0919
MRI-based prediction of microvascular invasion or high tumor grade and adjuvant therapy benefit for solitary HCC ≤5 cm1Radiology, West China Hospital, Sichuan University, Chengdu, China, 2Zhongda Hospital, Southeast University, Nanjing, China, 3West China Hospital, Sichuan University, Chengdu, China, 4Hôpital Beaujon, Clichy, France, 5Memorial Sloan Kettering Cancer Center, New York, NY, United States, 6University of California San Diego, San Diego, CA, United States, 7Duke University Medical Center, Durham, NC, United States, 8Sanya People’s Hospital, Sanya, China
Synopsis
Keywords: Liver, Liver
Motivation: Noninvasive assessment of high-risk histopathology (microvascular invasion or Edmondson-Steiner G3/4) for early HCC is critical but challenging.
Goal(s): To develop an MRI-based diagnostic model for high-risk histopathology.
Approach: This dual-center retrospective study included consecutive patients who underwent contrast-enhanced MRI and subsequent curative resection or RFA for solitary BCLC 0/A HCC≤5 cm. A diagnostic model was developed against pathology based on resection-treated patients.
Results: 554 patients were included. Serum α-fetoprotein, non-simple nodular growth subtype, and the VICT2 trait constituted the model (testing center AUC, 0.828). Adjuvant therapies were associated with improved RFS (resection, P=.009; RFA, P=.009) for the model-positive patients.
Impact: This dual-center study developed and externally validated a diagnostic model which could effectively predict high-risk histopathology and adjuvant therapy benefit for patients receiving curative resection or radiofrequency ablation for solitary BCLC 0 or A HCCs ≤5 cm.
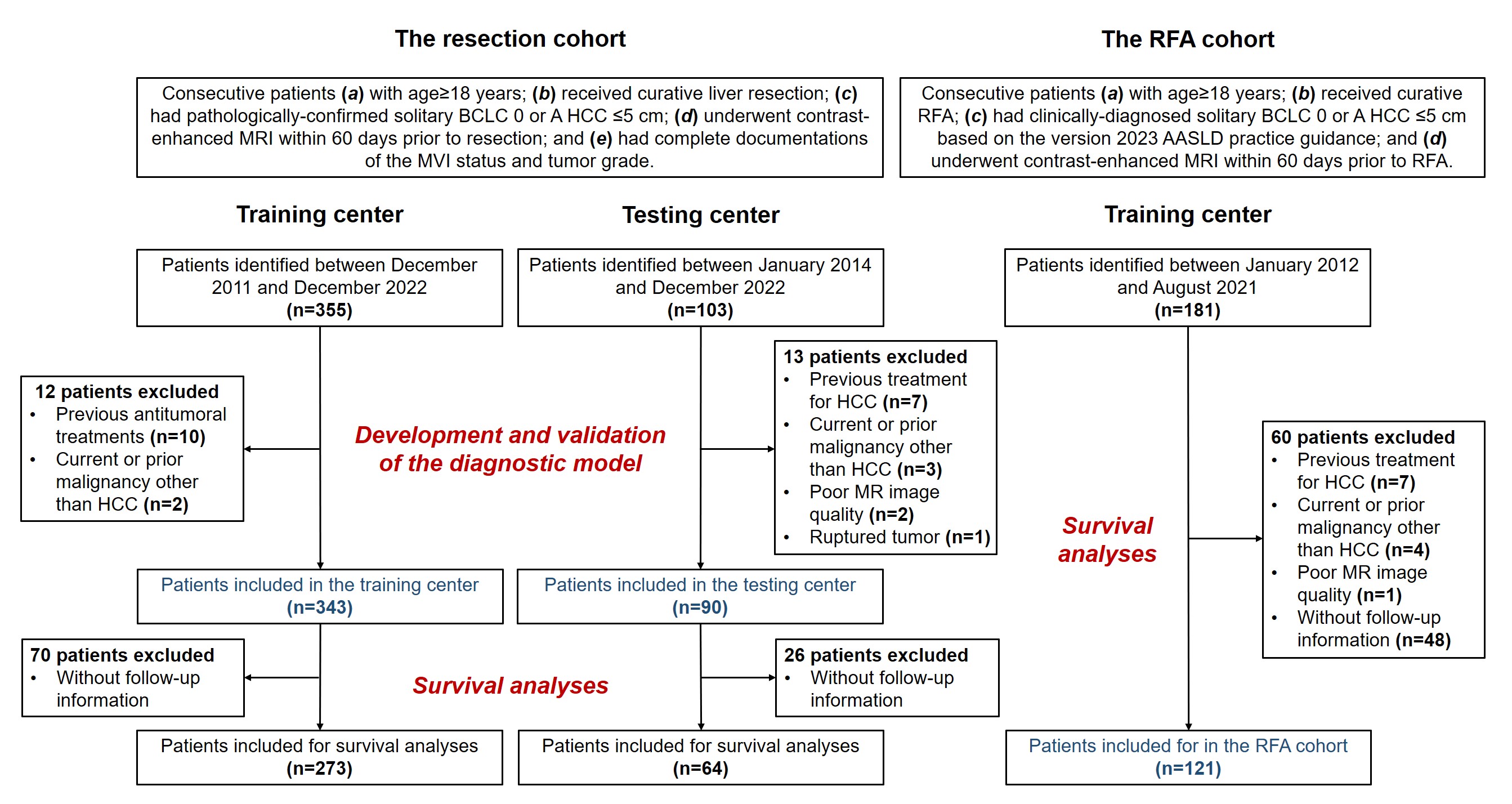
