0926
Interleaved 23Na/1H (pTx) MRI of the human heart at 7 Tesla1Institute of Radiology, University Hospital Erlangen, Friedrich-Alexander-Universität Erlangen-Nürnberg (FAU), Erlangen, Germany, 2Siemens Healthcare GmbH, Erlangen, Germany, 3Department of Nephrology and Hypertension, Friedrich-Alexander-Universität Erlangen-Nürnberg (FAU), Erlangen, Germany, 4Electrical Engineering and Information Technology, FH Aachen - University of Applied Sciences, Aachen, Germany, 5Division of Medical Physics in Radiology, German Cancer Research Centre (DKFZ), Heidelberg, Germany
Synopsis
Keywords: Non-Proton, Non-Proton, Sodium MRI, 23Na MRI, interleaved 23Na/1H MRI, High-Field MRI
Motivation: Interleaved dual-nuclear acquisition enables time-efficient 23Na and 1H cardiac MRI within one measurement. However, at 7T the reduced excitation wavelengths can lead to flip angle (FA) inhomogeneities in 23Na MRI and even to signal dropouts in 1H MRI. Both effects impair a reproducible quantitative evaluation of the myocardial 23Na signal.
Goal(s): To reduce FA inhomogeneities for interleaved 23Na/1H MRI.
Approach: We included three different pTx pulses in 1H MRI of the interleaved sequence and introduced a fast 23Na FA mapping.
Results: All three pTx pulses improved the 1H FA homogeneity and 23Na images showed better signal homogeneity after FA correction.
Impact: Interleaved 23Na/1H (pTx) MRI in combination with additional fast 23Na FA mapping is less prone to FA inhomogeneities and by that should enable reliable quantification of myocardial 23Na signal within clinically feasible acquisition times.
Introduction
