0899
Unlocking Muscle Fatigue: Insights from Multi-Parametric 1H, 23Na & 31P MRI in Exercise-Induced Muscle Damage and Inflammation1Sport and Exercise Sciences, Manchester Metropolitan University, Manchester, United Kingdom
Synopsis
Keywords: Muscle, Spectroscopy, Muscle Inflammation, Integrative Physiology
Motivation: Exercise Induced Muscle Damage (EIMD) presents as a viable model to study the muscle inflammation and fatigue which may present across various age-related pathologies.
Goal(s): Our model presents as a useful tool to test therapies aimed at improved patient rehabilitation.
Approach: Here we use multi-parametric 31P, 23Na and 1H based MRI to show EMID is charactered by reduced muscle oxygenation with an increase in phosphate metabolism, sodium perturbation and overall perception of effort. Interestingly the cardiovascular response to exercise remained unchanged.
Results: Our results suggest a discrepancy between cardiovascular and muscle metabolic demand leads to altered oxygen delivery during exercise and increased fatigability.
Impact: This study highlights the importance of an integrative multi-parametric MRI approach to study the physiological consequences underlying muscle inflammation. This is crucial for advance our understanding on the abnormal responses present in age-related/health conditions characterised by muscle weakness and fatigue.
Introduction
Skeletal muscle type III-IV nerve afferents orchestrate the cardiovascular responses to exercise (1, 2), maintaining adequate blood flow and oxygen delivery to the exercising muscle (3). However, muscle nerve afferents function can be altered in disease states (4), and following inflammation induced by uncustomed exercise (i.e., exercise-induced muscle damage - EIMD) (5). While previous research has shown similar or attenuated cardiovascular responses before and after EIMD (6-9) none of these studies accounted for the confounding factors present following EIMD (i.e., changes in muscle oxygenation, metabolism, and weakness). Therefore, the aim of the present study was to investigate whether changes in muscle oxygenation and metabolism were associated with changes in cardiovascular responses to exercise and the muscle nerve afferents activity following EIMD. We hypothesised that changes in the muscle environment following EIMD alter the blood pressure response driven by muscle III-IV afferents. In turn, the ‘perception’ of effort (RPE) would increase during exercise.Methods
