0910
Leveraging unprecedented ultra-high strength gradients in commercially available MRI for in-vivo diffusion tensor CMR1CMR Unit, The Royal Brompton Hospital, London, United Kingdom, 2National Heart and Lung Institute, Imperial College London, London, United Kingdom, 3MR Research Collaborations, Siemens Healthcare Limited, Camberley, United Kingdom, 4Cardiovascular MR Predevelopment, Siemens Healthcare GmbH, Erlangen, Germany
Synopsis
Keywords: Gradients, Diffusion Tensor Imaging, ultra high gradient strength; motion compensated spin echo;
Motivation: Spin echo diffusion tensor cardiovascular magnetic resonance (DT-CMR) suffers from low SNR and resolution due to the time-consuming motion-compensated encoding gradients required.
Goal(s): Shorten TEs for motion compensated spin echo (MCSE) DT-CMR techniques to improve SNR and allow higher spatial resolution using ultra-high strength whole body gradients (200mT/m) newly available in commercially available scanners.
Approach: We implemented second order MCSE and acquired data in healthy subjects at peak systole and end diastole with maximum gradient strength of 146mT/m.
Results: We demonstrate high quality MCSE DT-CMR data with reduced TEs and higher spatial resolution than on previously available scanners using similar protocols.
Impact: Increases in imaging efficiency in DT-CMR enabled by the use of ultra-high strength gradients on commercial MRI systems will deliver shorter scans and improvements in spatial resolution which are vital steps on the road to clinical translation of DT-CMR.
Background
Diffusion tensor CMR (DT-CMR) non-invasively interrogates the cardiac microstructure and its dynamics in vivo, providing a wealth microarchitectural information in health and disease[1]. However, DT-CMR acquisition techniques are hampered by the highly dynamic nature of the heart with the cardiac and respiratory cycles and the short T2 of myocardial tissue. Stimulated echo-acquisition mode (STEAM) methods provide robust DT-CMR measures in almost any cardiac phase, but are hampered by low SNR efficiency and therefore, spatial resolution[2]. Motion compensated spin echo (MCSE) acquisitions provide increased SNR efficiency, but the long diffusion encoding gradient waveforms result in long TEs, hampering the available SNR and maximum diffusion encoding strength, and leading to motion-induced signal loss[3,4]. Recently introduced commercially available scanners with ultrahigh strength gradient systems potentially allow for substantial shortening of the