0882
Hepatobiliary Phase Synthesis Using Multi-Task Learning GAN: Application to Liver Fibrosis Classification1Institute of Science and Technology for Brain-Inspired Intelligence, Fudan University, Shanghai, China, 2Department of Radiology, Shanghai Public Health Clinical Center, Shanghai, China, 3USC Viterbi School of Engineering, University of Southern California, Los Angeles, CA, United States, 4Department of Biomedical Engineering, The Chinese University of Hong Kong, Shatin, Hong Kong, 5Philips Healthcare, Shanghai, China, 6Siemens Healthineers, Shanghai, China, 7Human Phenome Institute, Fudan University, Shanghai, China
Synopsis
Keywords: AI/ML Image Reconstruction, Liver
Motivation: Hepatobiliary phase (HBP) has important clinical diagnostic value for liver diseases, but its long acquisition time can pose issues with scanning resources and patient cooperation.
Goal(s): Our goal was to design a generative model for HBP synthesis based on early phases in hepatobiliary-specific contrast-enhanced MRI.
Approach: We proposed a multi-task learning deep learning model and evaluated its performance on a multi-center dataset.
Results: The proposed model exhibited superior HBP synthesis performance compared to the classic Pix2Pix model. The synthetic HBP was comparable to the real HBP, and significantly outperformed early phases in subsequent liver fibrosis grading tasks.
Impact: The proposed approach has the potential to accurately synthesize HBP, which is expected to be extended to clinical practice for rapid acquisition of HBP in hepatobiliary-specific contrast-enhanced MRI, thereby significantly reducing scanning time and alleviating clinical stress.
Introduction
Hepatobiliary phase (HBP) in hepatobiliary-specific contrast-enhanced MRI has important clinical diagnostic value for liver function (1), liver fibrosis (2) and liver lesions (3). However, HBP acquisition needs to wait until nearly 20 min after contrast injection, which creates a serious burden on scanning resources, and decreases patient cooperation leading to breathing and movement artifacts. In contrast, early enhanced phases (arterial, portal venous, delayed phases) can be acquired within 5 min. Our study aimed to develop a multi-task learning generative adversarial network (GAN) model to realize HBP synthesis based on early enhanced phases, which has rarely been addressed in previous research.Methods
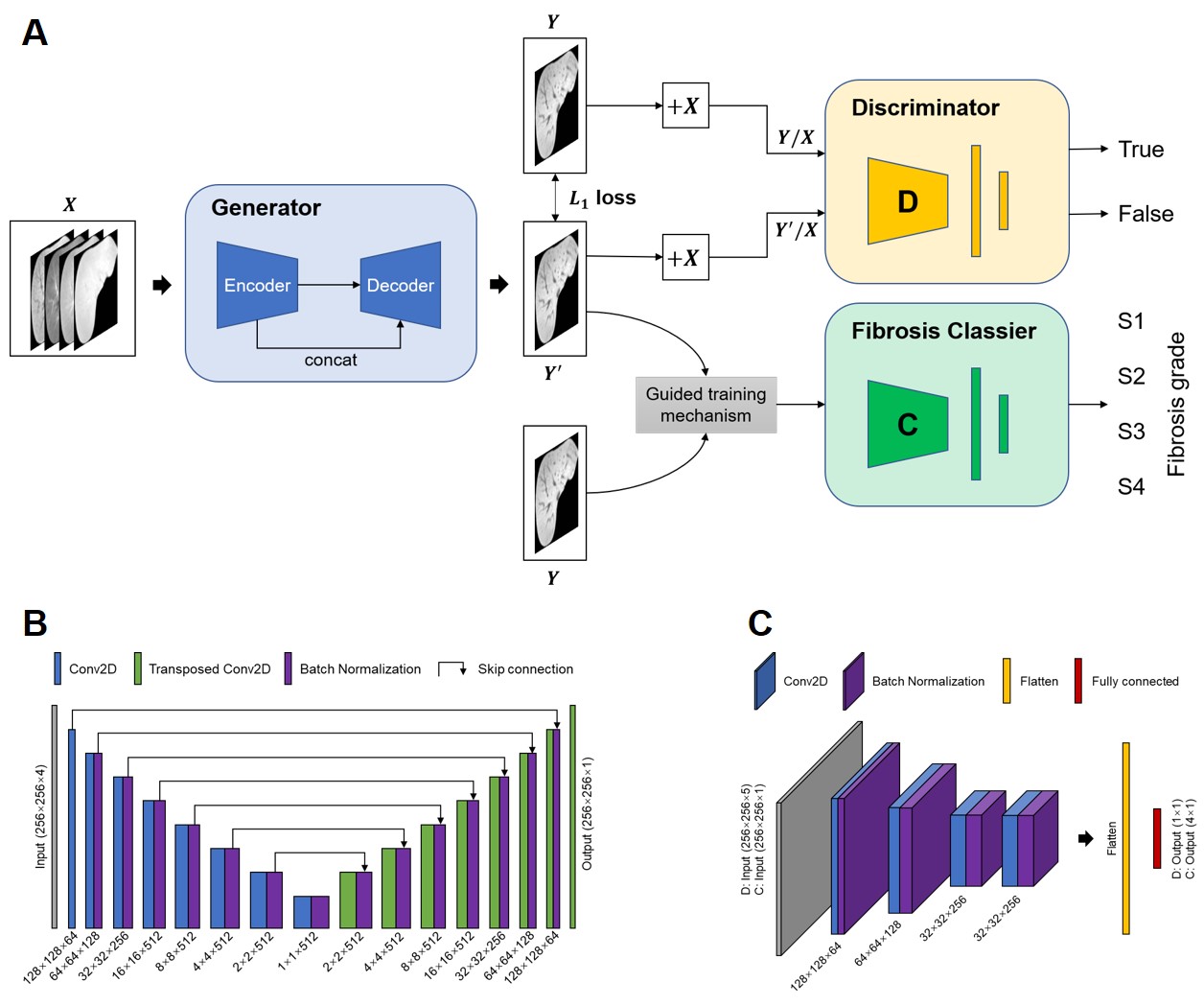
