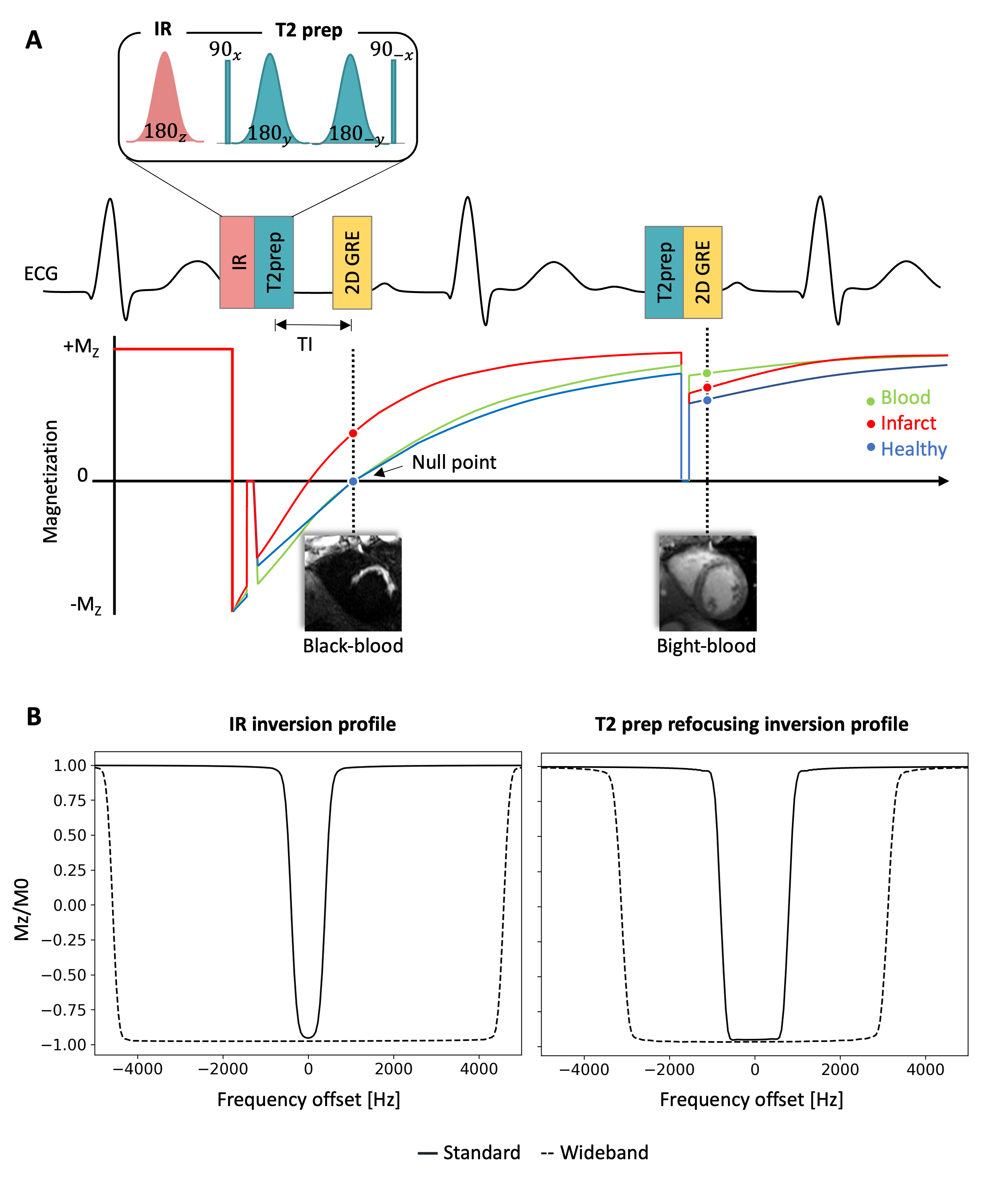
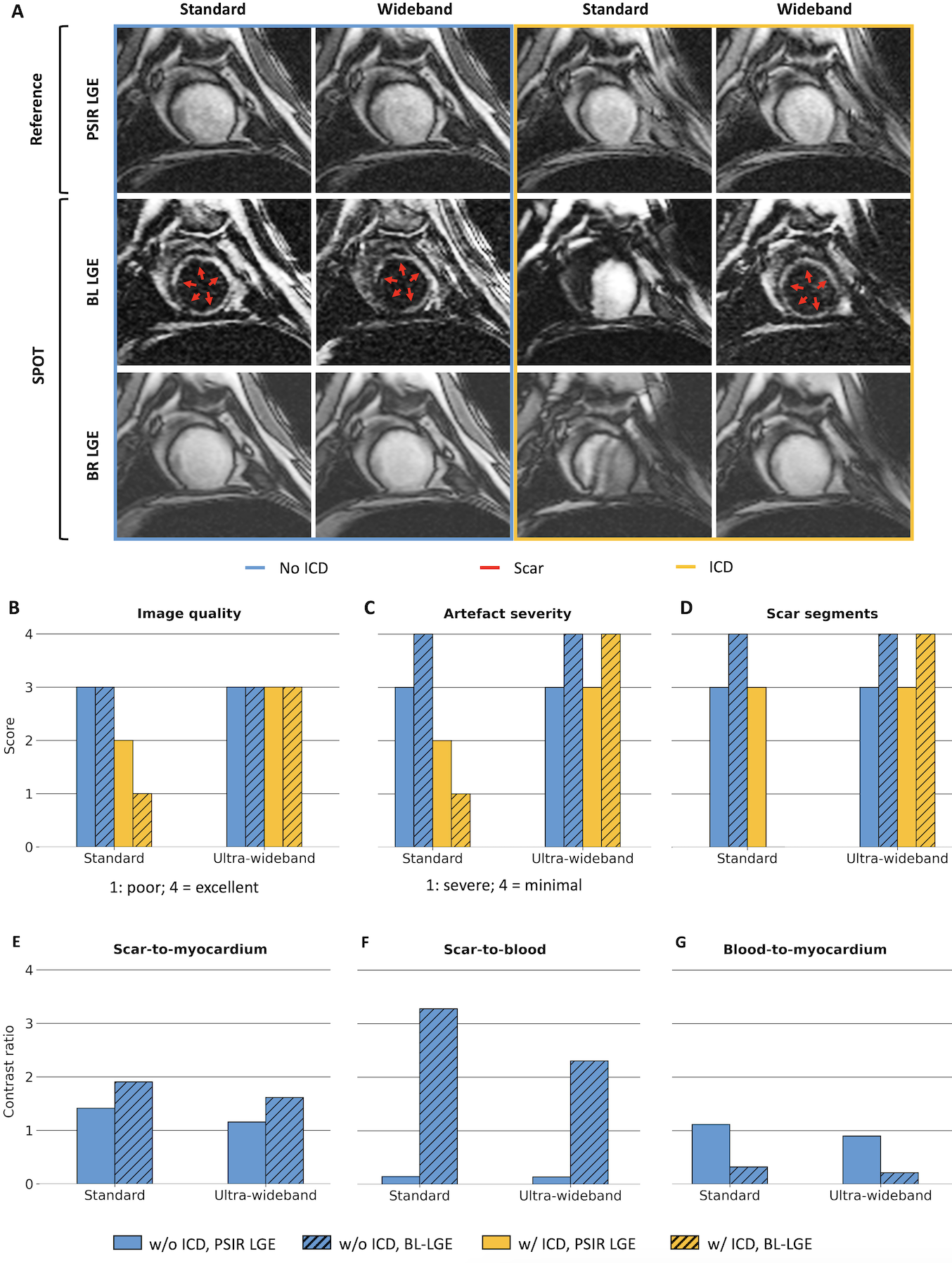
Figure 2: Results of image acquisition in the sheep. A) Top row: reference 2D PSIR LGE images. Middle row: 2D BL LGE images Bottom row: 2D BR LGE images. In the blue box (left): measurements without ICD. In the yellow box (right): measurements with ICD. B-D) Image quality and artifact severity scores, and number of detected scar segments with (yellow) and without (blue) ICD. E-G) Scar-myocardium, scar-blood, and blood-myocardium contrast ratios from PSIR and BL LGE images without ICD.
