0903
Dynamic MRI in vivo investigation of abdominal hernia repair during standardized exercises1Laboratoire de Biomécanique Appliquée - UMRT24 Université Gustave Eiffel - Aix Marseille Université, Marseille, France, 2Department of General Surgery, Aix Marseille Univ, North Hospital, APHM, Marseille, France, 3CRMBM - UMR 7339 CNRS - Aix Marseille Université, Marseille Cedex 05, France
Synopsis
Keywords: Data Processing, Segmentation
Motivation: The incidence of abdominal hernia recurrence is reaching up to 45%; so the integration of biomechanical concepts into management could be helpful.
Goal(s): Few tools are currently available to assess the behaviour of the abdominal wall in vivo under physiological conditions.
Approach: Dynamic MRI was employed to obtain motion of the abdominal wall of patients before and after hernia surgery during a range of exercises. The areas of interest were segmented.
Results: Quantification of displacements and deformations in the abdominal muscles, hernia sac area, and inter-muscular distance demonstrate anatomical and functional changes in the abdominal wall post-hernia surgery.
Impact: A better understanding of the biomechanical behaviour of pathologic abdominal wall could be helpful to understand the mechanisms involved in the appearance and recurrence of hernias, thereby opening the way to more effective interventions for hernia patients.
Introduction
The abdominal wall is a complex multi-layered structure involved in maintaining and protecting the organs and regulating intra-abdominal pressure. Hernias can occur thereby resulting in a rupture into the abdominal strap, as represented figure 1-a. Surgery can be used to repair (figure 1-b) but the hernia recurrence rates is high 1, calling for surgical practices to be reconsidered and biomechanical concepts to be incorporated into management. A better understanding of the biomechanical behaviour of pathological abdominal wall could be helpful to understand the mechanisms involved in the appearance and recurrence of hernias. The objective of the present study was assessing the dynamics of abdominal wall in vivo during different physiological situations, using MRI combined to a dedicated segmentation and post-processing method.Methods
Dynamic (or 2D+t) 3-Tesla MRI (MAGNETOM Vida, Siemens Healthineers) allows visualizing in a 2D plane the movement of the abdominal wall in real-time. Axial images were acquired with cine bssfp sequences, with T1/T2 contrast (TE/TR: 1.19/2.72 ms, encoding phase direction : right-left, flip angle: 33°, slice thickness: 8 mm, GRAPPA 4 with 28 reference lines). The default field of view (360 × 360 mm2), resolution time (160ms) and pixel size (0.9 × 0.9 mm2) are adjustable to patient body size.At this stage, 3 patients have been included after providing their informed consent and one of them had both the pre and post-operative MRI. Patients were in supine position with a torso-dedicated 18 channels array coil, were asked to realize three audio-guided exercises, i.e. breathing, coughing and Valsalva maneuver.
MR images were acquired in the axial plane at a pre-determined level i.e. where the hernia neck (rupture location into the abdominal wall aponeurosis) was the largest. Approximately 10% of the images were manually segmented by an operator. Then, an algorithm was used to compute the segmentation masks over all the images 2,3 so as to label abdominal muscles (figure 1-c) . The hernia sac (internal content passing through the hernia neck, figure 1-d), the dorsal zone (figure 1-e) and the internal visceral area (figure 1-f) were also segmented.
Various metrics are computed to evaluate the abdominal wall dynamics. By considering a 2D cylindrical coordinate system, the radial displacement is assessed into the muscles (drawn on figure 2). This displacement, normalized by the radial distance at rest, is quantified for the rectus abdominis (RA) and lateral muscles (LM) 4, as drawn figure 2. Additionally, the distance between the two inner corners of the RA muscle (called RAM distance, in mm) was also assessed. Furthermore, the area of hernia sac (cm²) and the visceral area (figure 1-d and 1-f, respectively) are assessed. All the output metrics are scaled by the rest values.
Results
3.1 Pre-operative casesThe hernia sac area evolution over time, represented figure 3 for one participant, is greater during active exercises (cough and Valsalva) as compared to passive exercise (breathing). The muscular radial displacements within the LM and RA were quantified, being lower for LM during active exercises (figure 4). Both the visceral area and the abdominal wall perimeter were reduced during coughing and Valsalva, thereby leading to a compressed abdominal content.
3.2 Pre & post-operative case study
The preliminary results obtained in the patient scanned both before and after the hernia surgery indicated clear differences regarding RAM changes for the 3 exercise types, shortened of approximately 1 cm after surgery.
