0920
Simultaneous Multi-Slice Imaging in DKI and IVIM for Hepatocellular Carcinoma: Correlation with Microvascular Invasion and Histologic Grade1West China Hospital, Sichuan University, Chengdu, China, 2Radiology Department, Sanya People’s Hospital, Sanya, China
Synopsis
Keywords: Liver, Quantitative Imaging, Hepatocellular carcinoma (HCC); apparent diffusion coefficient (ADC); diffusion kurtosis imaging (DKI); Intravoxel incoherent motion diffusion-weighted imaging (IVIM); histologic grade; microvascular invasion (MVI)
Motivation: IVIM and DKI, effective in HCC malignancy prediction, face limitations due to lengthy scan times. The Simultaneous Multi-Slice (SMS) technology has successfully reduced scan times for ADC studies, but its application in IVIM and DKI remains underexplored.
Goal(s): To evaluate SMS-accelerated IVIM and DKI's efficacy in predicting HCC microvascular invasion (MVI) and tumor grading compared to conventional methods.
Approach: The study enrolled 42 HCC patients, conducting MRI with both conventional and SMS-accelerated DWI, DKI, and IVIM.
Results: SMS significantly reduced MRI scan times while maintaining reliable diffusion metrics, proving more effective than ADC in predicting MVI and tumor grades in HCC.
Impact: Integrating SMS into IVIM and DKI protocols can notably shorten scan times while preserving diagnostic accuracy in MVI and tumor grading, potentially improving clinical efficiency and patient management.
Introduction
