0942
Towards Integrating 3D Fetal Brain Slice-to-Volume Reconstruction in a 0.55T Scanner Environment with Gadgetron1Centre for the Developing Brain, School of Biomedical Engineering & Imaging Sciences, King's College London, London, United Kingdom, 2Biomedical Engineering Department, School of Biomedical Engineering & Imaging Sciences, King's College London, London, United Kingdom, 3Department of Women & Children’s Health, King's College London, London, United Kingdom, 4MR Research Collaborations, Siemens Healthcare Limited, Camberley, United Kingdom
Synopsis
Keywords: Data Acquisition, Data Acquisition, Fetal
Motivation: Fetal MRI is an important tool for antenatal diagnosis, allowing to assess appropriate growth with T2-weighted TSE sequences. Involuntary fetal motion is frozen in-plane with single-shot sequences, but 3D inconsistencies remain and are currently mostly addressed with offline slice-to-volume reconstruction.
Goal(s): The goal of this work is to integrate slice-to-volume reconstruction into a clinical fetal low-field scan.
Approach: A Gadgetron-based real-time pipeline including quality control, decision support, 3D reconstruction and transfer back to the scanner was implemented.
Results: The steps of the pipeline were successfully tested in-vivo in low-field fetal MRI.
Impact: The complete integration of Slice-to-Volume reconstruction into the normal clinical workflow and the resulting availability of high resolution 3D volumes during the scan overcomes challenges and current barriers of fetal MRI.
Introduction
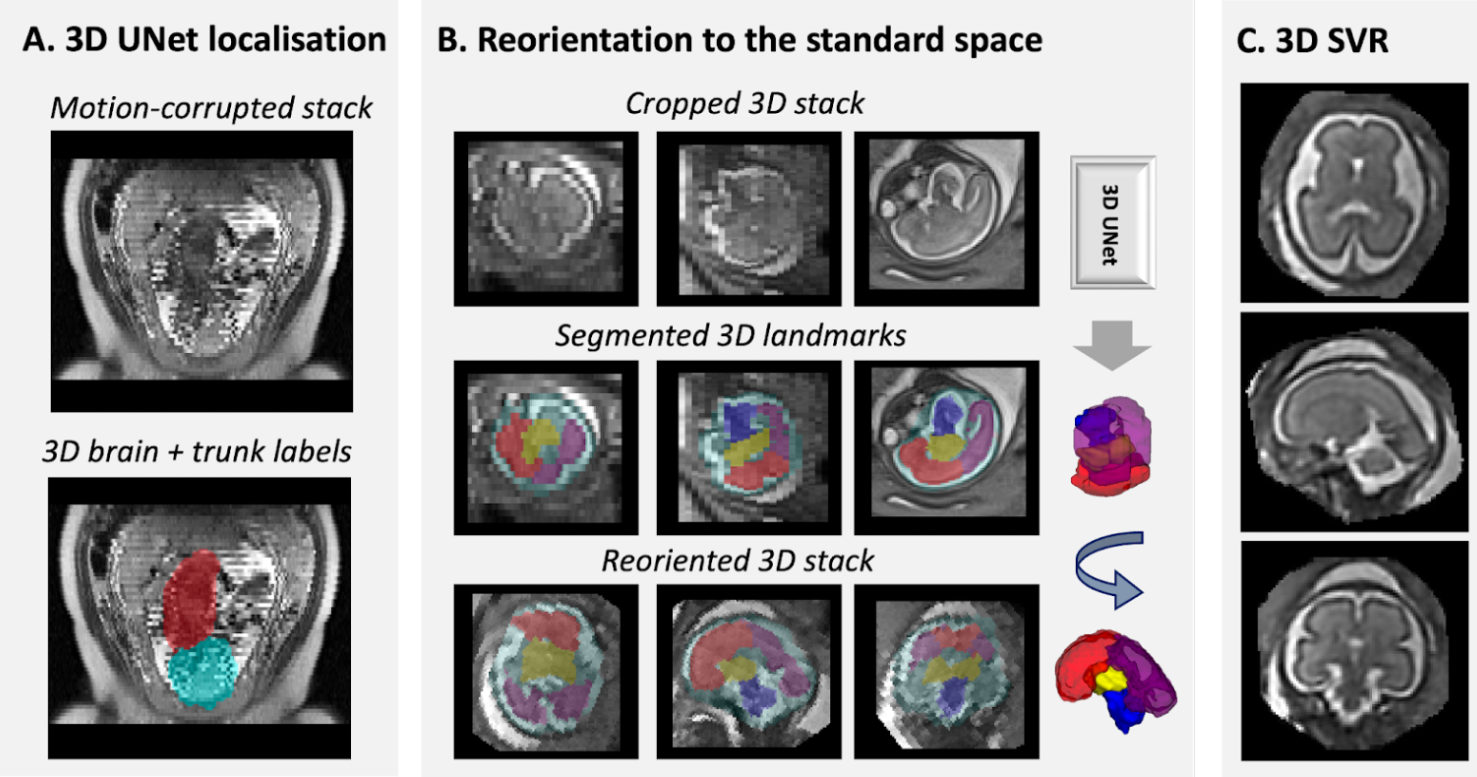