Sodium (23Na) ions play an important role in various physiological processes and 23Na MRI might help to better understand cardiac and renal diseases.1,2 Nevertheless, for precise quantification of 23Na signals e.g. within the myocardium, it is essential to additionally acquire high-resolution 1H images for segmentation. As previously shown at 7T, this can be achieved in a time-efficient manner using interleaved 23Na/1H MRI.3 However, at ultra-high field strengths both 23Na and 1H excitation suffer from flip angle (FA) inhomogeneities, which impair the evaluability of the 23Na signal. To counteract this, FA correction was performed for 23Na MRI and parallel transmission (pTx) pulses were used for a more homogeneous 1H signal excitation.Methods
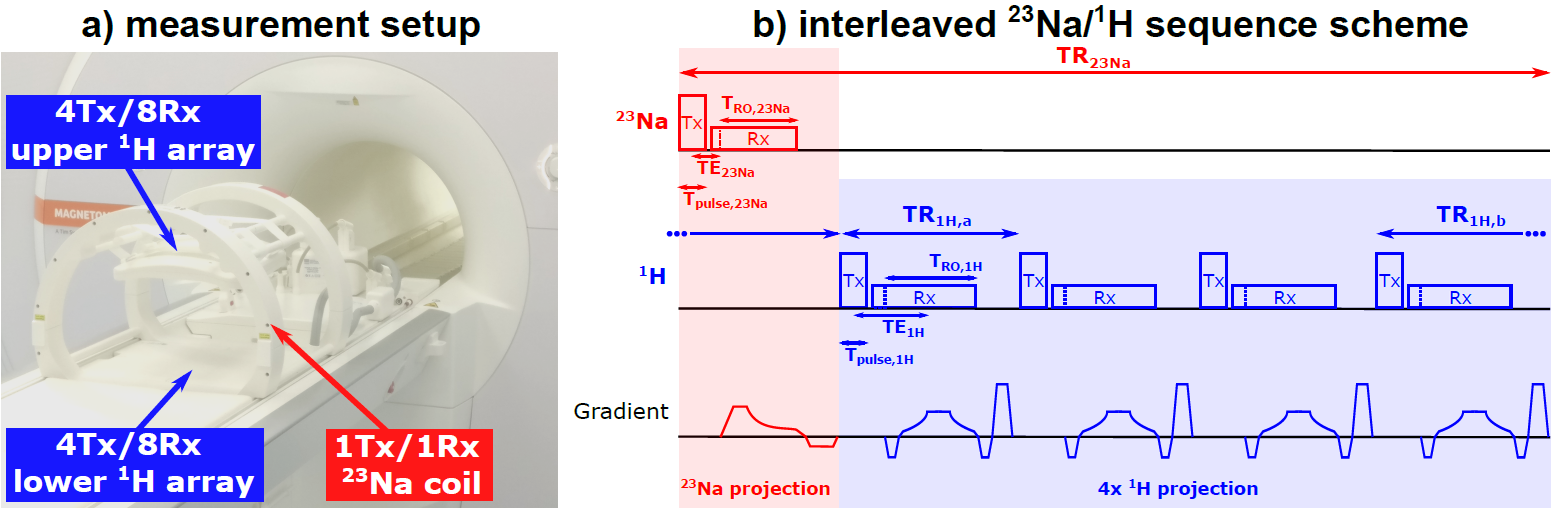
HardwareWith approval of the local ethics committee measurements of one healthy subject were performed at a 7T scanner (MAGNETOM Terra.X, Siemens Healthcare, Erlangen) using a combined 23Na/1H radiofrequency (RF) coil setup (Rapid Biomedical, Rimpar) (see Figure 1a). The setup consists of a 23Na RF volume coil and two 4Tx/8Rx 1H arrays allowing for interleaved 23Na/1H acquisition3 and the use of pTx for 1H MRI.
Measurements
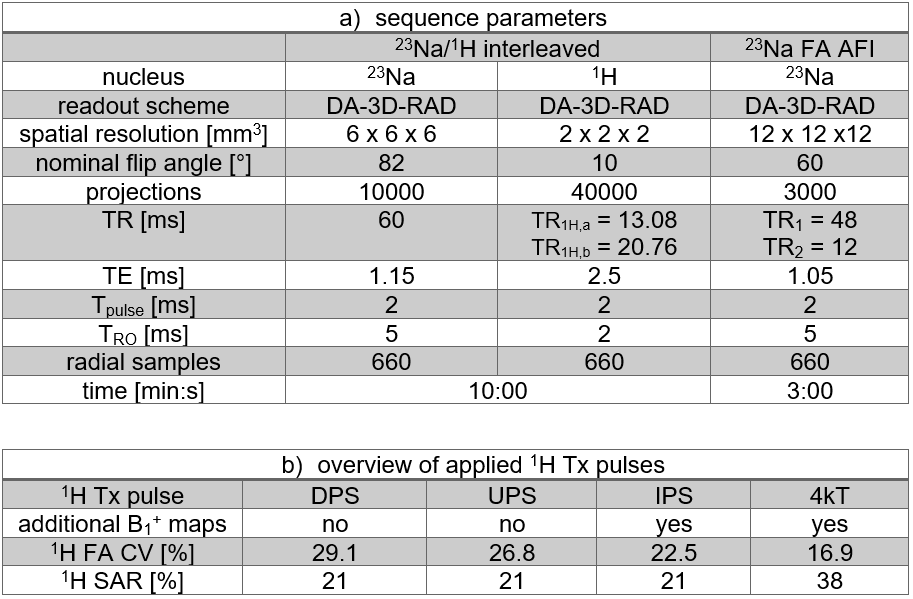
A 23Na/1H interleaved sequence with a density-adapted 3D radial readout4 was employed (see Figure 1b) enabling the acquisition of both 23Na and 1H MR data within one measurement. The projections were acquired in a golden angle scheme to allow for time-resolved reconstruction in the future.5 FA mapping for the 23Na RF coil was conducted using the actual flip-angle imaging (AFI) method.6 The Gaussian filtered (σ=14mm) FA map was used to correct the 23Na images based on Scorr=Suncorr/sin(FA). However, no B1- correction was applied yet. All sequence parameters are given in Table 1a.