The local research ethics committee approved the study and 12 healthy males (age 25.2 ± 5.0 years) volunteered to take part and provided written, informed consent to participate. Assessments (questionnaire, MVC and MRI) were completed before and 48h after EIMD (Fig 1.). EIMD consisted of 40 min downhill running (DHR) at a 20% decline on a treadmill (H/P Cosmos Saturn 300/100). We recorded indicators of EIMD which included Maximal Voluntary Contraction (MVC), Soreness (VAS), and swelling measured from quadriceps cross-sectional area (Qcsa). All MRI measures used a SIEMENS MAGNETOM 3T Vida system. Participants were in a feet-first supine position with suitable RF coils placed over the thigh. 1H T2 mapping confirmed muscle inflammation post-EIMD. Muscle metabolism and oxygenation were measured at rest, during isometric knee extension and post-exercise cuff occlusion (PECO) with non-localized 31P NMR spectroscopy and Blood Oxygenation Level Dependent measures, respectively. The latter was preceded and followed by 23Na imaging to assess the ionic microenvironment of the muscle tissue (Fig 1). Measures of blood pressure (MAP) and heart rate (HR) were recorded throughout the MRI assessments with a non-invasive beat-by-beat device. All MRI-related outcomes were analysed offline in MATLAB 2020a (The MathWorks, Natick) using software routines developed in-house on the middle portion of the vastus lateralis muscle. A paired t-test was used to analyse outcomes of neuromuscular function and soreness while a two-way repeated measures ANOVA was implemented to analyse significant effects of time (pre- vs post-EIMD), phase (rest, exercise, PECO, recovery) and interaction. Statistical significance was set when p<0.05.Results
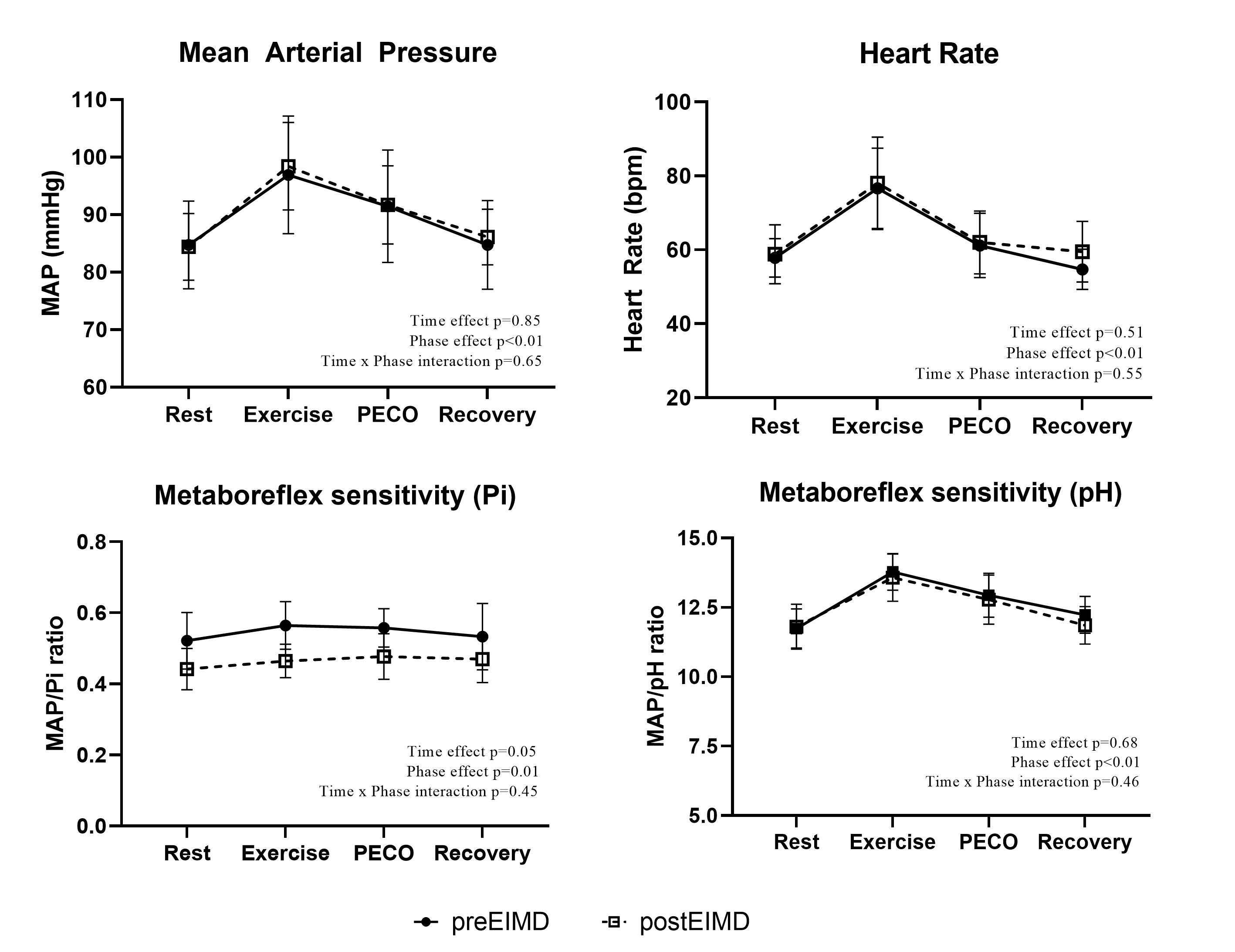
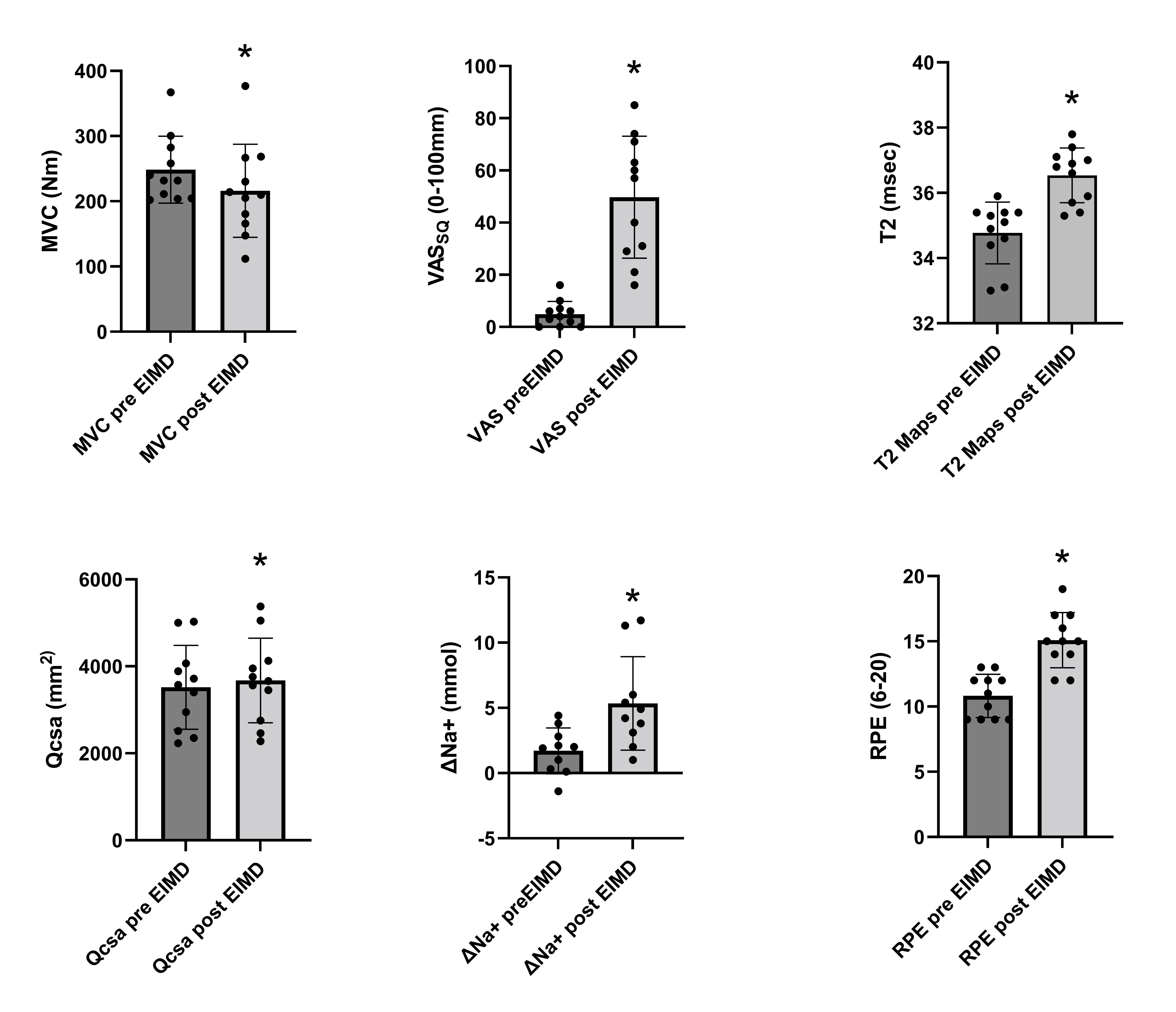
The downhill running protocol had a significant effect on neuromuscular function and soreness post-EIMD, showing a significant decrease in MVC torque (p<0.01) with an increase in Qcsa (p<0.01) and VASSQ (p<0.01). RPE during exercise increased post-EIMD (p<0.01), (Fig 2). Moreover, significant increases in muscle T2 were observed post-EIMD (p<0.01) confirming related