0913
Predictive Model for Proliferative HCC Using LI-RADS v2018: Assessing Therapeutic Outcomes in Hepatectomy and Systemic Therapy1Nantong Third People's Hospital, Nantong, China, 2Philips Healthcare, Nantong, China
Synopsis
Keywords: Liver, Data Analysis
Motivation: Hepatocellular carcinoma (HCC) can be categorized into proliferative and non-proliferative classes, with proliferative HCC exhibiting aggressive characteristics and a poor prognosis.
Goal(s): To develop a predictive model for proliferative HCC using Liver Imaging Reporting and Data System (LI-RADS) and to investigate its prognostic value for HCC.
Approach: A logistic regression nomogram was constructed based on LI-RADS features to identify proliferative HCC. The implication of model-predicted proliferative HCC for different therapeutic outcomes in HCC was investigated.
Results: The predictive model for proliferative HCC performed well and is a risk factor for postoperative recurrence in HCC, associated with favorable outcomes in systemic therapy.
Impact: The MR-based model, utilizing LI-RADS v2018, could predict proliferative HCC before treatment. Patients with model-predicted proliferative HCC had more post-hepatectomy recurrences but better responses to systemic therapy, which may facilitate clinical decision-making for more precise and rational therapeutic strategies.
Introduction
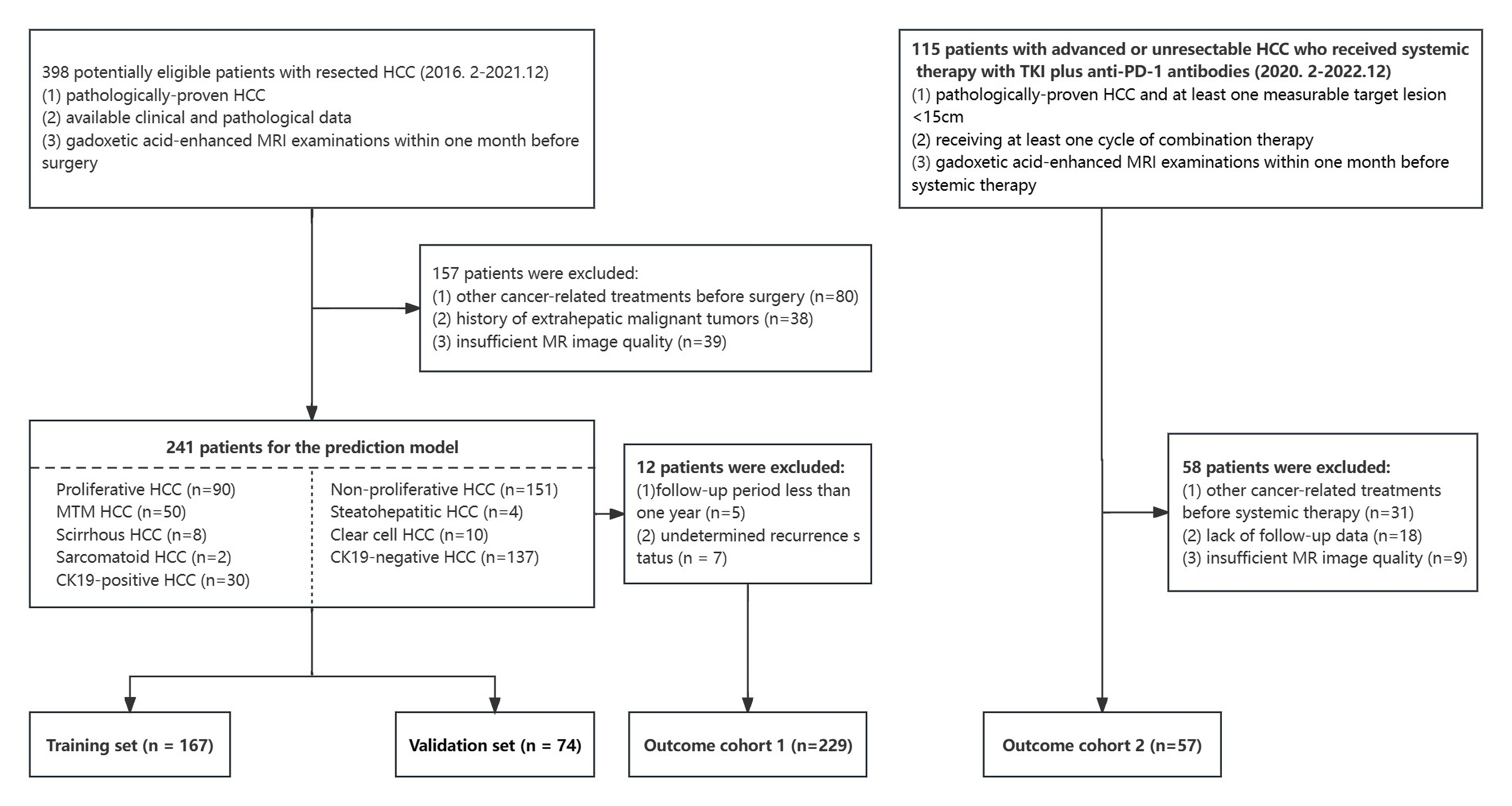
We aimed to develop a predictive model for proliferative hepatocellular carcinoma (HCC) using Liver Imaging Reporting and Data System (LI-RADS) v2018 and to investigate the potential value of the model in assessing therapeutic outcomes for hepatectomy and systemic therapy in HCC.Methods