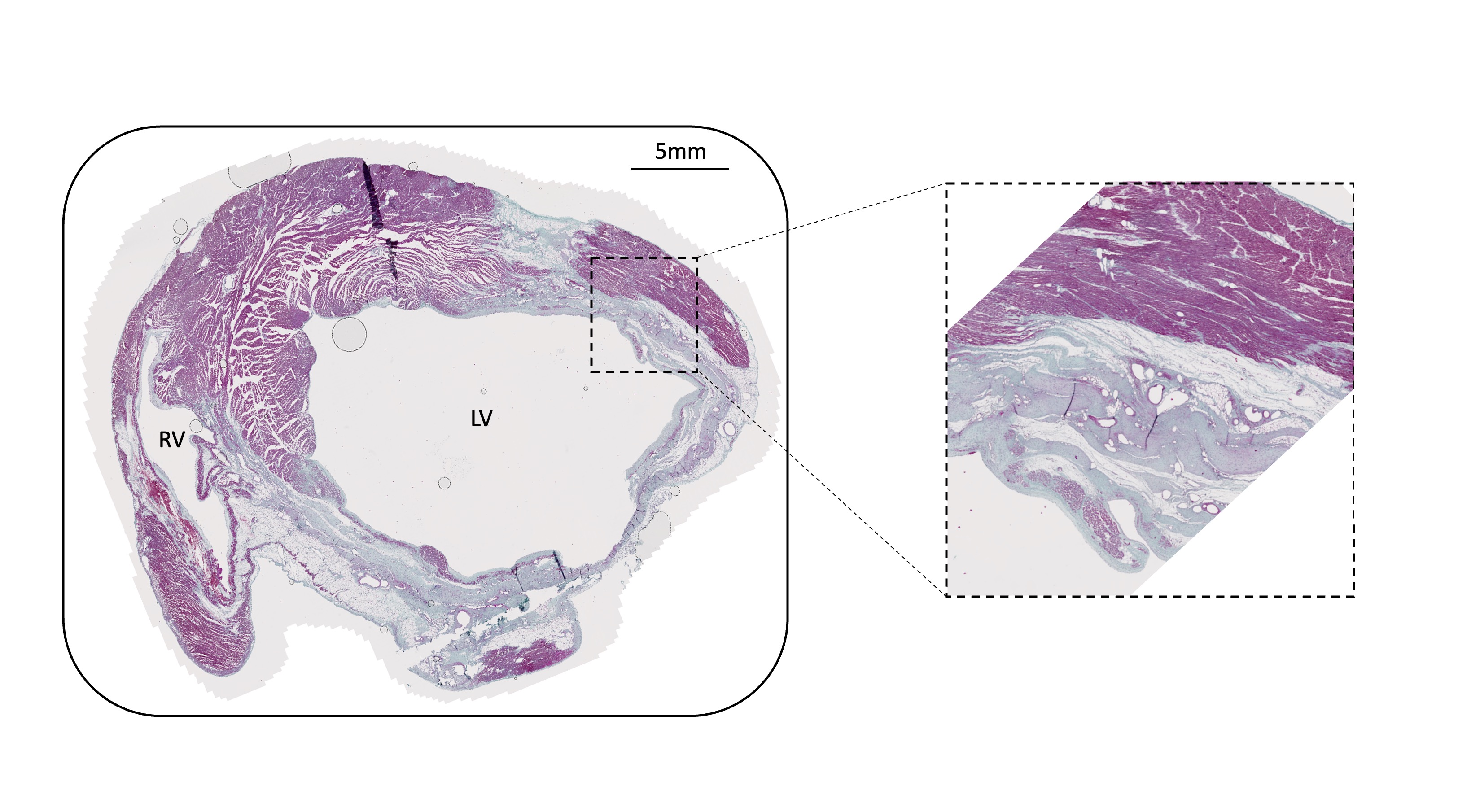
Figure 3: Masson’s trichrome staining of the cross-section identified by the white rounded rectangle, confirming the presence of dense fibro-fatty replacement with diffuse surviving myocardial fibers – dashed inset (red/purple=cardiomyocytes; blue=collagen).