tissue inflammation. Significant changes were found for [ΔNa+] from rest to post-sustained isometric contraction (p<0.01). BOLD measures confirmed that muscle oxygenation significantly decreased post-EIMD while 31P MRS showed significant increases in Pi/PCr, intracellular and extracellular Pi pre- to post-EIMD. Interestingly, no changes in ATPγ, PCr and pH from pre- to post-EIMD were observed (Fig 3). No changes were found in MAP and HR from pre- to post-EIMD. On the other hand, index of Metaboreflex sensitivity (Pi) changed significantly from pre- to post-EIMD, with no significant changes in Metaboreflex sensitivity for pH following EIMD (Fig 4).Discussion
In line with previous investigations, we found a considerable loss in muscle force and soreness after EIMD. This correlated with MRI T2 measures showing increased inflammation 48h later (10). Damaged muscles showed an elevated Pi/PCr ratio during rest, exercise, PECO, and recovery (11), as well as decreased oxygenation during occlusion (12) and increased RPE during exercise (13). Moreover, we found for the first time increases in delta sodium in damaged muscles that have been previously linked with muscle fatigability and weakness (14, 15). However, despite these peripheral perturbations, cardiovascular responses were unchanged from the non-damaged state. These results show possible interference on oxygen delivery and blood flow during exercise that may in turn increase the metabolic demand following EIMD, resulting in extensive reduction in muscle oxygenation and consequent increase in exercise effort and muscle fatigability.Conclusion
This study highlights the importance of an integrative multi-parametric MRI approach to study the physiological consequences underlying muscle inflammation following uncustomed exercise. This is crucial for advancing our understanding of the abnormal responses present in several medical conditions characterised by muscle weakness and fatigability. Our mechanistic study delivers an integrated protocol to track the impact of acute exercise bouts on recovery/rehabilitation in inflammatory conditions.Acknowledgements
No acknowledgement found.References
1. McCloskey DI, and Mitchell JH. Reflex cardiovascular and respiratory responses originating in exercising muscle. The Journal of Physiology 224: 173-186, 1972.