Fetal MRI is a key complementary modality to Ultrasound for antenatal diagnosis. Fast acquisition protocols, such as single-shot Turbo Spin Echo (ss-TSE) provide high in-plane 2D image quality but unpredictable fetal motion results in a loss of 3D structural continuity, preventing adequate radiological evaluation and triggering repeat scans in many cases. Motion correction techniques such as slice-to-volume super-resolution techniques allow reconstructing high-resolution 3D volumes from multiple motion corrupted stacks [1, 2, 3, 4]. However, currently, such approaches are therefore mostly limited to specialist centres and involve manual offline steps. Integration of such image reconstruction into clinical processes is crucial for translation. Recent work has integrated for example image quality assessment into the scan to assure adequate stacks are available [5].A further recent trend is the use of low field strength 0.55T MRI [6] for fetal MRI, promising for fetal imaging due to reduced susceptibility artefacts, improved comfort and improved accessibility [7,8]. However, addressing signal-to-noise ratio challenges is crucial. This study introduces an automated 3D reconstruction pipeline for low field 0.55T fetal MRI, making both a decision support system for individual TSE stacks and the final 3D reconstruction available during scan time.Methods
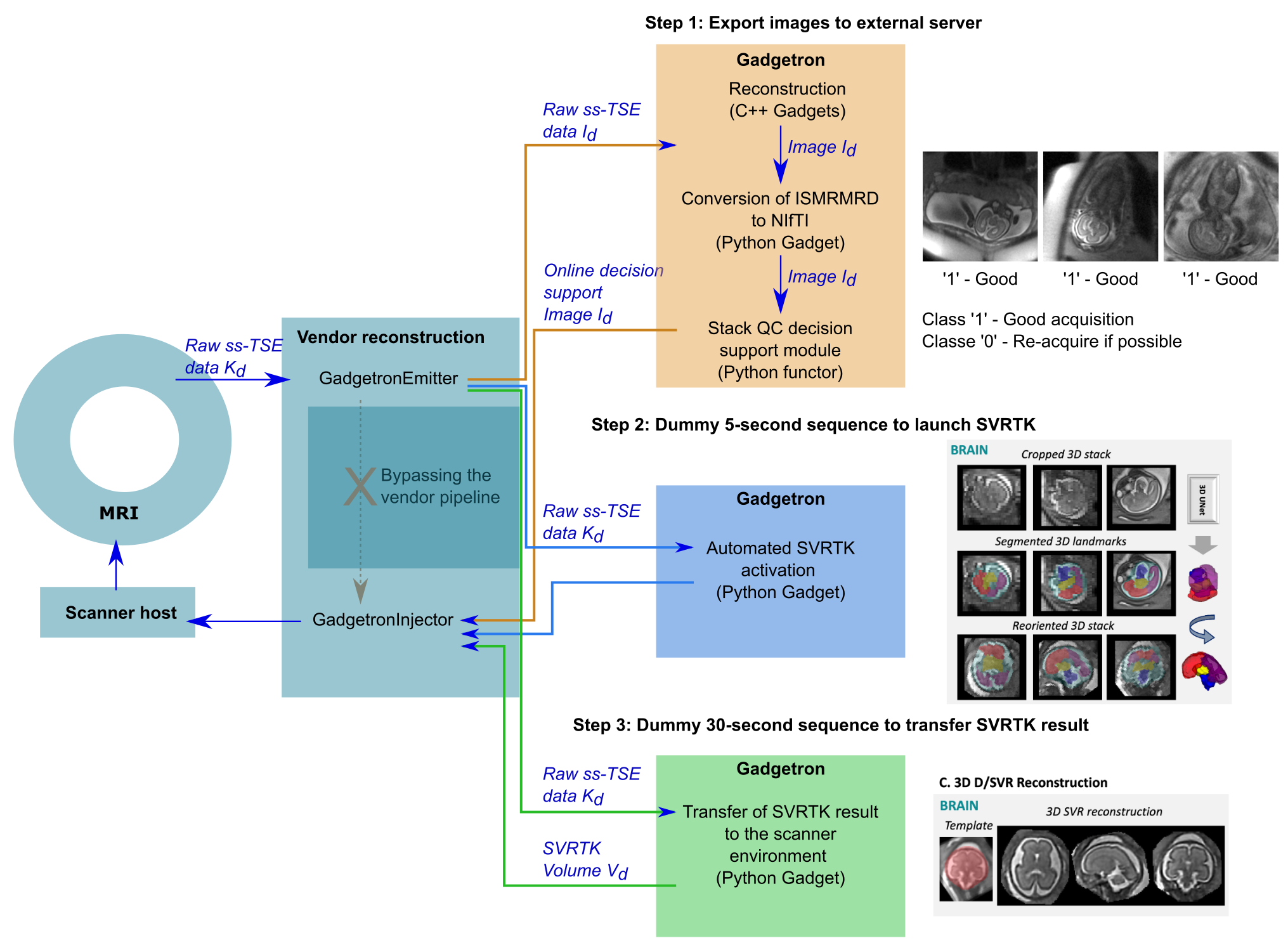