241 HCC patients who underwent hepatectomy and 57 who received systemic therapy with combined anti-angiogenic tyrosine kinase inhibitors (TKIs) and anti-PD-1 antibodies were included, respectively. LI-RADS features were evaluated on pretreatment gadoxetic-enhanced MRI. A diagnostic nomogram was constructed based on LI-RADS to identify proliferative HCC and the model performance was tested in the validation set. The implication of model-predicted proliferative HCC for postoperative recurrence was investigated, and survivals in different groups were compared. Tumor response was assessed on MRI and the relationship between model-predicted proliferative HCC and objective response to combination therapy were explored.Results
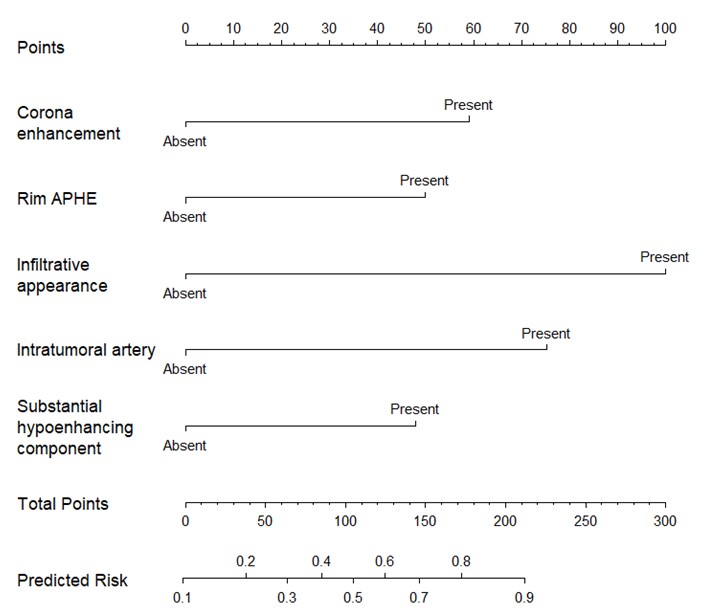
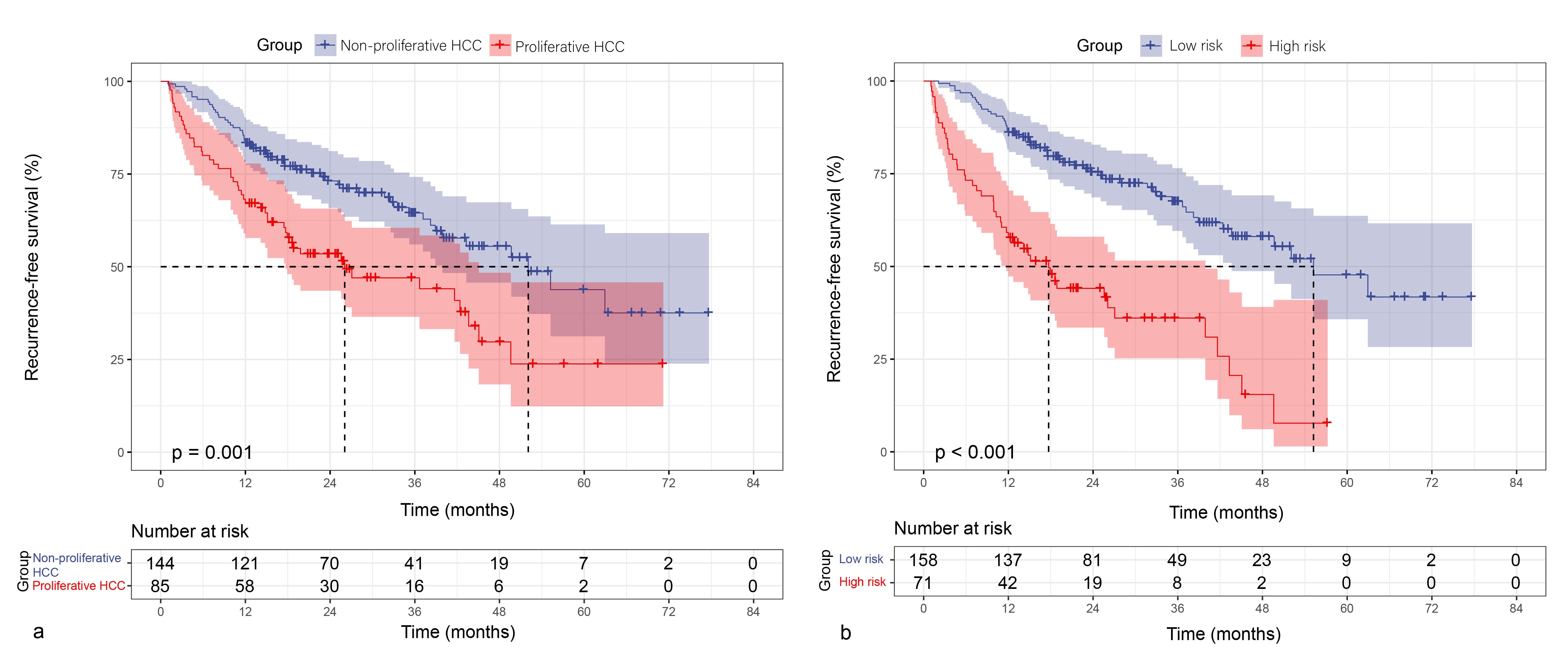
Corona enhancement (OR, 3.373; p = 0.006), rim arterial phase hyperenhancement (APHE) (OR, 2.787; p = 0.037), infiltrative appearance (OR, 7.818; p = 0.018), intratumoral artery (OR, 4.706; p = 0.001), and substantial hypoenhancing component (OR, 2.684; p = 0.033) are independent predictors of proliferative HCC. The model performed well with AUCs of 0.823 and 0.803 for the training and validation sets, respectively. High risk score (HR, 2.695; p < 0.001) for proliferative HCC was independent risk factor for recurrence-free survival (RFS) in HCCs after hepatectomy. Differences in RFS were significant between groups (high-risk vs. low-risk, p = 0.001; proliferative HCC vs. non-proliferative HCC, p < 0.001). Furthermore, patients who received systemic therapy exhibited a higher objective response rate and longer progression-free survival (PFS) in the high-risk group than the low-risk group (p < 0.001).Discussion
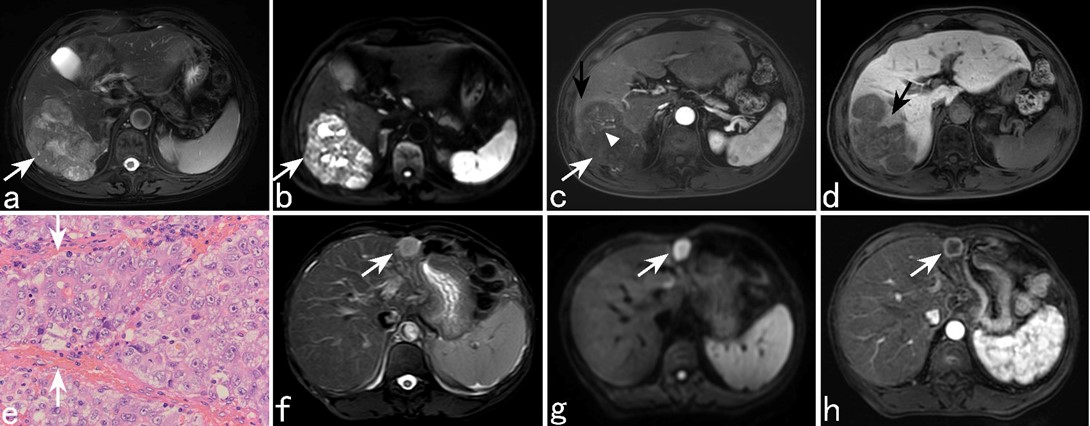
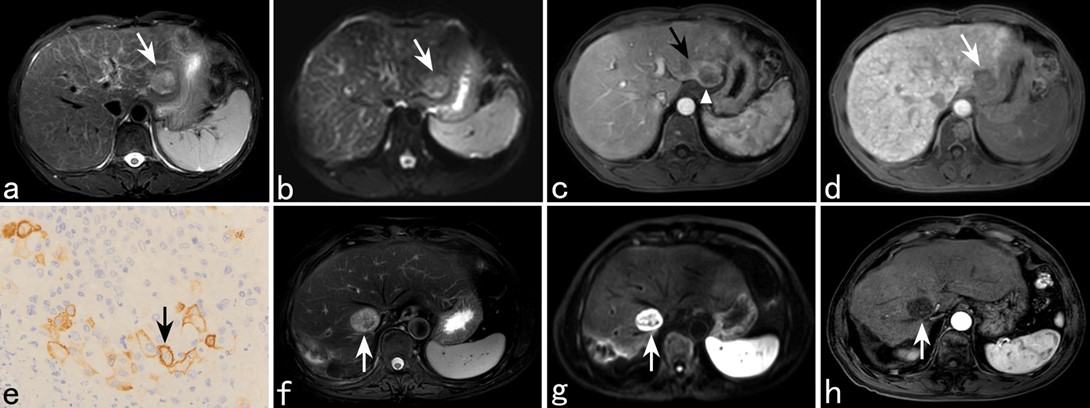