2. Goodwin GM, McCloskey DI, and Mitchell JH. Cardiovascular and respiratory responses to changes in central command during isometric exercise at constant muscle tension. The Journal of Physiology 226: 173-190, 1972.
3. Amann M, Runnels S, Morgan DE, Trinity JD, Fjeldstad AS, Wray DW, Reese VR, and Richardson RS. On the contribution of group III and IV muscle afferents to the circulatory response to rhythmic exercise in humans. J Physiol 589: 3855-3866, 2011.
4. Vianna LC, and Fisher JP. Reflex control of the cardiovascular system during exercise in disease. Current Opinion in Physiology 10: 110-117, 2019.
5. Zambolin F, Giuriato G, Laginestra FG, Ottaviani MM, Favaretto T, Calabria E, Duro-Ocana P, Bagley L, Faisal A, Peçanha T, McPhee JS, and Venturelli M. Effects of nociceptive and mechanosensitive afferents sensitization on central and peripheral hemodynamics following exercise-induced muscle damage. Journal of Applied Physiology 133: 945-958, 2022.
6. Ray CA, Mahoney ET, and Hume KM. Exercise-induced muscle injury augments forearm vascular resistance during leg exercise. Am J Physiol 275: H443-447, 1998.
7. Miles MP, Li Y, Rinard JP, Clarkson PM, and Williamson JW. Eccentric exercise augments the cardiovascular response to static exercise. Med Sci Sports Exerc 29: 457-466, 1997.
8. Lee JB, Katerberg C, Bommarito J, Power GA, and Millar PJ. Blood Pressure Responses to Post-Exercise Circulatory Occlusion Are Attenuated Following Exercise-Induced Muscle Weakness. Med Sci Sports Exerc 2023.
9. Zambolin F, Peçanha T, Pinner S, Venturelli M, and McPhee JS. Effects of exercise induced muscle damage on cardiovascular responses to isometric muscle contractions and post-exercise circulatory occlusion. European Journal of Applied Physiology 2023.
10. Bontemps B, Vercruyssen F, Gruet M, and Louis J. Downhill Running: What Are The Effects and How Can We Adapt? A Narrative Review. Sports Medicine 50: 2083-2110, 2020.
11. Davies RC, Eston RG, Fulford J, Rowlands AV, and Jones AM. Muscle damage alters the metabolic response to dynamic exercise in humans: a 31P-MRS study. J Appl Physiol (1985) 111: 782-790, 2011.
12. Larsen RG, Thomsen JM, Hirata RP, Steffensen R, Poulsen ER, Frøkjaer JB, and Graven-Nielsen T. Impaired microvascular reactivity after eccentric muscle contractions is not restored by acute ingestion of antioxidants or dietary nitrate. Physiol Rep 7: e14162, 2019.
13. Clarkson PM, and Newham DJ. Associations Between Muscle Soreness, Damage, and Fatigue. In: Fatigue: Neural and Muscular Mechanisms, edited by Gandevia SC, Enoka RM, McComas AJ, Stuart DG, Thomas CK, and Pierce PA. Boston, MA: Springer US, 1995, p. 457-469.