After informed consent to the MEERKAT study [REC19/LO/0852], pregnant women were scanned in supine position on a clinical 0.55T Free.Max Scanner. T2-weighted single-shot Turbo Spin Echo (FOV= 450X450mm2, resolution 1.5x1.5x4.5mm3, partial Fourier = 4/8, TR =2500ms. TE= 106ms, slices = 20-55) sequences were acquired coronal, sagittal and transverse with respect to the maternal habitus covering the entire uterus and with respect to the fetal brain, resulting in 6-9 (with occasional repeats) stacks. The Gadgetron framework [9] is adopted in this workflow to export the raw data to be reconstructed using off-the-shelf Gadgets. A Python Gadget follows where images are converted into the NIfTI format, required for further processing, and an online Stack Quality Control decision support classifier to provide real-time quality assessment of the images to determine if they are suitable for SVRTK reconstruction or if re-acquisition is advised. The classifier prediction is exported to the MRI host to support the radiographer and re-acquisition is recommended if the image quality is insufficient.After all stacks are collected, a 5-second dummy sequence is run to establish the connection between the scanner and the server to automatically activate the SVRTK docker, initialising the reconstruction process. This task is run as a subprocess to ensure no interference with the ongoing scanning.
Once the reconstructed volume is produced, a 30-second dummy sequence is used to re-connect to the external server for transferring the SVRTK result to the scanner environment - similarly to ensure no interference with the scanning process. The result is stored in the medical image database, alongside the acquired images, for future diagnostic analysis.