Microvascular invasion (MVI) and tumor grading critically influence the prognosis of Hepatocellular Carcinoma (HCC) [1, 2]. Preoperative identification using Diffusion Weighted Imaging (DWI) could enable more tailored treatment strategies, potentially improving patient outcomes [3]. Advanced diffusion models like Diffusion Kurtosis Imaging (DKI) and Intravoxel Incoherent Motion (IVIM) offer detailed insights but are limited by long acquisition times. The Simultaneous Multi-Slice (SMS) technique promises to reduce these times while maintaining image quality [4, 5]. However, evaluating the precise impact of SMS on the prognostic accuracy of IVIM and DKI requires further investigation.Purpose
To assess the effectiveness of SMS-accelerated IVIM and DKI parameters for preoperative evaluation of MVI and histologic grading in HCC, compared to conventional methods.Materials and Methods
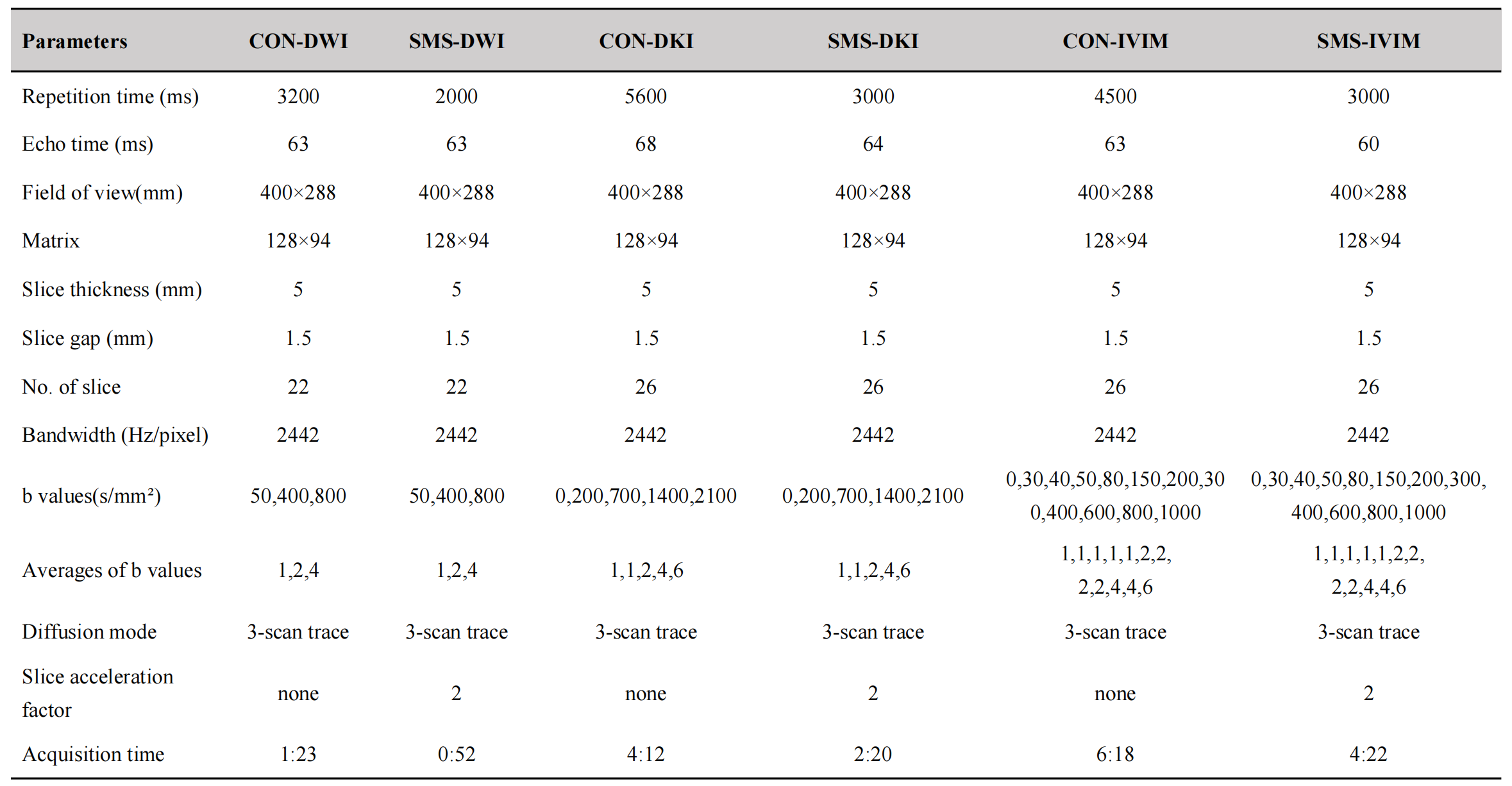
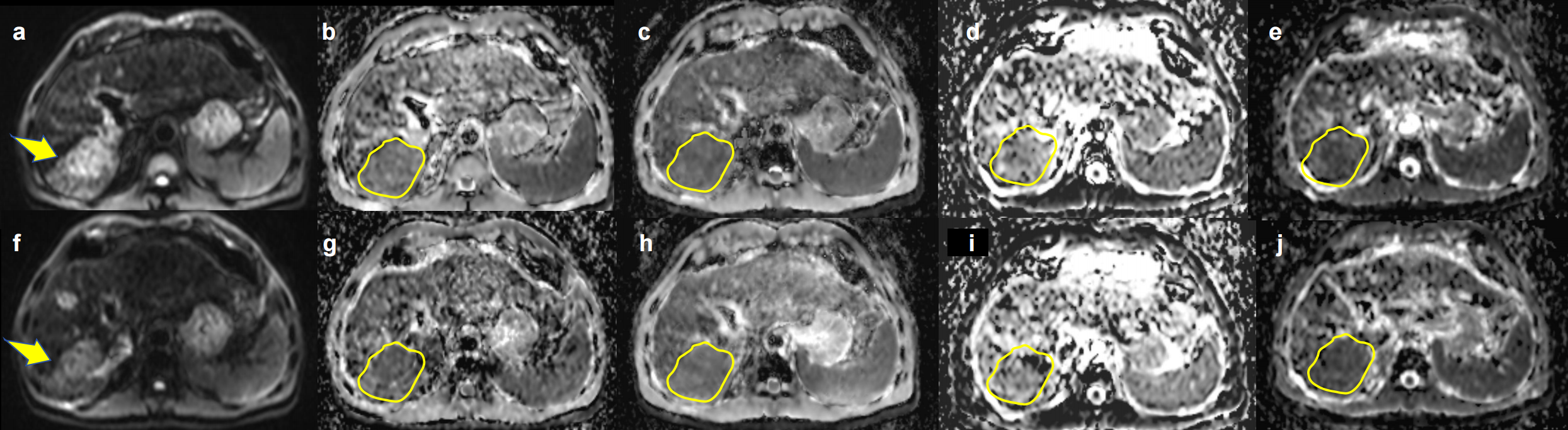
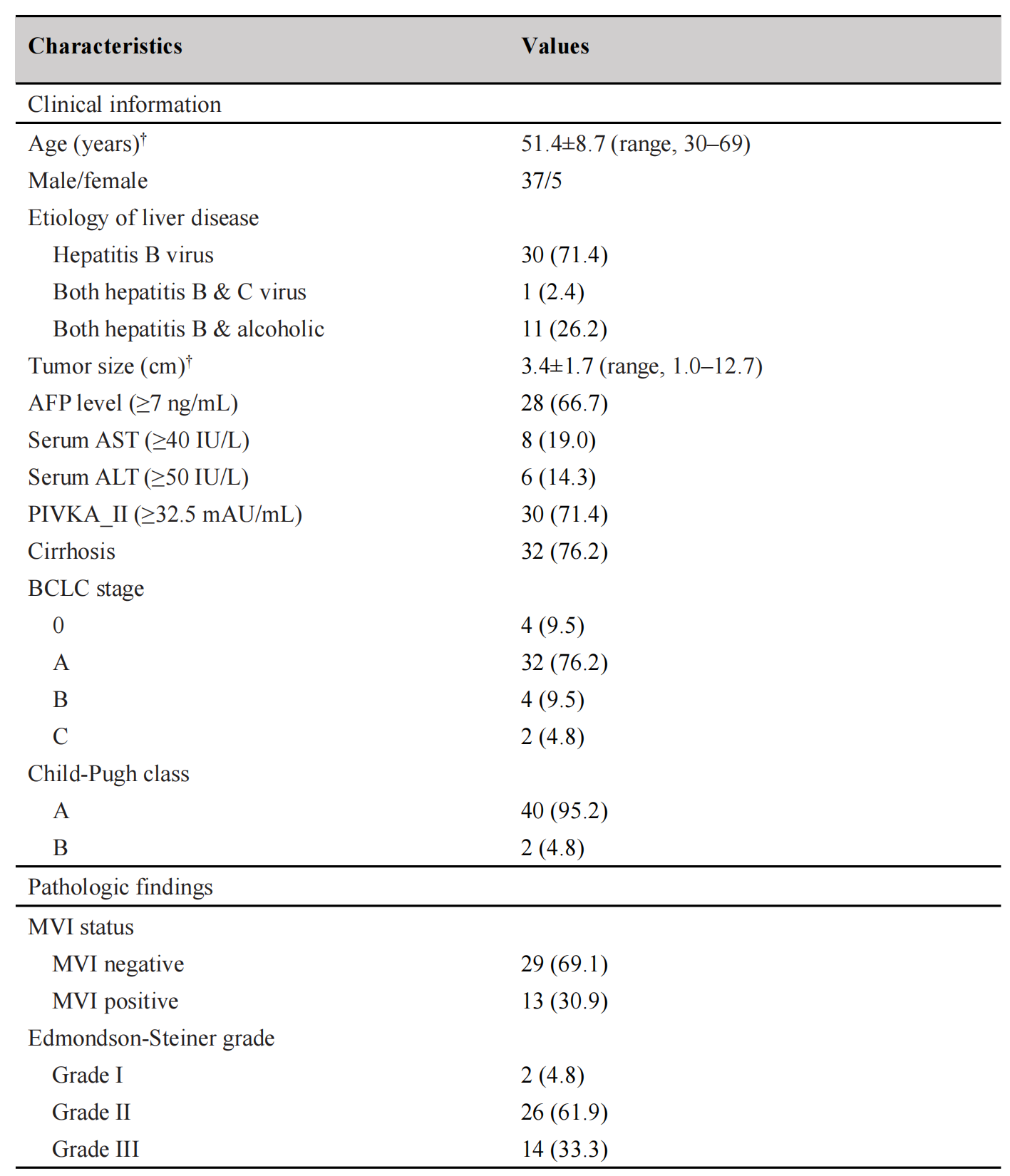
This prospective study was approved by the Institutional Review Board, with written informed consent obtained from all participants. A total of 42 patients (37 men, 5 women; mean age ± SD, 51.4 ± 8.7 years) with pathology-confirmed HCC were enrolled from June 2021 to November 2022. Preoperative MRI was conducted on a 3T MAGNETOM Skyra scanner (Siemens Healthineers, Erlangen, Germany) with an 18-channel body coil. Both conventional and SMS-accelerated diffusion-weighted