This retrospective study included totally 427 pathologically confirmed liver fibrosis patients (mean age ± SD, 48.8 years ± 13.1; 117 females) who underwent abdominal dynamic contrast-enhanced magnetic resonance imaging (DCE-MRI) using hepatobiliary-specific contrast agent gadolinium ethoxybenzyl diethylenetriamine pentaacetic acid (Gd-EOB-DTPA) from two clinical sites (internal dataset, Philips scanner, 165 cases for model development, 74 cases for internal evaluation; external dataset, Siemens scanner, 116 cases for model fine-tuning, 72 cases for external evaluation). The arterial, portal venous, delayed, and hepatobiliary phases were acquired at 20-25 s, 60-70 s, 120 s, and 20 min after contrast agent injection.We proposed a tripartite network structure containing generator (G), discriminator (D), and liver fibrosis classifier (F) branches for multi-task learning. The F branch implicitly introduced more texture constraints into the model (called Fib-GAN model), as fibrosis grade is highly correlated with liver texture (4-6). Moreover, to mitigate the instability of multi-task learning, we introduced a guided training mechanism (called GMFib-GAN model). Specifically, real and synthetic HBPs were jointly fed into the fibrosis classifier for training. The incorporation of real HBP could guide the classifier to better capture essential texture information, particularly in early training stage. The overall framework of the GMFib-GAN model is shown in Figure 1, and the loss functions are as follows:
$$Loss_{G}\left(X,Y,Y_{fib}\right)=L_{BCE}\left(D\left(concat\left(G\left(X\right),Y\right)\right),1\right)+\lambda_{1}L_{1}\left(G\left(X\right),Y\right)+\lambda_{2}\left(L_{CE}\left(F\left(Y\right),Y_{fib}\right)+L_{CE}\left(F\left(G\left(X\right)\right),Y_{fib}\right)\right)$$
$$Loss_{D}\left(X,Y\right)=L_{BCE}\left(D\left(concat\left(Y,X\right)\right),1\right)+L_{BCE}\left(D\left(concat\left(G\left(X\right),X\right)\right),0\right)$$
$$Loss_{F}\left(X,Y,Y_{fib}\right)=L_{CE}\left(F\left(Y\right),Y_{fib}\right)+L_{CE}\left(F\left(G\left(X\right)\right),Y_{fib}\right)$$
where X represents early DCE phases, as the multichannel input of the generator, Y is the real HBP, and Yfib is the fibrosis grade label. Moreover, concate signifies channel concatenation, λ1 and λ2 are hyperparameters to adjust the loss weights, which were set to 100 and 1 respectively. L1, LBCE and LCE denote absolute error loss, binary cross-entropy loss and cross-entropy loss.