Channel-wise relative B1+ maps7 were acquired (TA=6min) for the optimization of the 1H pTx pulses. Additionally, based on these maps the coefficient of variation (CV) of the FA was calculated within the heart for each 1H pulse as a measure of homogeneity. Apart from the vendor-provided cardiac default phase shim (DPS) three other pTx pulses were used for 1H excitation:
1. Universal phase shim (UPS): optimization of channel phases based on previously acquired cardiac B1+ maps of 35 subjects
2. Individual phase shim (IPS): optimization of channel phases based on B1+ maps of the currently measured subject8
3. Individual 4kT pulse (4kT): optimization of pulse amplitudes/phases of four sub-pulses and gradients between the sub-pulses based on B1+ maps of the currently measured subject9
Results
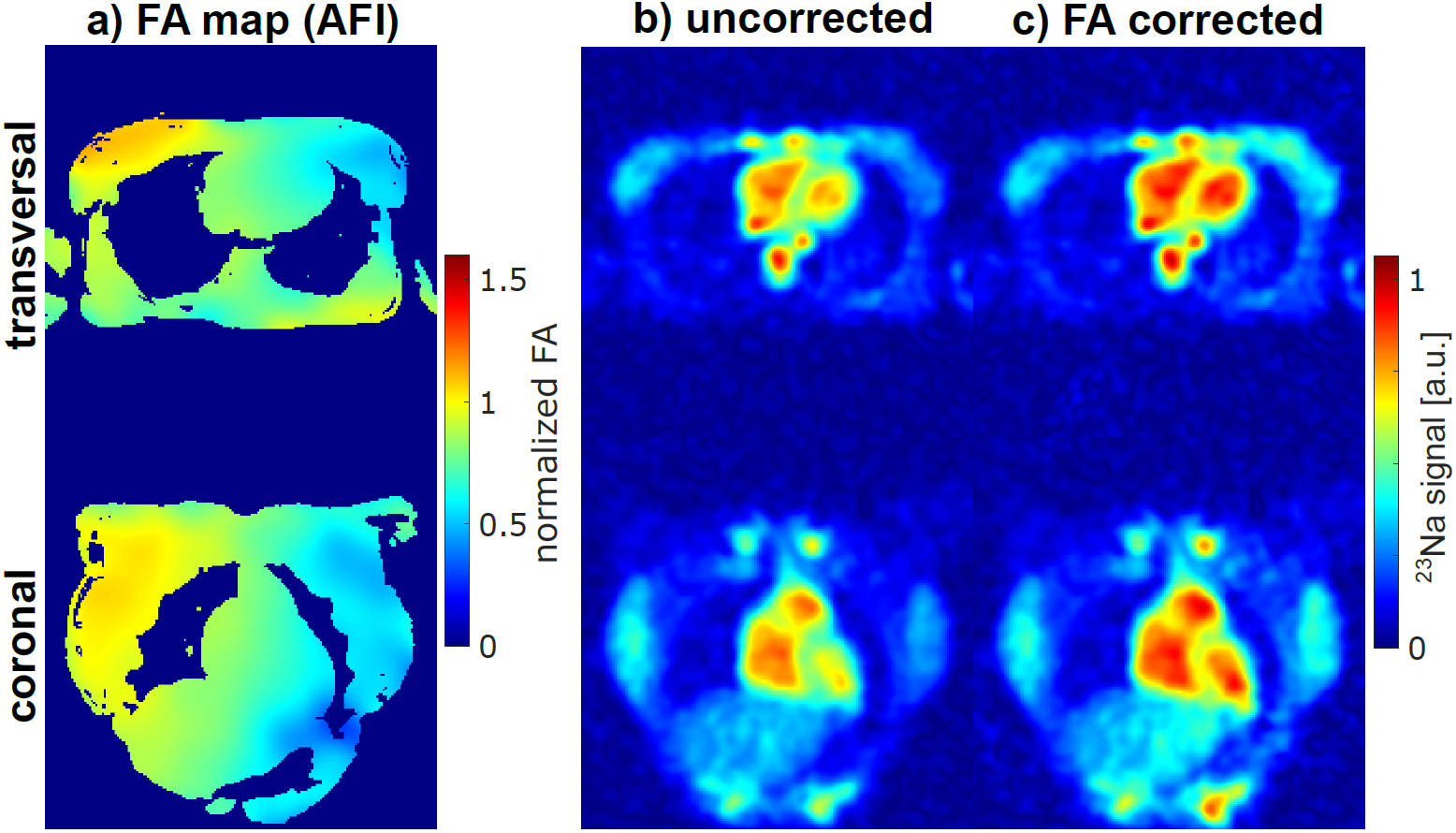
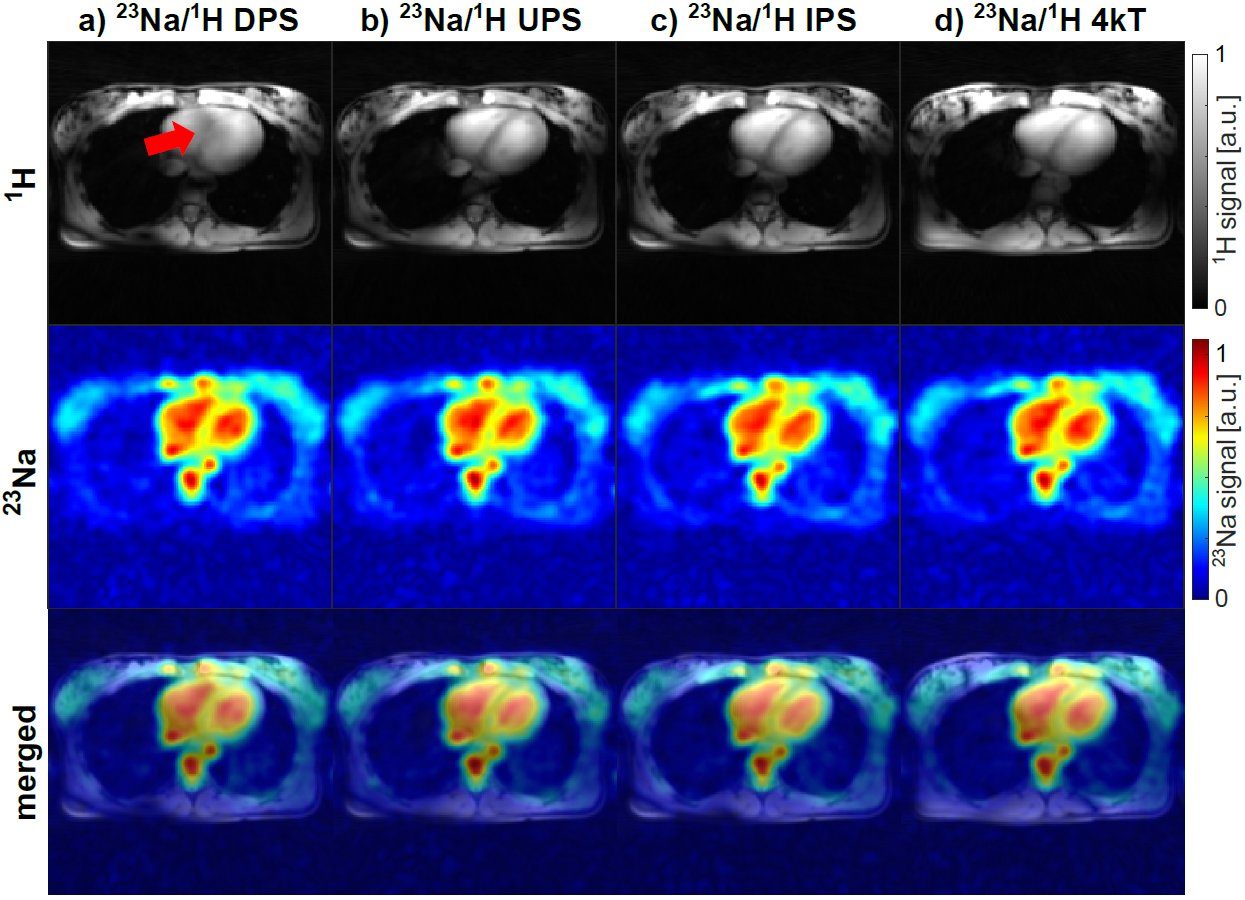
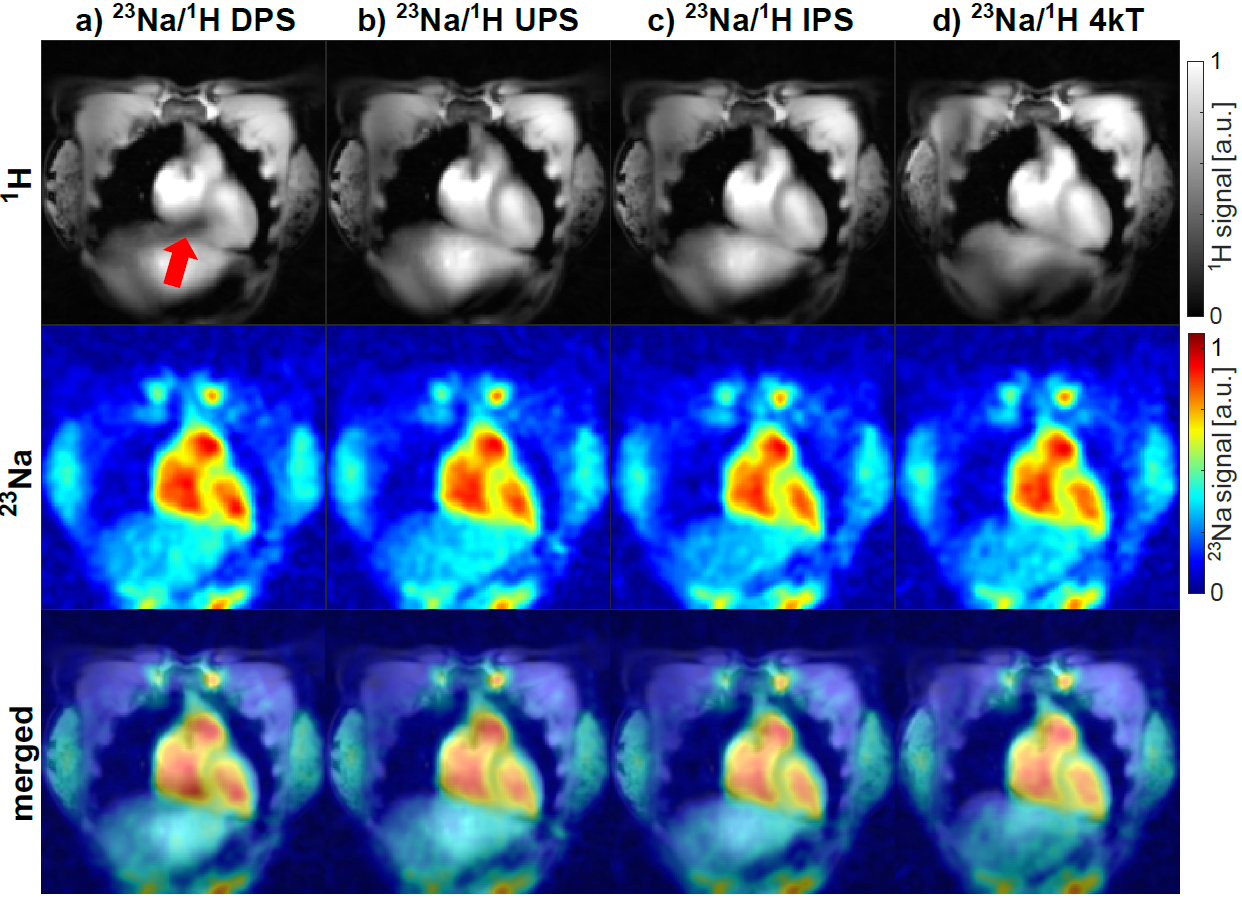
Figure 2a shows the FA distribution of the 23Na body coil. The FA in the heart is below the expected FA and decreases towards the lower left of the heart, which leads to a reduced 23Na signal in this region of the uncorrected 23Na image (see Figure 2b). After FA correction the 23Na signal in the heart is more homogeneous, which is particularly evident in the blood signal of the left and right ventricle (see Figure 2c).Figure 3 and 4 display the 1H and 23Na images of the interleaved 23Na/1H in vivo measurements in transversal and coronal view. Using the DPS (a) for 1H excitation, signal dropouts within the heart are visible. In contrast, a homogeneous excitation of the heart was achieved for the other three types of pTx pulses (b-d). Based on CV values within the heart (see Table 1b), the best FA homogeneity was achieved for the 4kT pulse followed by the IPS and UPS. However, latter result in a lower relative 1H SAR compared to the 4kT pulse (21% vs 38%). The 23Na images are not influenced by any of the 1H excitations and depict the quasi-same physiological state as the 1H images due to the interleaved acquisition.