sequences, including CON-DWI, SMS-DWI, CON-DKI, SMS-DKI, CON-IVIM, and SMS-IVIM, were utilized in a free-breathing setup (Figure 1). All images were transferred to a syngo.via frontiers workstation and subsequent analysis was carried out on a prototype MR Body Diffusion toolbox (v1.4.0), which generated apparent diffusion coefficient (ADC) for DWI, true diffusion coefficient (D), perfusion-related diffusion (D*), and perfusion fraction (f) for IVIM, and mean kurtosis (MK) and mean diffusivity (MD) for DKI. Two radiologists independently conducted ROI analysis for quantitative measurements, using free-hand ROIs on the largest tumor diameter slices of HCC lesions, excluding areas of necrosis and hemorrhage (Figure 2). Statistical analysis involved independent-sample t-test or Mann-Whitney U test was used to compare the diffusion parameters of different MVI status groups and different histopathological groups and pair t-test or Wilcoxon signed rank test to compare the diffusion parameters between conventional and SMS-accelerated groups. Diagnostic accuracy was evaluated using receiver operating characteristic (ROC) curve analyses.Results
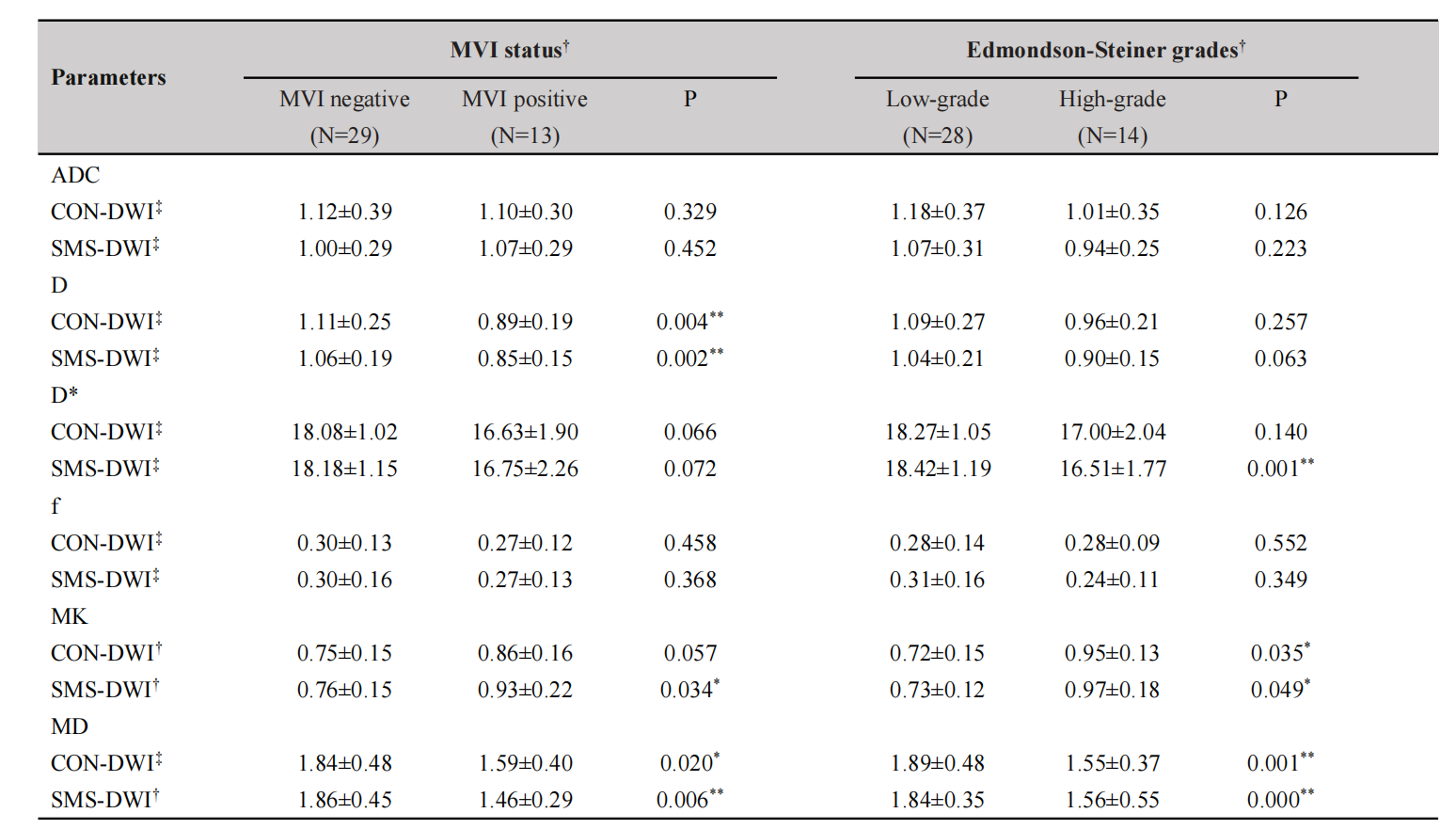
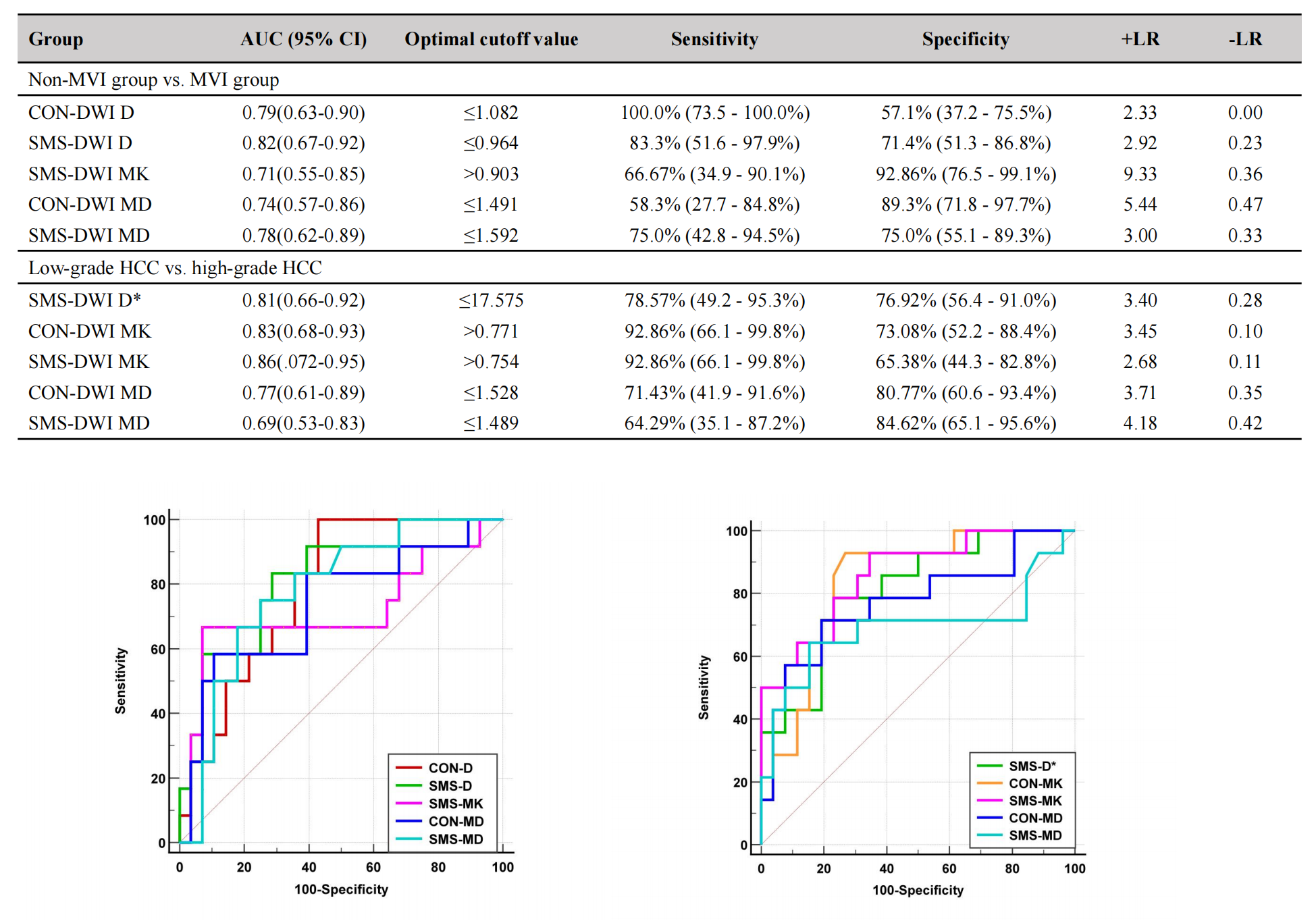
The acquisition times for SMS-DWI, SMS-DKI, and SMS-IVIM were reduced by 37.35%, 44.44%, and 30.69%, compared to conventional sequences, respectively. Quantitative diffusion metrics showed no significant difference between the conventional and