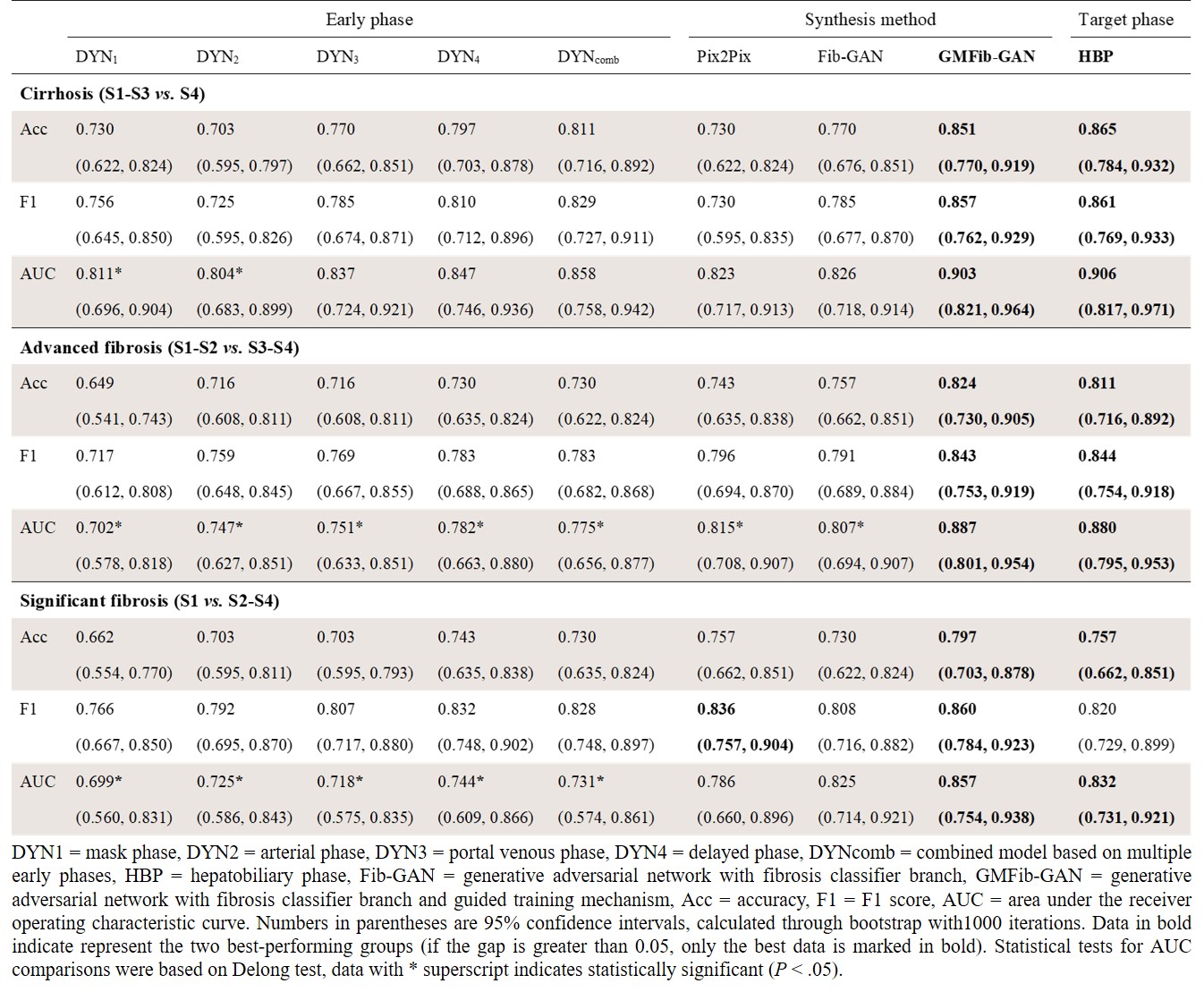
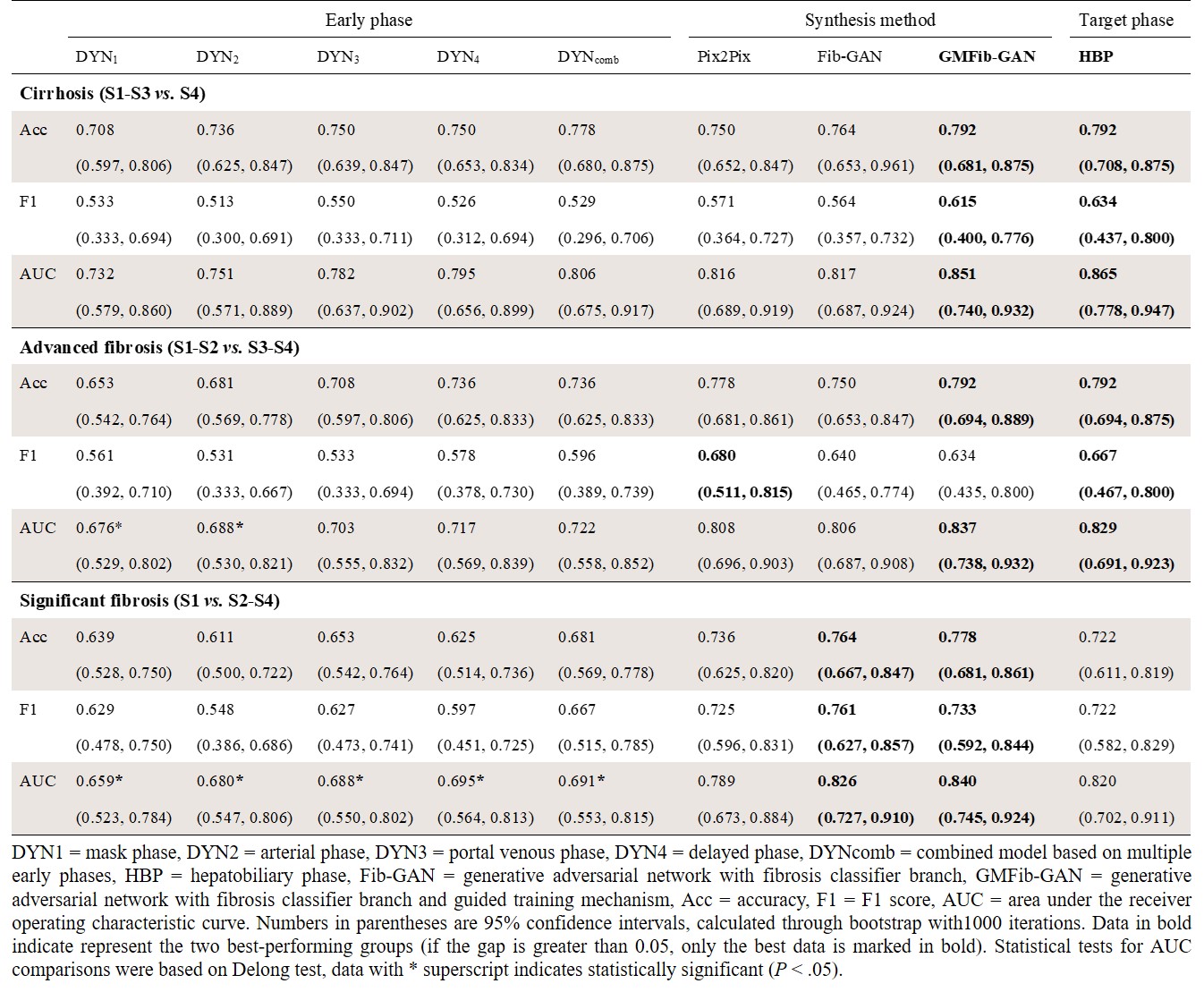
For fairness, we uniformly adopted standardized radiomics analysis method to compare the liver fibrosis grading performance of various phases. According to the Scheuer–Ludwig scoring system (7), fibrosis grades were categorized into S1-S4, and were constructed into three binary classification tasks in this study. Model evaluation included the quality assessment of synthetic HBP, using peak signal-to-noise ratio (PSNR) and structural similarity (SSIM); and performance assessment of fibrosis classification, using accuracy, F1 score, and area under the receiver operating characteristic curve (AUC). Paired Student’s t-tests and DeLong tests were performed to compare image quality metrics and AUCs.