14. Gast LV, Baier LM, Meixner CR, Chaudry O, Engelke K, Uder M, Nagel AM, and Heiss R. MRI of Potassium and Sodium Enables Comprehensive Analysis of Ion Perturbations in Skeletal Muscle Tissue After Eccentric Exercise. Invest Radiol 58: 265-272, 2023.
15. Höger SA, Gast LV, Marty B, Hotfiel T, Bickelhaupt S, Uder M, Heiss R, and Nagel AM. Sodium and quantitative hydrogen parameter changes in muscle tissue after eccentric exercise and in delayed-onset muscle soreness assessed with magnetic resonance imaging. NMR in Biomedicine 36: e4840, 2023.
Figures
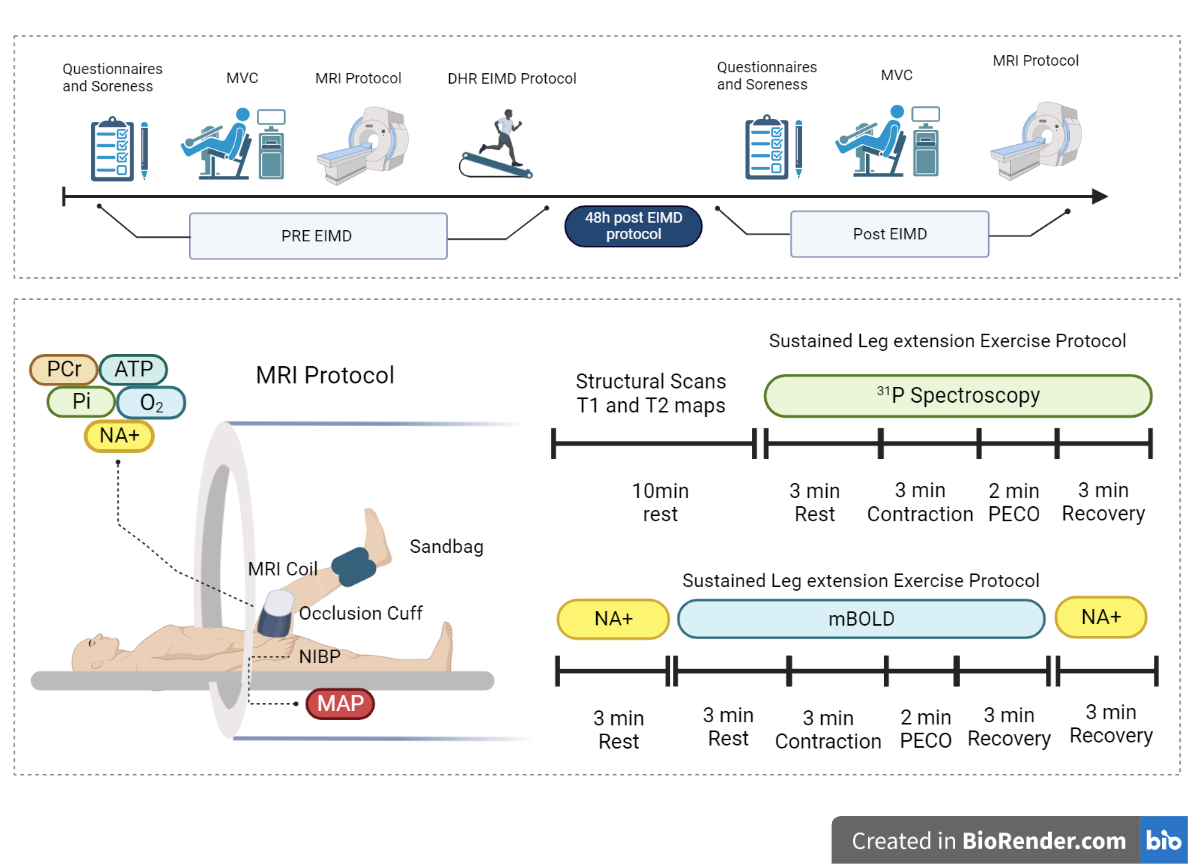
Design and timeline of the study and MRI protocol sequences. Participants underwent a preliminary questionnaire