Methods: This dual-center retrospective study included consecutive adult patients who underwent contrast-enhanced MRI and subsequent curative resection (the resection cohort) or RFA (the RFA cohort) for solitary BCLC 0 or A HCCs ≤5 cm from two tertiary-care academic hospitals. Fifty MRI features were independently evaluated by three fellowship-trained blinded abdominal radiologists at each hospital. For the resection cohort, a diagnostic model was developed using training center data with logistic regression analyses against pathology, and validated using testing center data with the area under the receiver operating characteristic curve (AUC), sensitivity and specificity. The model’s utilities to predict posttreatment RFS and adjuvant therapy benefit were evaluated with the Kaplan-Meier method.
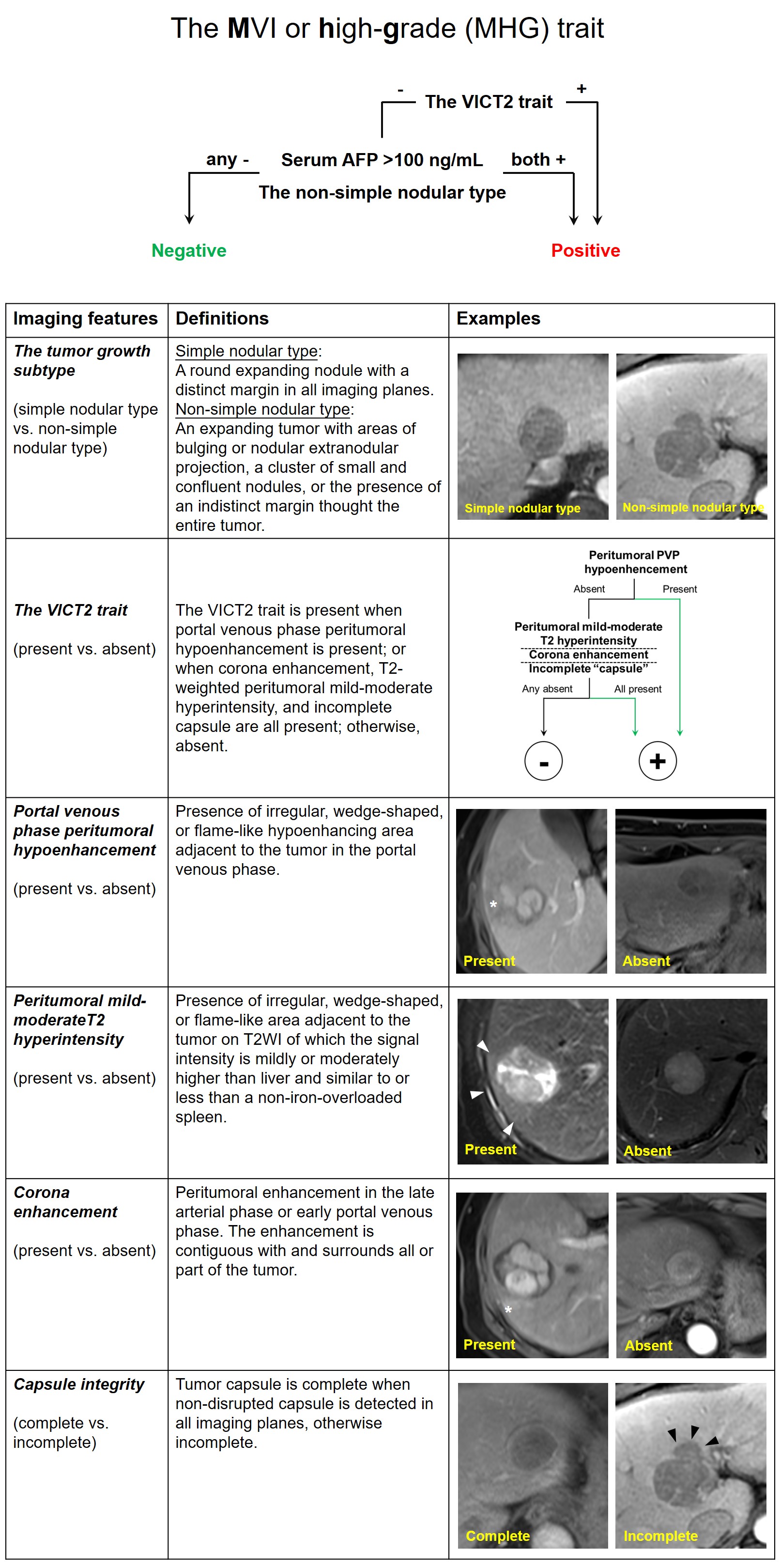
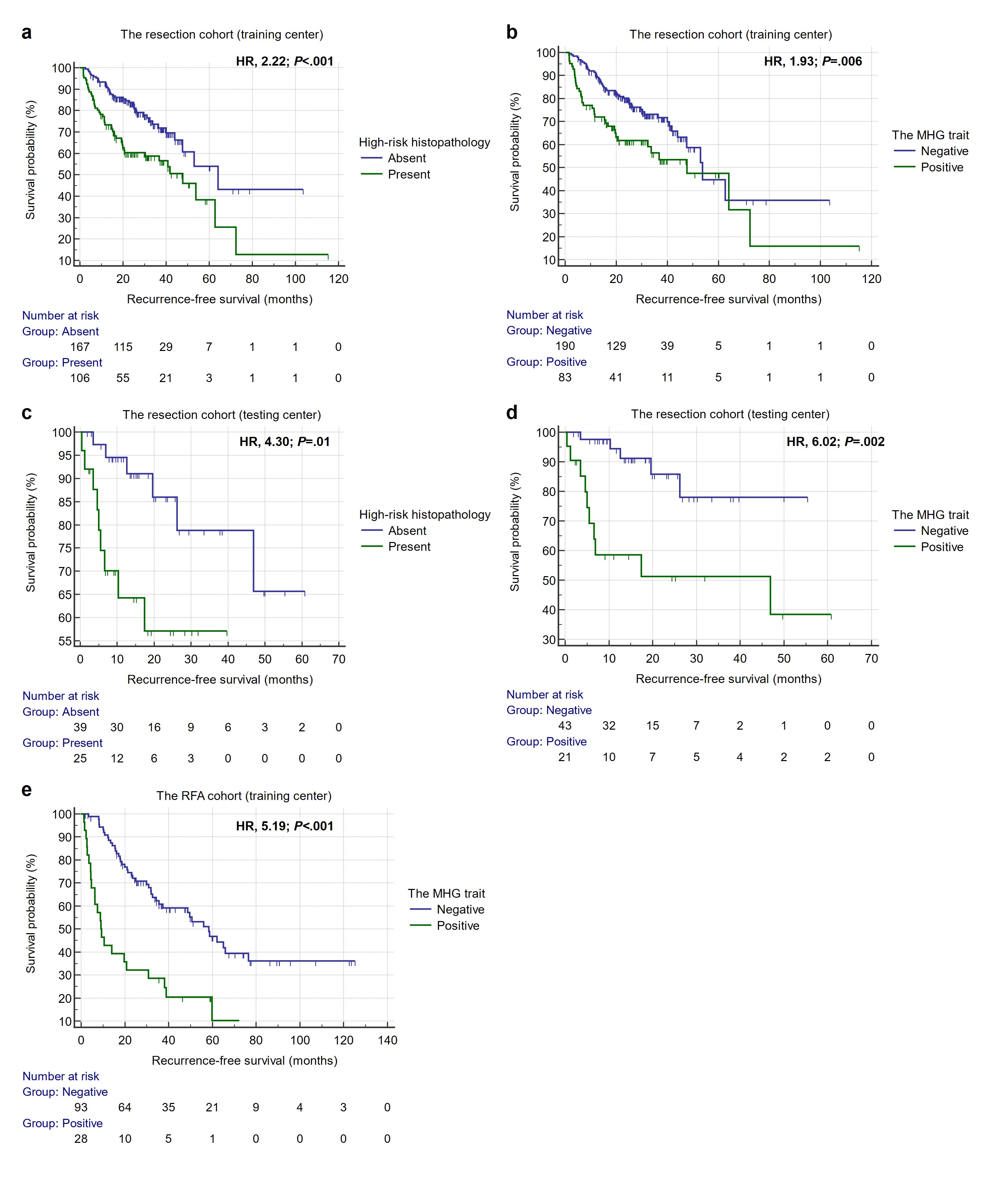
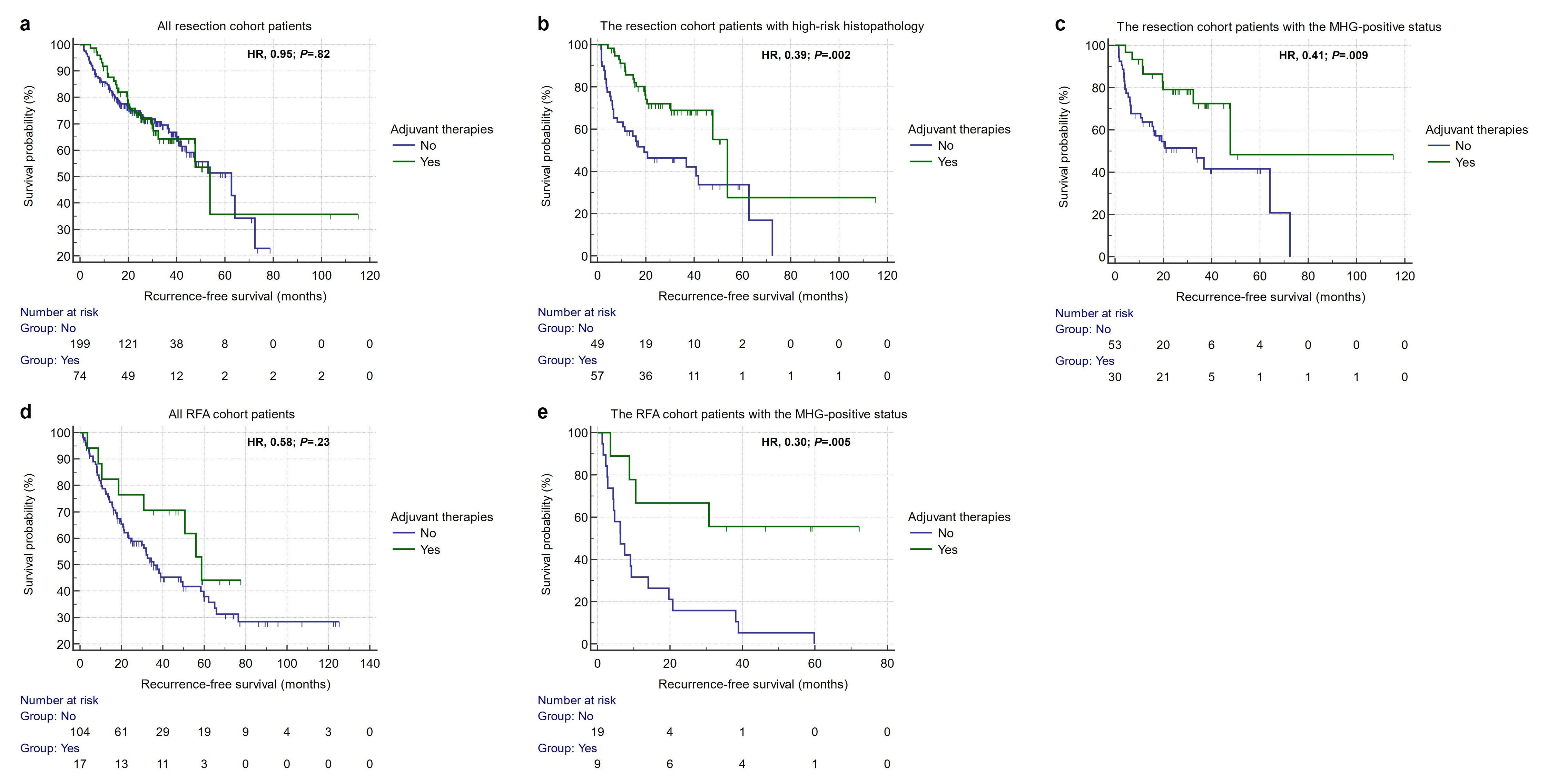
Results: 554 patients were included (the resection cohort, n=433 [training center, n=343; testing center, n=90], 173 [40.0%] with the high-risk histopathology; the RFA cohort, n=121 [all from training center]). Serum α-fetoprotein>100 ng/mL (odds ratio [OR], 1.94; P=.006), non-simple nodular growth subtype (OR, 1.69; P=.03), and the VICT2 trait (OR, 4.49; P<.001) were included in the MVI or high-grade (MHG) trait, with testing center AUC, sensitivity, and specificity of 0.828, 60.0%, and 85.5%, respectively. RFS was worse for the MHG-positive patients for both the resection (training center, hazard ratio [HR], 1.93, P=.006; testing center, HR, 6.02, P=.002) and RFA cohorts (HR, 5.19; P<.001). Adjuvant therapies were associated with improved RFS (resection, HR, 0.41, P=.009; RFA, HR, 0.30, P=.009) for the MHG-positive patients, but not for the MHG-negative ones (resection, P=.12; RFA, P=.56).