In the predictive model for proliferative HCC, rim APHE, corona enhancement, infiltrative appearance, intratumoral artery, and substantial hypoenhancing component were identified to be significant predictors. Subsequently, model-predicted proliferative HCC was identified as predictor for postoperative recurrence in HCC and had association with objective response to systemic therapy, thereby demonstrating the prognostic value of the model. Rim APHE, categorized as LR-M, has been frequently observed in HCCs with macrotrabecular massive (MTM) and cytokeratin-19 (CK19) positive subtypes1,2. This appearance may be attributed to central fibrous stroma or reduced internal microvascular density in tumor3. Corona enhancement may originate from tumor obstruction of the venules, leading to a preferential arterial supply or connection between the tumor sinusoids and hepatic sinusoids4. It is closely related to higher pathological grades and microvascular invasion5,6. Infiltrative appearance may reflect a permeative pathological growth pattern with infiltration of tumor cells into the liver parenchyma, which has strong relation with tumor invasion7 and recurrence8. And it can help predict CK19-positive HCC, a histopathological subtype of proliferative HCC9. Intratumoral artery is valuable for diagnosing MTM-HCC10 and the identification of VETC11, whereas VETC are enriched in most of MTM-HCCs12. In our study, MTM-HCCs comprised a relatively high proportion of proliferative HCCs. Substantial hypoenhancing component may be caused by a high proportion of fibrotic stroma or extensive tumor necrosis. Studies have identified it as a determinant factor for predicting MTM-HCC10,13, which consequently implies proliferative HCC. Proliferative HCC displays aggressive molecular features including the activation of some signaling pathways4, several targeted therapeutic agents can block these pathways to inhibit tumor development14-16. Non-invasive interventions are significant for HCC patients who couldn’t accept hepatectomy. In our study, patients with proliferative HCCs (pathologically-confirmed / model-predicted) showed