Results
Step 1 of the pipeline was tested in real-time in two fetal subjects, with acquisitions converted to NIfTI and analysed with the QA classifier. The SVRTK docker was initialised and run as a subprocess while continuing the protocol acquisition. Step 3 was tested separately for a different fetal subject, with the SVR reconstructed brain volume transferred to the scanner environment stored in the medical image database.Discussion and Conclusion
Crucial steps towards the implementation of the first automated 3D SVR reconstruction of the fetal brain on a 0.55T scanner were achieved using the here presented Gadgetron framework. The main novel components are the application of 3D reconstruction methods to low field fetal MRI and integration into the scanner environment. The immediate availability of both the online decision support, quality assessment and the final high-resolution 3D reconstruction allows for a more efficient acquisition by reducing repetitions to the minimum while delivering high quality data. The main current limitation is the mismatch between the ISMRMRD header parameters and the ones required for SVR reconstruction, such as rotation matrix and position. Further work includes testing the complete pipeline during clinical fetal scans and extending it to body SVR reconstruction.Acknowledgements
This work was supported by the EPSRC Doctoral Training Programme EP/R513064/1, the NIH Human Placenta Project grant 1U01HD087202-01 (Placenta Imaging Project (PIP)), a Sir Henry Wellcome Fellowship, a UKRI FL fellowship, a DFH Heisenberg professorship and by core funding from the Wellcome/EPSRC Centre for Medical Engineering [WT203148/Z/16/Z] and by the National Institute for Health Research (NIHR) Biomedical Research Centre based at Guy’s and St Thomas’ NHS Foundation Trust and King’s College London and the NIHR Clinical Research Facility. The authors would like to acknowledge the support of the Gadgetron group, particularly Michael Hansen and Hui Xue, and the radiographers, midwives and obstetricians who have contributed to this work.References
[1] Gholipour Ali, Estroff Judy A., Warfield Simon K. Robust super-resolution volume reconstruction from slice acquisitions: Application to fetal brain MRI. IEEE Transactions on Medical Imaging. 2010;29:1739-1758.
[2] Kuklisova-Murgasova Maria, Quaghebeur Gerardine, Rutherford Mary A., Hajnal Joseph V., Schnabel Julia A.. Reconstruction of fetal brain MRI with intensity matching and complete outlier removal. Med Image Analysis. 2012;16:1550-1564.
[3] Kainz, Bernhard, Steinberger, Markus, Wein, Wolfgang, et al. Fast Volume Reconstruction from Motion Corrupted Stacks of 2D Slices. IEEE Transactions on Medical Imaging. 2015;34:1901-1913.
[4] Kim K, Habas PA, Rajagopalan V, Scott JA, Corbett-Detig JM, Rousseau F, Barkovich AJ, Glenn OA, Studholme C. Bias field inconsistency correction of motion-scattered multislice MRI for improved 3D image reconstruction. IEEE Trans Med Imaging. 2011 Sep;30(9):1704-12.
[5] Faghihpirayesh, R., Karimi, D., Erdoğmuş, D., Gholipour, A. (2022). Deep Learning Framework for Real-Time Fetal Brain Segmentation in MRI. In: Licandro, R., Melbourne, A., Abaci Turk, E., Macgowan, C., Hutter, J. (eds) Perinatal, Preterm and Paediatric Image Analysis. PIPPI 2022. Lecture Notes in Computer Science, vol 13575. Springer, Cham. https://doi.org/10.1007/978-3-031-17117-8_6.
[6] Gowland PA, Freeman A, Issa B, Boulby P, Duncan KR, Moore RJ, Baker PN, Bowtell RW, Johnson IR, Worthington BS. In vivo relaxation time measurements in the human placenta using echo planar imaging at 0.5 T. Magn Reson Imaging. 1998 Apr;16(3):241-7.
[7] Aviles Verdera J, Story L, Hall M, Finck T, Egloff A, Seed PT, Malik SJ, Rutherford MA, Hajnal JV, Tomi-Tricot R, Hutter J. Reliability and Feasibility of Low-Field-Strength Fetal MRI at 0.55 T during Pregnancy. Radiology. 2023 Oct;309(1):e223050.
[8] Ponrartana, S., Nguyen, H.N., Cui, S.X. et al. Low-field 0.55 T MRI evaluation of the fetus. Pediatr Radiol 53, 1469–1475 (2023).
[9] Hansen MS, Sørensen TS. Gadgetron: an open source framework for medical image reconstruction. Magn Reson Med. 2013 Jun;69(6):1768-76. doi: 10.1002/mrm.24389.
Figures