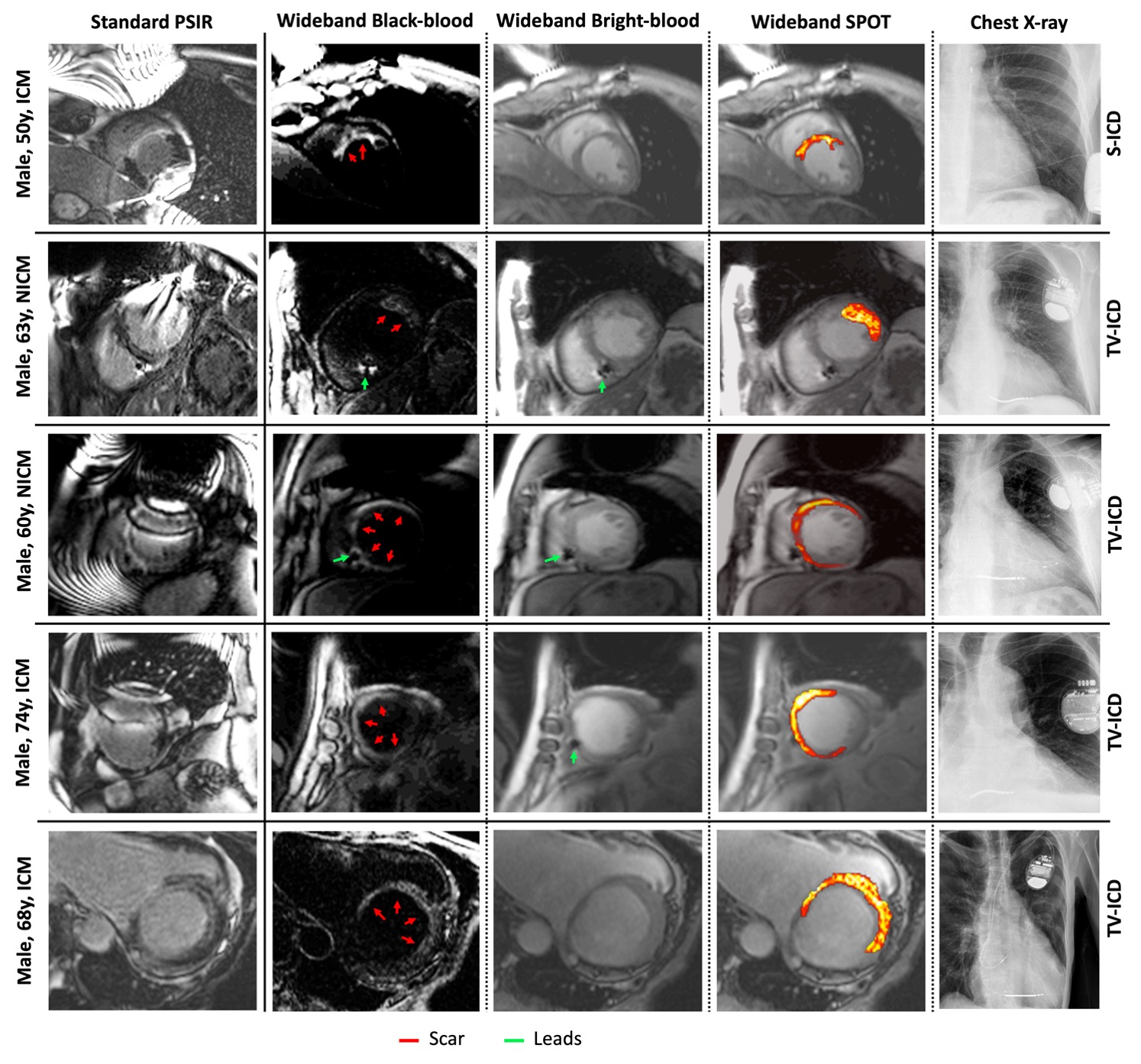
Figure 4: Patient results. From the left: First column: reference standard PSIR LGE images with presence of hyperintensity and ripple ICD-artifacts. Second column: wideband BL LGE images. Third column: wideband BR LGE images. Fourth column: Fusion of wideband BL and BR images. Fifth column: chest X-rays. Red arrow: scar tissue. Green arrow: ICD leads.