SMS-accelerated sequences (all p-values > 0.05). Detailed patient characteristics are summarized in Figure 3. As shown in Figure 4, the MVI-positive group exhibited significantly lower D values (CON: 0.89±0.19 vs. 1.11±0.25, P=0.004; SMS: 0.85±0.15 vs. 1.06±0.19, P=0.002) and MD values (CON: 1.49±0.40 vs. 1.84±0.48, P=0.02; SMS: 1.46±0.29 vs. 1.86±0.45, P=0.006), and higher SMS-MK values (0.93±0.22 vs. 0.76±0.15, P=0.034) compared to MVI-negative HCCs. In distinguishing MVI-positive from MVI-negative HCC, SMS-D showed an AUC of 0.82, while CON-D exhibited a sensitivity of 1.00 (Figure 5). D and MD from both diffusion-weighted sequences and MK from SMS sequences differed significantly between the high-grade and low-grade HCCs (P=0.000-0.049) and showed moderate diagnostic efficacy (AUC=0.69-0.86).Discussion
We integrated SMS technology into the diffusion imaging protocols of IVIM and DKI to shorten MRI scan times [4]. Our analysis revealed no significant differences between the quantitative parameters of SMS-accelerated and conventional diffusion sequences, supporting the potential for clinical application of these advanced models. Our preliminary findings corroborate the superiority of IVIM and DKI over the mono-exponential model in characterizing the malignant behavior of HCC, in line with prior research [2, 6]. Specifically, the D appears to be a more reliable indicator of MVI than the ADC, likely because ADC conflates tissue cellularity and perfusion