Discussion and Conclusion
We have shown that 23Na/1H interleaved acquisition with 1H imaging in pTx mode is feasible at 7T. Previous work about interleaved X-nucleus/1H MRI used 1H MRI in single-channel transmit mode only.10,11 The best choice of the three examined pTx pulses depends on the target application. The UPS outperforms the DPS and is preferable for fast protocols, since no B1+ mapping is necessary. If additional B1+ mapping is acceptable, the usage of individually optimized pTx pulses results in even more homogeneous excitation within the heart. The 4kT pulse leads to the lowest CV. However, compared to the IPS the 1H SAR is higher, which reduces the available SAR for the 23Na MRI. Overall, using pTx for 1H excitation is essential for precise segmentation in the human abdomen. In combination with the presented fast 23Na FA mapping, interleaved 23Na/1H MRI (pTx) can enable reliable quantitative 23Na MRI in the human heart within clinically feasible acquisition times.Acknowledgements
This project was funded by the Deutsche Forschungsgemeinschaft (DFG) under 449552397.References
1. Sandstede JJ, Hillenbrand H, Beer M, et al. Time course of 23Na signal intensity after myocardial infarction in humans. MRM. 2004;52(3):545-551.
2. Akbari A, Lemoine S, Salerno F, et al. Functional Sodium MRI Helps to Measure Corticomedullary Sodium Content in Normal and Diseased Human Kidneys. Radiology. 2022;303(2):384-389.
3. Ruck L, Wilferth T, Gast LV, et al. Interleaved 23 Na/H MRI of the human heart at 7 Tesla. In Proceedings of the 30th Annual Meeting of ISMRM, London, UK 2022.
4. Nagel AM, Laun FB, Weber MA, Matthies C, Semmler W, Schad LR. Sodium MRI using a density-adapted 3D radial acquisition technique. Magn Reson Med. 2009;62(6):1565-1573.
5. Winkelmann S, Schaeffter T, Koehler T, Eggers H, Doessel O. An optimal radial profile order based on the Golden Ratio for time-resolved MRI. IEEE Trans Med Imaging. 2006;26(1):68-76
6. Yarnykh VL. Actual flip‐angle imaging in the pulsed steady state: a method for rapid three‐dimensional mapping of the transmitted radiofrequency field. Magn Reson Med. 2007;57(1):192-200.
7. Van de Moortele P-F, Ugurbil K. Very fast multi channel B1 calibration at high field in the small flip angle regime. In Proceedings of the 17th Annual Meeting of ISMRM, Honolulu, Hawaii, USA, 2009. 367.
8. Schmitter S, Wu X, Adriany G, Auerbach EJ, Uğurbil K, Van de Moortele PF. Cerebral TOF angiography at 7T: Impact of B1+ shimming with a 16‐channel transceiver array. Magn Reson Med. 2014;71(3):966-977.
9. Aigner CS, Dietrich S, Schaeffter T, Schmitter S. Calibration‐free pTx of the human heart at 7T via 3D universal pulses. Magn Reson Med. 2022;87(1):70-84.
10. Lopez Kolkovsky AL, Carlier PG, Marty B, Meyerspeer M. Interleaved and Simultaneous Multi‐Nuclear Magnetic Resonance in vivo. Review of Principles, Applications and Potential. NMR Biomed. e4735.
11. Wilferth T, Müller M, Gast LV, et al. Motion‐corrected 23Na MRI of the human brain using interleaved 1H 3D navigator images. Magn Reson Med. 2022.
Figures