Discussion: The MHG trait may serve as a noninvasive diagnostic tool for high-risk histopathology and a decision-making tool for individualized prognostication and adjuvant therapy administration. For both the resection and RFA cohorts, the MHG-positive patients had worse RFS than the MHG-negative ones. More importantly, for both cohorts, the use of adjuvant therapies was associated with improved RFS for the MHG-positive patients but not the MHG-negative ones. Despite the critical utility of high-risk histopathology as an indicator for the use of adjuvant therapies (3-5), the MVI status and Edmondson-Steiner grade are not typically evaluated for RFA-treated HCC. Therefore, there remains a paucity of effective decision-making tool to inform the use of adjuvant therapies for RFA-treated solitary BCLC 0/A HCC, and our findings underscored the potential of the MHG trait to address such challenges. Moreover, for patients with good performance status and preserved liver function, we speculated that those with the MHG-positive status may benefit from more intensive treatment options, such as surgery over ablation, anatomic over non-anatomic resections, wide over narrow resection margins, and neoadjuvant therapies (7,8). Nevertheless, these potential treatment modifications were either derived from small-scale single-center retrospective data or largely hypothetical, and any reliable conclusion would require intensive external prospective validations, ideally in the settings of clinical trials.
Conclusion: The MHG trait could predict high-risk histopathology, posttreatment RFS and adjuvant therapy benefit for patients receiving curative resection or RFA for solitary BCLC 0 or A HCCs ≤5 cm.
Acknowledgements
No acknowledgement found.References
1. Singal AG, Llovet JM, Yarchoan M, et al. AASLD practice guidance on prevention, diagnosis, and treatment of hepatocellular carcinoma. Hepatology. 2023. doi: 10.1097/HEP.0000000000000466.
2. General Office of National Health Commission. Standard for diagnosis and treatment of primary liver cancer (2022 edition). J Clin Hepatol. 38 (2), 306-321.
3. Li J, Xing J, Yang Y, et al. Adjuvant 131I-metuximab for hepatocellular carcinoma after liver resection: a randomised, controlled, multicentre, open-label, phase 2 trial. Lancet Gastroenterol Hepatol. 2020;5(6):548-560.
4. Wang Z, Ren Z, Chen Y, et al. Adjuvant Transarterial Chemoembolization for HBV-Related Hepatocellular Carcinoma After Resection: A Randomized Controlled Study. Clin Cancer Res. 2018;24(9):2074-2081.
5. Hack SP, Spahn J, Chen M, et al. IMbrave 050: a Phase III trial of atezolizumab plus bevacizumab in high-risk hepatocellular carcinoma after curative resection or ablation. Future Oncol. 2020;16(15):975-989.
6. Ronot M, Chernyak V, Burgoyne A, et al. Imaging to Predict Prognosis in Hepatocellular Carcinoma: Current and Future Perspectives. Radiology. 2023:221429.
7. Lee S, Kang TW, Song KD, et al. Effect of Microvascular Invasion Risk on Early Recurrence of Hepatocellular Carcinoma After Surgery and Radiofrequency Ablation. Ann Surg. 2021;273(3):564-571.
8. Kudo M, Kawamura Y, Hasegawa K, et al. Management of Hepatocellular Carcinoma in Japan: JSH Consensus Statements and Recommendations 2021 Update. Liver Cancer. 2021;10(3):181-223.
Figures