higher rates of recurrence after hepatectomy but better responses to systemic therapy. Hence, identifying proliferative HCC prior to treatment may open up a new horizon for application of systemic therapy strategies including immunotherapy, targeted therapy and their combination treatment.Conclusion
The MR-based model, utilizing LI-RADS v2018, could predict proliferative HCC before treatment. Patients with model-predicted proliferative HCC demonstrated different survival outcomes following hepatectomy and systemic therapy. Such a model could be a valuable tool for clinicians to enable earlier diagnosis and more appropriate treatment.Acknowledgements
The study was approved by the ethics committee of the Affiliated Nantong Hospital 3 of Nantong University, and the requirement of informed consent was exempted.References
1. Choi SY, Kim SH, Park CK, et al (2018) Imaging Features of Gadoxetic Acid-enhanced and Diffusion-weighted MR Imaging for Identifying Cytokeratin 19-positive Hepatocellular Carcinoma: A Retrospective Observational Study. Radiology 286(3):897-908
2. Ziol M, Poté N, Amaddeo G, et al (2018) Macrotrabecular-massive hepatocellular carcinoma: A distinctive histological subtype with clinical relevance. Hepatology 68(1):103-112
3. Rhee H, An C, Kim HY, Yoo JE, Park YN, Kim MJ (2019) Hepatocellular carcinoma with irregular rim-like arterial phase hyperenhancement: more aggressive pathologic features. Liver Cancer 8(1):24–40
4. Fowler KJ, Burgoyne A, Fraum TJ, et al (2021) Pathologic, Molecular, and Prognostic Radiologic Features of Hepatocellular Carcinoma. Radiographics 41(6):1611-163
5. Lu M, Qu Q, Xu L, et al (2023) Prediction for Aggressiveness and Postoperative Recurrence of Hepatocellular Carcinoma Using Gadoxetic Acid-Enhanced Magnetic Resonance Imaging. Acad Radiol 30(5):841-852