information. As HCC progresses, the increase in cellular density and perfusion falsely elevates ADC, whereas the D would not be affected [1, 2]. While perfusion parameters D* and f did not differ significantly between MVI-positive and MVI-negative HCC, this may be due to the variable vascularity in advanced malignancy masking their effects [7]. Furthermore, MK and MD offered better predictions of histologic grade and MVI status compared to ADC. Higher MK values correlated with tissue complexity, and lower MD values with cell density, both indicative of more aggressive characteristics [8]. Although MK showed higher AUCs, the differences across parameters were not marked. These insights suggest an intricate association between DKI and IVIM parameters and the biological behavior of HCC, meriting further investigation. Future studies with larger patient groups and comprehensive preoperative data are planned to further refine prognostic indicators for HCC.Conclusions
SMS significantly reduced MRI scan times while maintaining reliable diffusion metrics. IVIM-derived D values and DKI-derived MD and MK values outperformed conventional ADC values for predicting MVI and histologic grade of HCC.Acknowledgements
This study was supported by the National Natural Science Foundation of China (Grant number 82302161) and China Postdoctoral Science Foundation (Grant number 2023M732464).References
1. Wang WT, Yang L, Yang ZX, et al. Assessment of Microvascular Invasion of Hepatocellular Carcinoma with Diffusion Kurtosis Imaging. Radiology 2018;286:571-580.