and soreness assessment followed by maximum voluntary contraction (MVC) and MRI. Thereafter, participants performed the downhill running (DHR). Two days later participants presented in the lab and performed all baseline assessments. Multi-parametric MRI assessment was composed of structural scans (T1 and T2) sequences and recording 31P, 23NA, and muscle oxygenation (mBOLD) during exercise and muscle occlusion (PECO). Created with BioRender.com
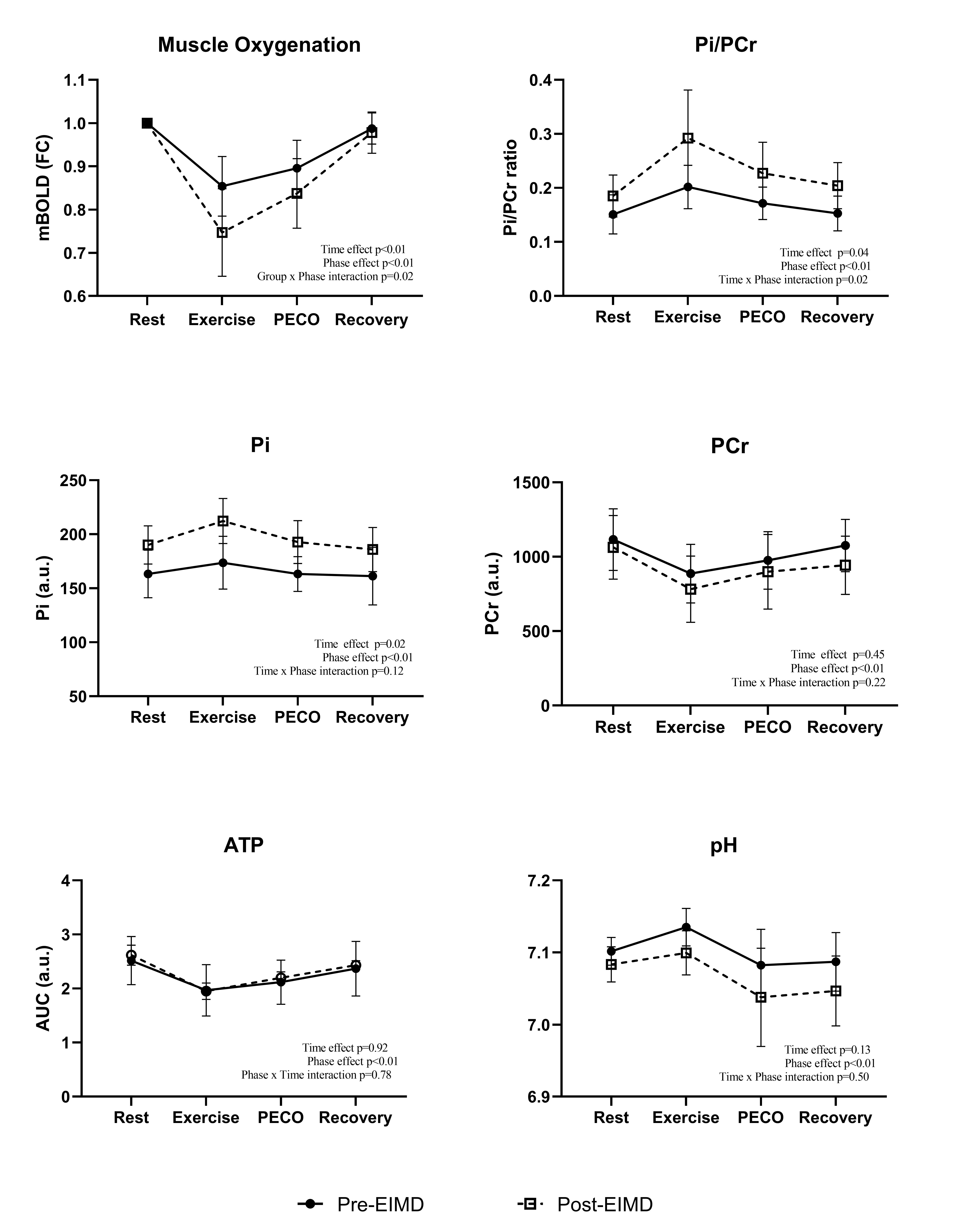
Changes in muscle metabolism and oxygenation before and 48h after EIMD. On the bottom right of each graph is reported the results from the statistical analysis and its respective p values. Data are presented as mean ± SD.