Discussion
The greater increase of hernia sac area during exercises engaging the muscles of the abdominal wall can be attributable to the higher intra-abdominal pressure created by this type of exercise 5.The orientation of muscular radial displacements accords with those outlined by Jourdan et al. in their study of healthy subjects 4. Furthermore, the reduction in RAM distance is primarily attributable to the closing of the hernia's neck. A RAM distance that is still large even after surgery can be a factor in hernia recurrence 6.
Conclusion
The biomechanical evaluation of the pathologic abdominal wall (herniated and repaired) was conducted using dynamic MRI. In a limited number of patients, our findings show that hernia sac area changes more in response to abdominal muscular activation. We also quantified the shortening of the distance between the rectus abdominis after surgery. To better comprehend the biomechanical alterations in pathological abdominal walls and the effects of surgery, the study is conducted in a larger number of subjects.Acknowledgements
No acknowledgement found.References
1. Romain B, Renard Y, Binquet C, et al. Recurrence after elective incisional hernia repair is more frequent than you think: An international prospective cohort from the French Society of Surgery. Surgery. 2020;168(1):125-134. doi:10.1016/j.surg.2020.02.016
2. Ogier A, Sdika M, Fouré A, Le Troter A, Bendahan D. Individual muscle segmentation in MR images: A 3D propagation through 2D non-linear registration approaches. In: 2017 39th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC). ; 2017:317-320. doi:10.1109/EMBC.2017.8036826
3. Jourdan A, Le Troter A, Daude P, et al. Semiautomatic quantification of abdominal wall muscles deformations based on dynamic MRI image registration. NMR Biomed. 2021;34(4):e4470. doi:10.1002/nbm.4470
4. Jourdan A, Rapacchi S, Guye M, Bendahan D, Masson C, Bège T. Dynamic-MRI quantification of abdominal wall motion and deformation during breathing and muscular contraction. Comput Methods Programs Biomed. 2022;217:106667. doi:10.1016/j.cmpb.2022.106667
5. Soucasse A, Jourdan A, Edin L, Gillion JF, Masson C, Bege T. A better understanding of daily life abdominal wall mechanical solicitation: Investigation of intra-abdominal pressure variations by intragastric wireless sensor in humans. Med Eng Phys. 2022;104:103813. doi:10.1016/j.medengphy.2022.103813
6. Burger JWA, Lange JF, Halm JA, Kleinrensink GJ, Jeekel H. Incisional Hernia: Early Complication of Abdominal Surgery. World J Surg. 2005;29(12):1608-1613. doi:10.1007/s00268-005-7929-3
Figures
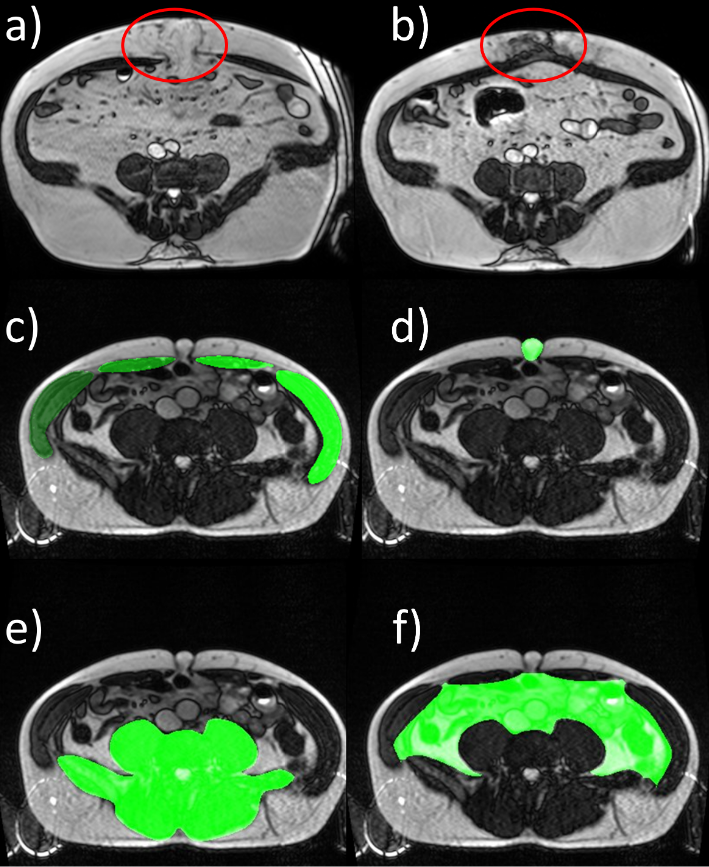
Figure 1 – MRI of the abdominal wall :
Pre (a) & post (b)-operative MRI in a patient, hernia sac and scar site are delineated.