2. Woo S, Lee JM, Yoon JH, et al. Intravoxel incoherent motion diffusion-weighted MR imaging of hepatocellular carcinoma: correlation with enhancement degree and histologic grade. Radiology 2014;270:758-767.
3. Surov A, Pech M, Omari J, et al. Diffusion-Weighted Imaging Reflects Tumor Grading and Microvascular Invasion in Hepatocellular Carcinoma. Liver Cancer 2021;10:10-24.
4. Taron J, Martirosian P, Erb M, et al. Simultaneous multislice diffusion-weighted MRI of the liver: Analysis of different breathing schemes in comparison to standard sequences. J Magn Reson Imaging 2016;44:865-879.
5. Obele CC, Glielmi C, Ream J, et al. Simultaneous Multislice Accelerated Free-Breathing Diffusion-Weighted Imaging of the Liver at 3T. Abdom Imaging 2015;40:2323-2330.
6. Choi IY, Lee SS, Sung YS, et al. Intravoxel incoherent motion diffusion-weighted imaging for characterizing focal hepatic lesions: Correlation with lesion enhancement. J Magn Reson Imaging 2017;45:1589-1598.
7. Matsui O, Kobayashi S, Sanada J, et al. Hepatocelluar nodules in liver cirrhosis: hemodynamic evaluation (angiography-assisted CT) with special reference to multi-step hepatocarcinogenesis. Abdom Imaging 2011;36:264-272.
8. Rosenkrantz AB, Padhani AR, Chenevert TL, et al. Body diffusion kurtosis imaging: Basic principles, applications, and considerations for clinical practice. J Magn Reson Imaging 2015;42:1190-1202.
Figures