Results
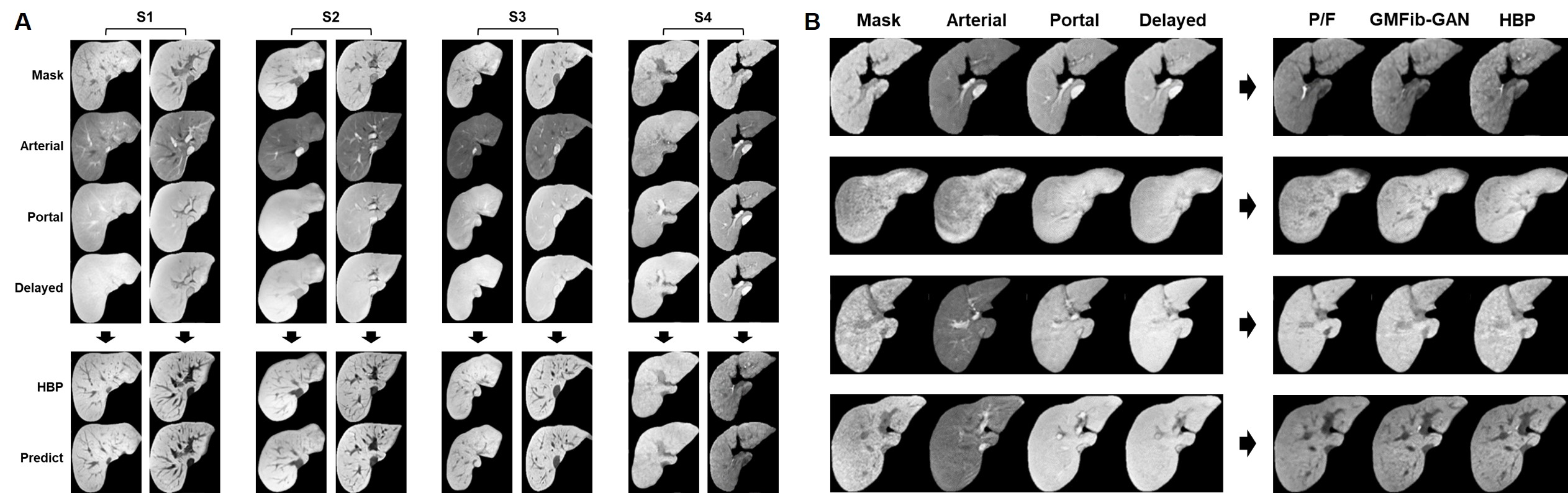
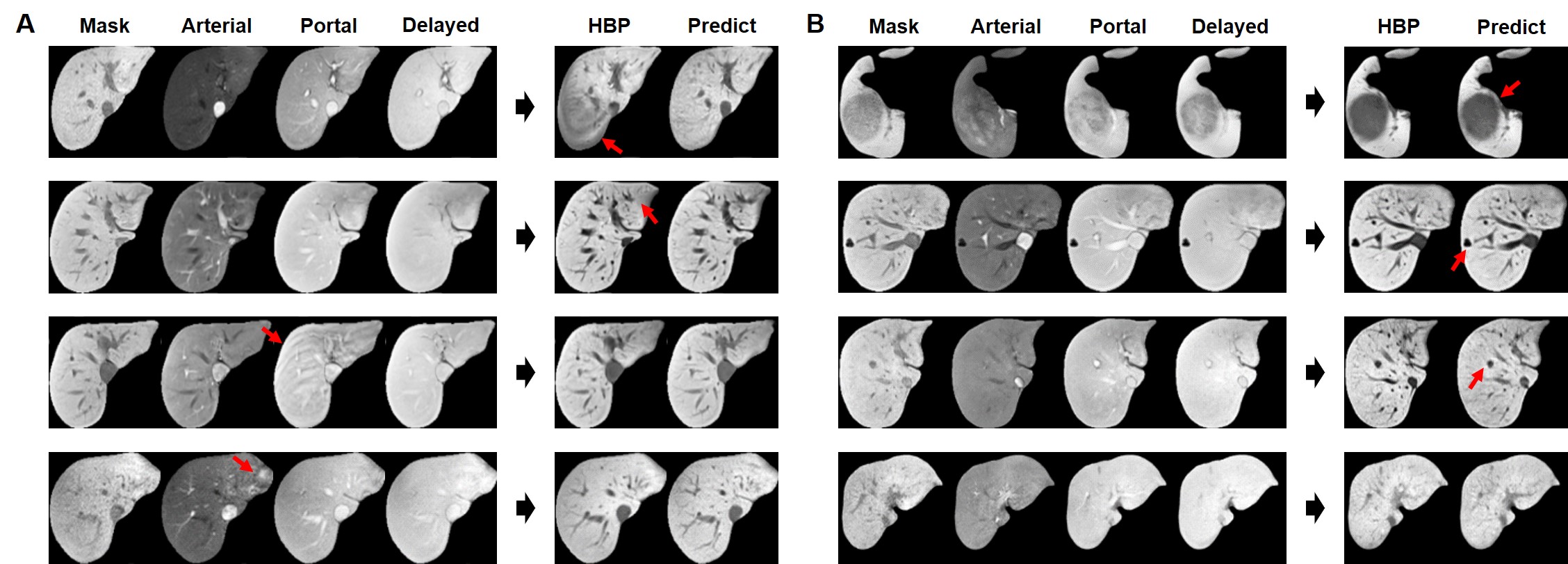
The proposed model achieved PSNRs of 25.52 and 25.06, SSIMs of 0.86 and 0.82 in the internal and external test sets respectively, which significantly outperformed the Pix2Pix model (8) (P < .01). Some representative synthesis results of the GMFib-GAN model, as well as comparisons with the Fib-GAN and Pix2Pix models are shown in Figure 2. Moreover, the effect of HBP synthesis under interference or in the presence of various liver lesions was further explored in Figure 3. In liver fibrosis grading, the synthetic HBP from GMFib-GAN model achieved AUCs of 0.86-0.90 and 0.84-0.85 internally and externally, which was comparable to the real HBP (P > .75 for most comparisons), and outperformed early phases as well as combined model (P < .05 for most comparisons). Specific performance metrics are listed in Tables 1 and 2.Discussion
The results demonstrated the superior performance of the proposed model in HBP synthesis, which provided benefits for downstream liver fibrosis grading tasks. Limited studies have focused on the synthesis effect of liver texture, we achieved better liver texture recovery through multi-task learning and a guided training mechanism. The synthetic HBP appeared rougher texture as the degree of liver fibrosis increased, consistent with the pathological process (4-6). Moreover, the proposed model exhibited robust anti-interference capability, and the synthesized liver lesions generally met the diagnostic requirements, enhancing the clinical usability of this study.Conclusion
This study proposed a multi-task learning GAN model for accurate synthesis of HBP in hepatobiliary-specific contrast-enhanced MRI, which is expected to be extended to clinical practice for rapid acquisition of HBP, thereby reducing scanning time and alleviating clinical stress.Acknowledgements