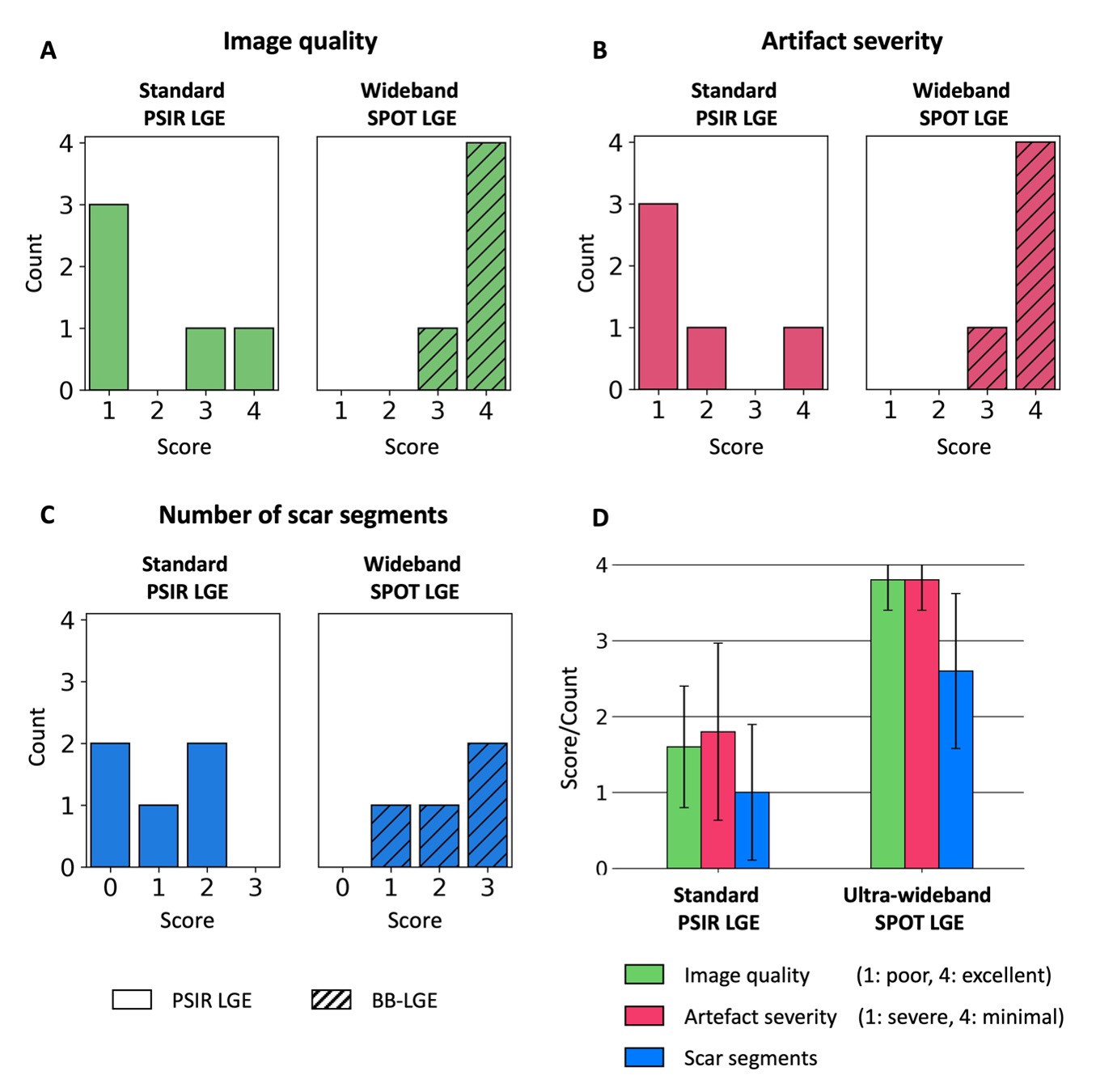
Figure 5: Patient results. A-C) Count of the different image quality- and artifact severity scores, and of the number of detected scar segments in all patients. D) Mean image quality and artifact severity scores and mean number (mean count) of scar segments for all patients, with standard deviations.