6. Xu X, Zhang HL, Liu QP et al (2019) Radiomic analysis of contrastenhanced CT predicts microvascular invasion and outcome in hepatocellular carcinoma. J Hepatol 70(6):1133-1144
7. Vernuccio F, Porrello G, Cannella R, et al (2021) Benign and malignant mimickers of infiltrative hepatocellular carcinoma: Tips and tricks for differential diagnosis on CT and MRI. Clin Imaging 70:33-45
8. An C, Zuo M, Li W, Chen Q, Wu P (2021) Infiltrative hepatocellular carcinoma: Transcatheter arterial chemoembolization versus hepatic arterial infusion chemotherapy. Front Oncol 11:747496
9. Rhee H, Kim H, Park YN (2020) Clinico-radio-pathological and molecular features of hepatocellular carcinomas with keratin 19 expression. Liver Cancer 9(6):663-681
10. Cha H, Choi JY, Park YN, et al (2023) Comparison of imaging findings of macrotrabecular-massive hepatocellular carcinoma using CT and gadoxetic acid-enhanced MRI. Eur Radiol 33(2):1364-1377
11. Yang J, Dong X, Wang G, et al (2023) Preoperative MRI features for characterization of vessels encapsulating tumor clusters and microvascular invasion in hepatocellular carcinoma. Abdom Radiol (NY) 48(2):554-566
12. Renne SL, Woo HY, Allegra S, et al (2020) Vessels Encapsulating Tumor Clusters (VETC) Is a Powerful Predictor of Aggressive Hepatocellular Carcinoma. Hepatology 71(1):183-195
13. Rhee H, Cho ES, Nahm JH, et al (2021) Gadoxetic acid-enhanced MRI of macrotrabecular-massive hepatocellular carcinoma and its prognostic implications. J Hepatol 74(1):109-121
14. Wu Y, Zhang Y, Qin X, Geng H, Zuo D, Zhao Q (2020) PI3K/AKT/mTOR pathway-related long non-coding RNAs: roles and mechanisms in hepatocellular carcinoma. Pharmacol Res 160:105195
15. Moon H, Ro SW (2021) MAPK/ERK Signaling Pathway in Hepatocellular Carcinoma. Cancers (Basel) 13(12):3026
16. Chen J, Gingold JA, Su X (2019) Immunomodulatory TGF-β Signaling in Hepatocellular Carcinoma. Trends Mol Med 25(11):1010-1023
Figures