diffusion encoding waveforms of MCSE DT-CMR sequences. Here we present preliminary results investigating the utility of such systems in shortening TE in MCSE DT-CMR and facilitating improvements in spatial resolution.Methods
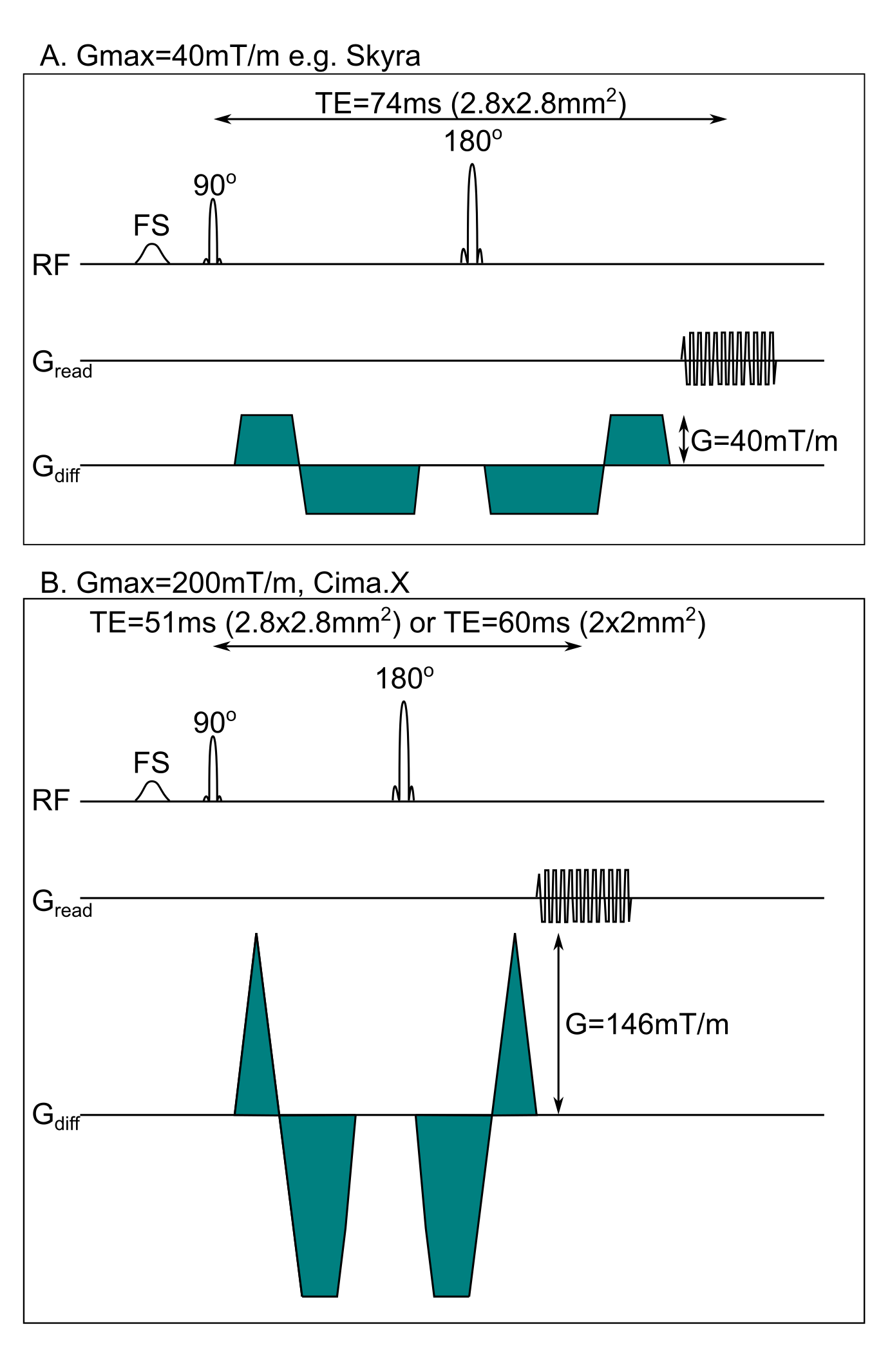
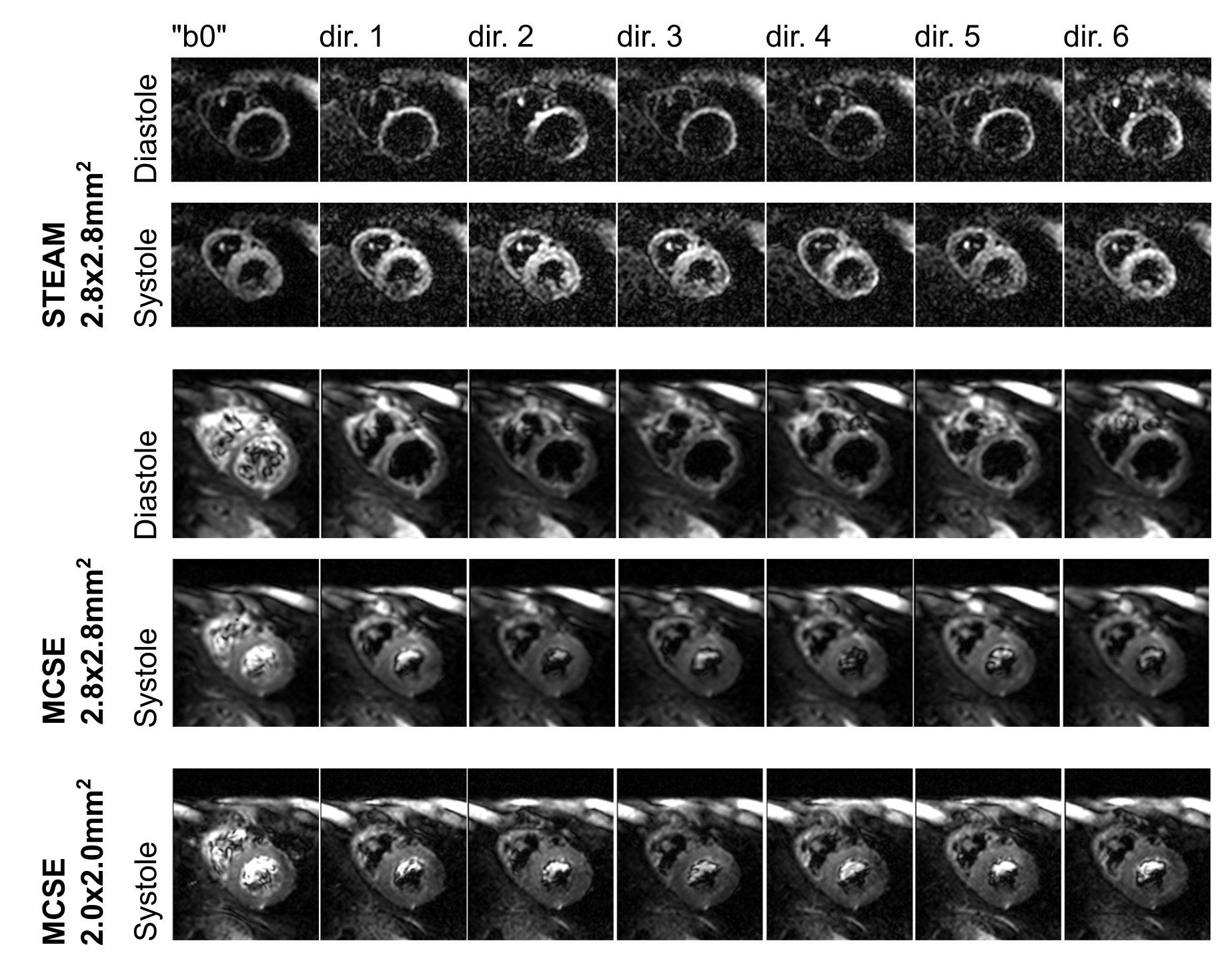
ECG-triggered second order MCSE (figure 1) and monopolar STEAM DT-CMR research sequences were implemented on a 3T scanner with maximum gradient strength 200mT/m and slew rate 200T/m/s (MAGNETOM Cima.X, Siemens Healthineers AG, Erlangen, Germany) with a single shot EPI readout. MCSE diffusion encoding gradient waveforms were based on those described by Welsh[5] and Stoeck[6].DT-CMR was performed in a single short axis mid-ventricular slice triggered to acquire the spin echo at peak systole and at diastolic pause. Acquisitions were performed during a breath hold of 18RR intervals including EPI phase correction, parallel imaging reference data, “b0” data and 6 diffusion encoding directions, with TR=2RR intervals. Data was acquired with 10 averages at the higher b-value (b=450smm-2 for MCSE and b=600smm-2 for STEAM) and 2 averages at b=150smm-2. SENSE acceleration factor 2 was used without partial Fourier. A reduced phase field of view was enabled by making