c:f : Pre-operative MRIs in a patient
Abdominal muscles are delineated in c, the hernia sac in d, the dorsal zone in e and the visceral area in f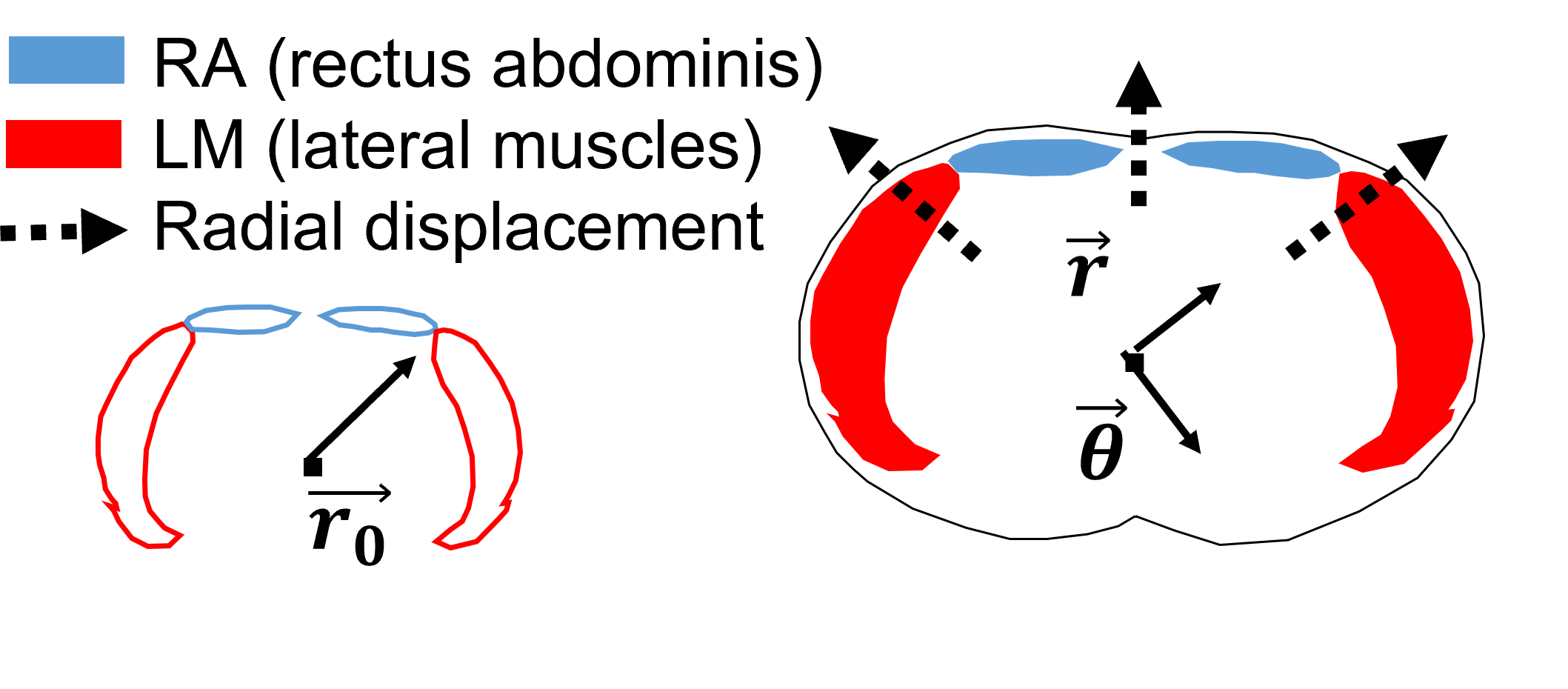
Figure 2 – Scheme of the abdominal wall muscles :
Rectus abdominis (RA) and lateral muscles (LM)
Cylindrical coordinate system and radial displacement direction