the first (MCSE) or first and second (STEAM) RF pulses slice selective in the phase encode direction, resulting in a field of view of 360x135mm2. Acquired resolution was 2.8x2.8x8mm3 reconstructed to 1.4x1.4x8mm3. Chemical shift selective fat saturation was used. TE=51ms for MCSE and 24ms for STEAM. The systolic MCSE acquisition was repeated with acquired resolution 2.0x2.0x8mm3 reconstructed to 1.0x1.0x8mm3 and TE=60ms.
Results
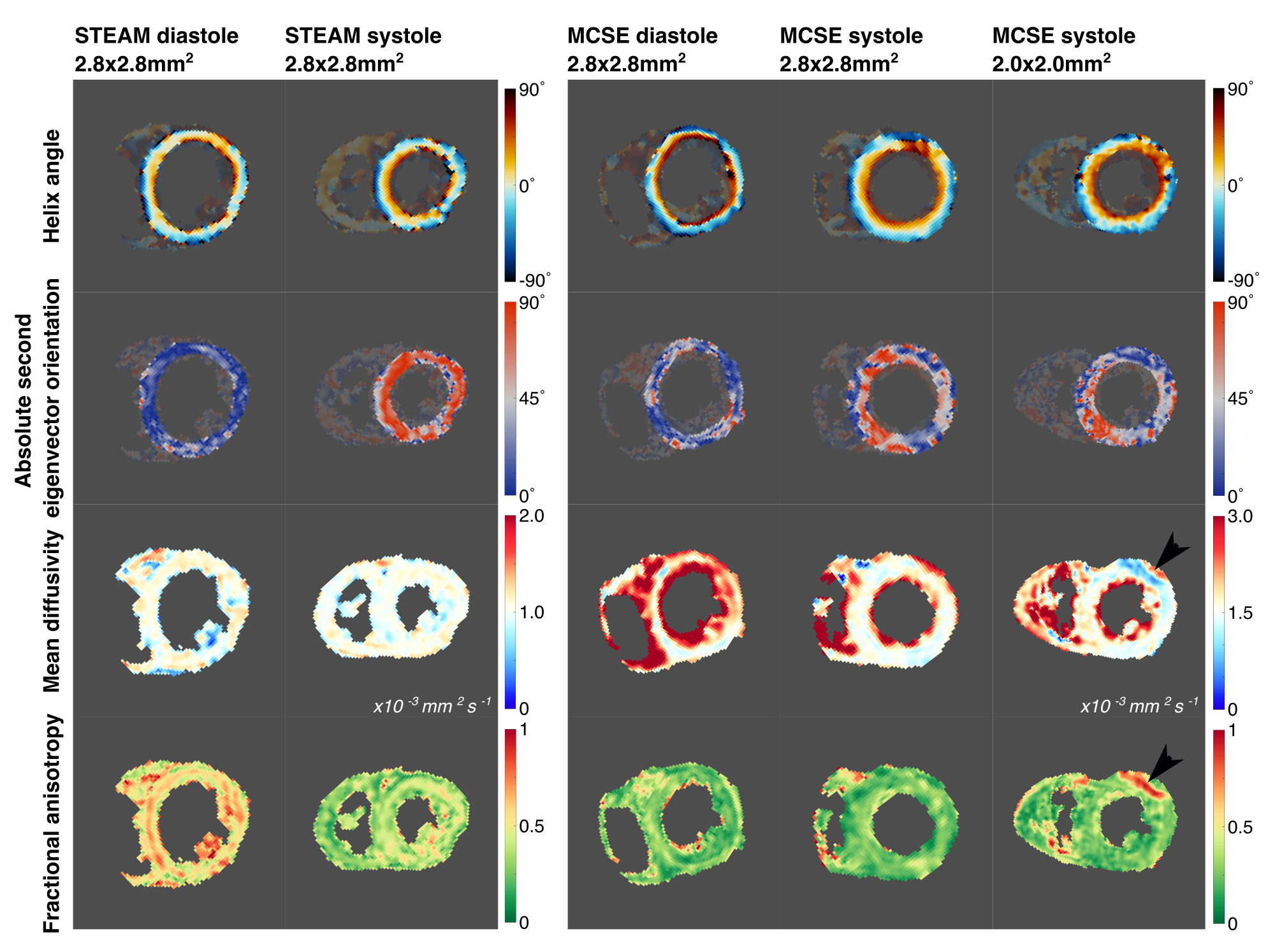
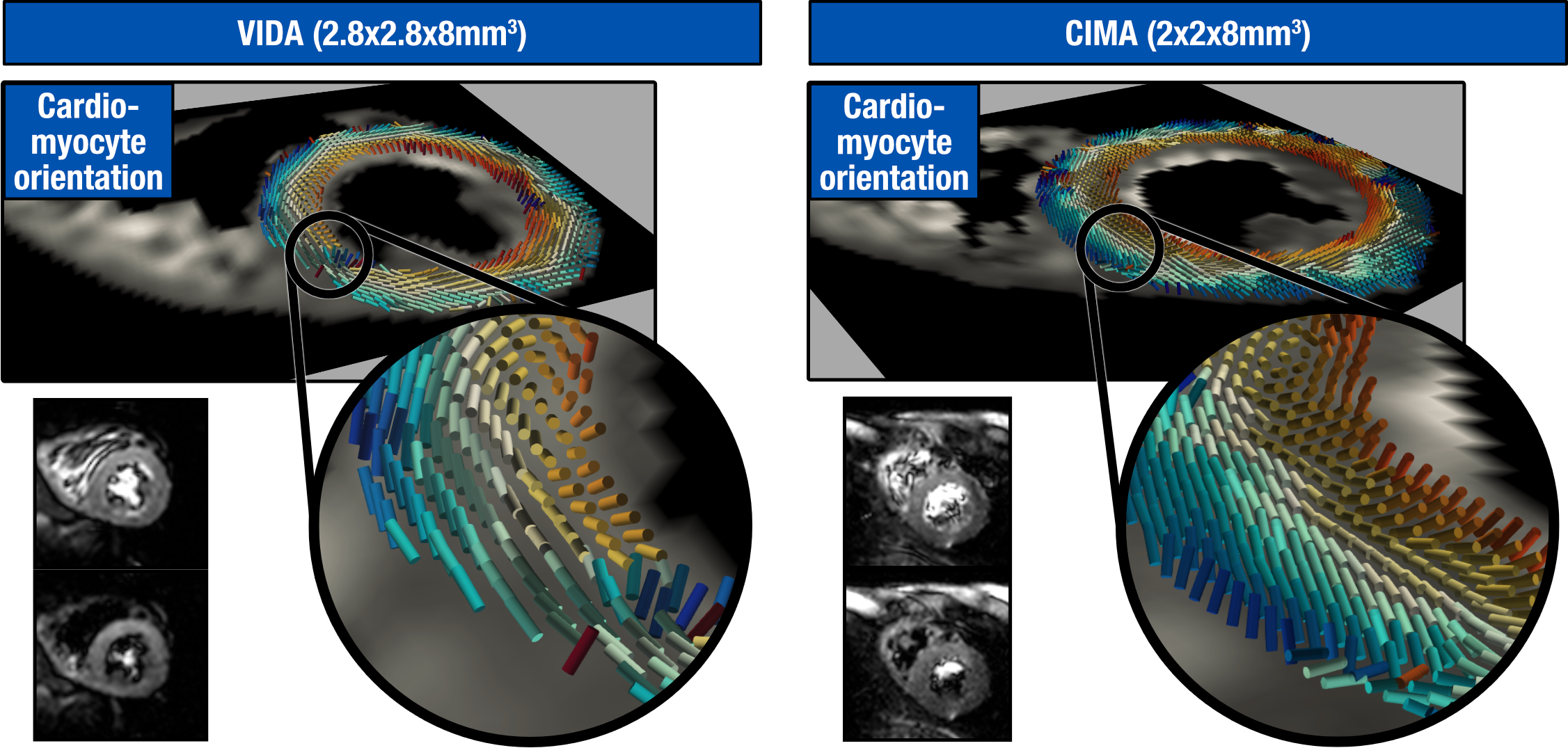
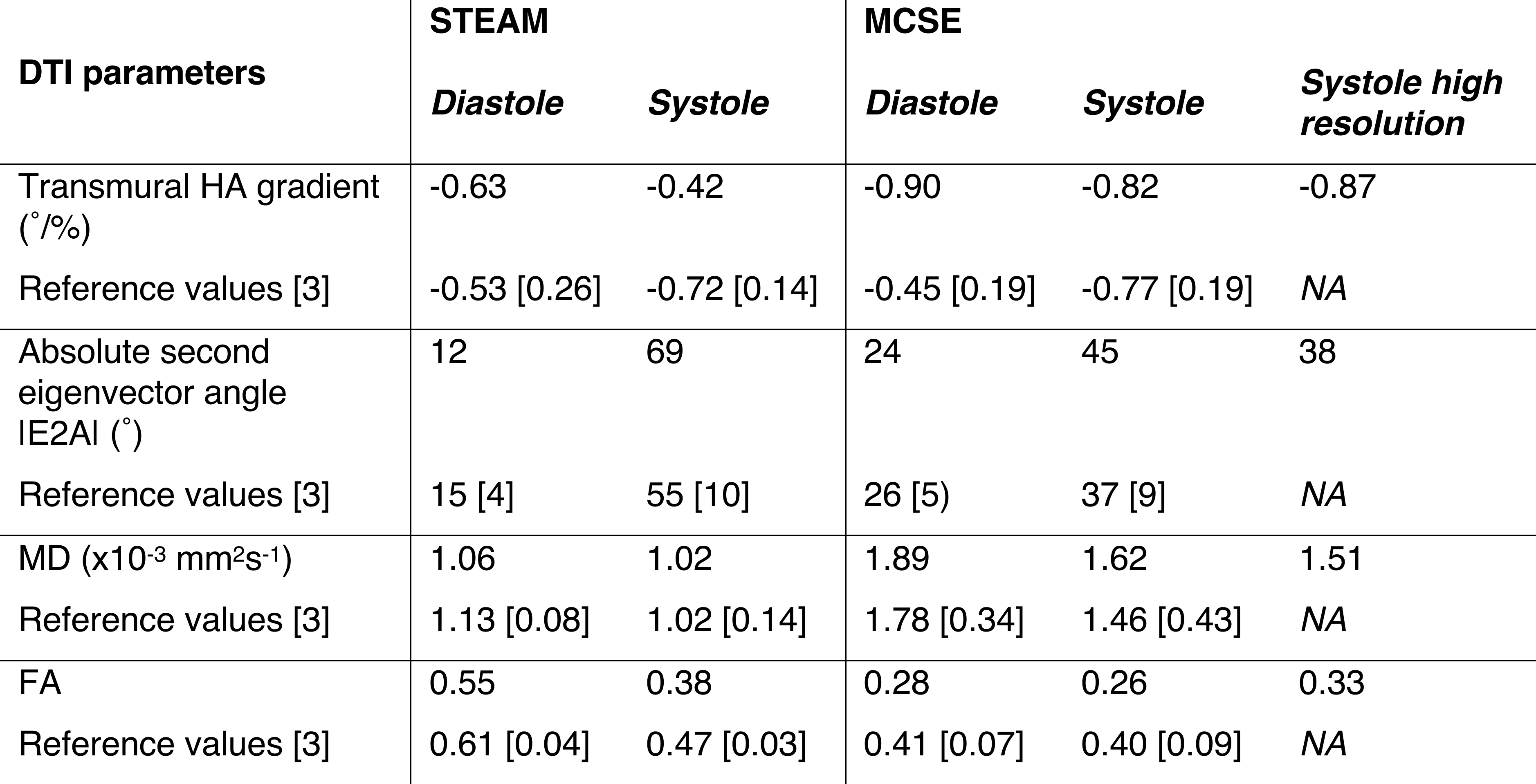
Acquisitions were performed in 4 healthy subjects and data is presented from subject 4 (male 33years ) after optimising the protocols in the first 3. Compared to typical TE=74ms for a matched protocol with a maximum gradient strength of 40mT/m (e.g. MAGNETOM Skyra , Siemens Healthineers AG, Erlangen, Germany), the reduction in TE to 51ms would result in a factor of 1.6 improvement in myocardial SNR (assuming T2=47ms[7]). Figure 2 demonstrates the image quality of the acquired diffusion weighted images and figure 3 shows DT-CMR parameter maps from each of the protocols. Figure 4 shows a rendering of the primary eigenvector of the MCSE data acquired at 2.0x2.0mm2, highlighting the amount of transmural data across the myocardium. Table 1 compares the results obtained to published literature values obtained with similar sequences[3], demonstrating compatible values in almost all parameters.Discussion and conclusion
Ultrahigh strength gradients allow a substantial reduction in TE for MCSE DT-CMR sequences which we have shown facilitates an increase in spatial resolution. The reduction in time required for the diffusion encoding waveforms may enable an increase in the robustness of MCSE sequences in diastole where they have been shown to frequently fail when used with more typical gradient systems[4,5]. It remains to be seen in future studies whether robust measures of sheetlet reorientation can be obtained from MCSE with ultrahigh gradient strengths, but they can be obtained using STEAM sequences[8]. The shortened diffusion encoding waveforms enabled by ultrahigh gradient strengths are expected to result in systematic changes in some DT-CMR parameters such as lower FA and higher MD (as observed) due to the reduced diffusion time which allows less time for diffusing particles to reach and interact with restrictions such as membranes[3].Some residual fat artefacts were present in the MCSE data (see figure 3), which are unrelated to the maximum diffusion encoding gradient strength and may be reduced in future studies with the use of binomial water selective excitation. Future studies may make further use of the maximum 200mT/m gradient strength by adopting unequal maximum amplitudes for the bipolar pulses used in the second order motion compensated encoding[5] or by using optimised non-trapezoidal gradient waveforms[9].
In conclusion, ultrahigh strength gradients available in commercial whole body MRI scanners facilitate reduced TEs in MCSE DT-CMR, potentially enabling increased spatial resolution and bringing translation of clinical DT-CMR one step closer.
Acknowledgements
This work was supported by British Heart Foundation Grant RG/19/1/34160 and by Siemens.References
1. Nielles-Vallespin S et al. JMRI 2020 doi: 10.1002/jmri.26912
2. Nielles-Vallesin S et al. MRM 2013 doi: 10.1002/mrm.24488
3. Scott AD et al. JCMR 2018 doi: 10.1186/s12968-017-0425-8
4. Moulin K et al. PLOS ONE 2020. doi: 10.1371/journal.pone.0241996
5. Welsh C et al. IEEE TMI 2015. doi: 10.1109/TMI.2015.2411571
6. Stoeck C et al. MRM 2016. doi: 10.1002/mrm.25784
7. Stanisz et al. MRM 2004. doi: 10.1002/mrm.20605
8. Nielles-Vallespin et al. JACC 2017 doi: 10.1016/j.jacc.2016.11.051
9. Afzali M et al. ISMRM 2023. Abstract 4284.
Figures