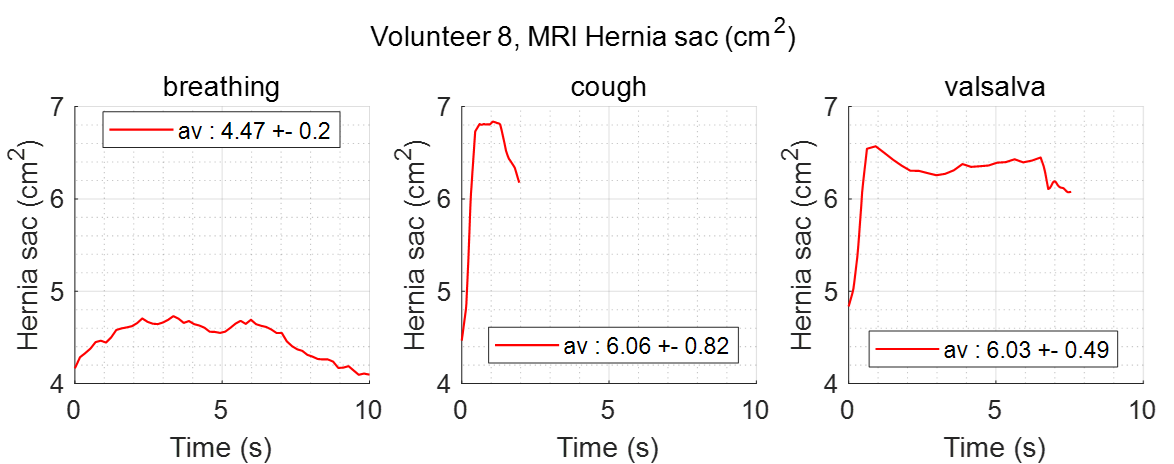
Figure 3 – Hernia sac area variation over time
During the three standardized exercises (breathing – cough – Valsalva)
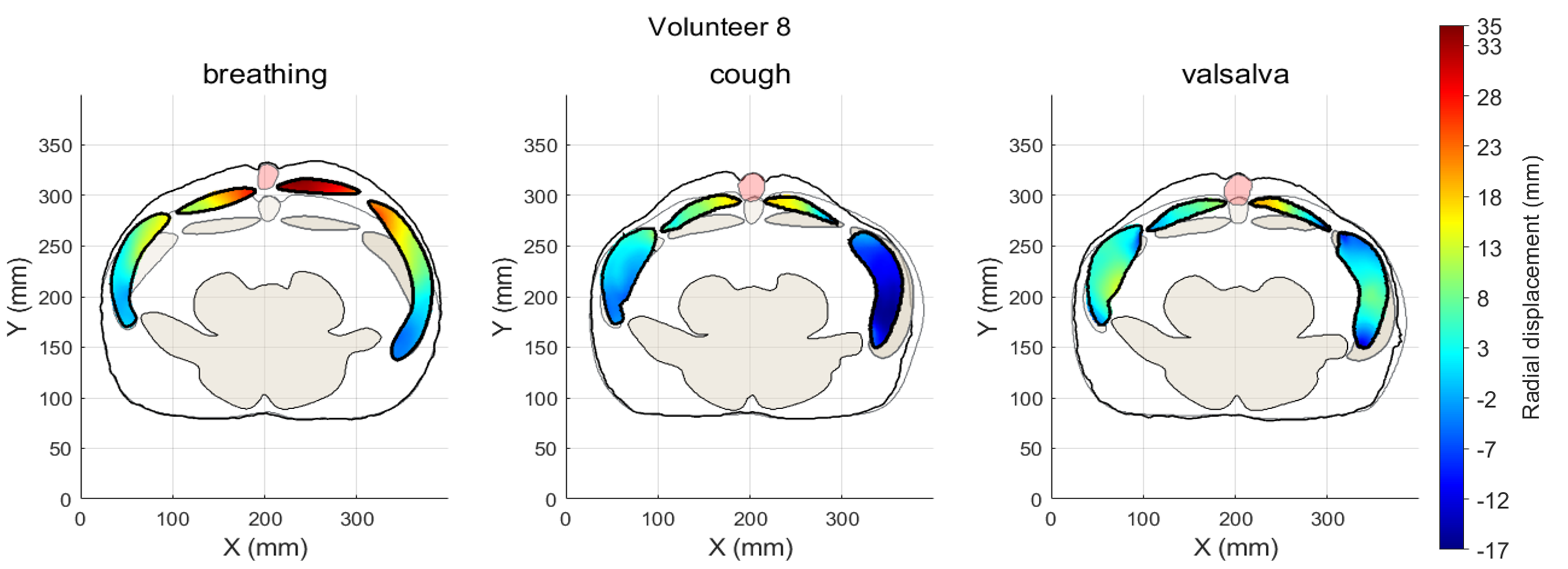
Figure 4 – Maximum radial displacement within muscle segmentation masks
During the three standardized exercises (breathing – cough – Valsalva)