This work was supported by the National Natural Science Foundation of China (No. 81971583, No. 82271956), Shanghai Municipal Science and Technology Major Project (No. 2018SHZDZX01), National Key R&D Program of China (No. 2018YFC1312900).
References
1. Yoon JH, Lee JM, Kang H-j, et al. Quantitative assessment of liver function by using gadoxetic acid–enhanced MRI: hepatocyte uptake ratio. Radiology 2019;290(1):125-133.
2. Watanabe H, Kanematsu M, Goshima S, et al. Staging hepatic fibrosis: comparison of gadoxetate disodium–enhanced and diffusion-weighted MR imaging—preliminary observations. Radiology 2011;259(1):142-150.
3. Li X-Q, Wang X, Zhao D-W, et al. Application of Gd-EOB-DTPA-enhanced magnetic resonance imaging (MRI) in hepatocellular carcinoma. World J Surg Oncol 2020;18(1):1-8.
4. Kisseleva T, Brenner D. Molecular and cellular mechanisms of liver fibrosis and its regression. Nat Rev Gastroenterol Hepatol 2021;18(3):151-166.
5. Ozaki K, Matsui O, Kobayashi S, et al. Selective atrophy of the middle hepatic venous drainage area in hepatitis C–related cirrhotic liver: morphometric study by using multidetector CT. Radiology 2010;257(3):705-714.
6. Wu Z, Matsui O, Kitao A, et al. Hepatitis C related chronic liver cirrhosis: feasibility of texture analysis of MR images for classification of fibrosis stage and necroinflammatory activity grade. PLoS One 2015;10(3):e0118297.
7. Scheuer PJ. Classification of chronic viral hepatitis: a need for reassessment. J Hepatol 1991;13(3):372-374.
8. Isola P, Zhu J-Y, Zhou T, Efros AA. Image-to-image translation with conditional adversarial networks. In: Proceedings of the 2017 IEEE Conference on Computer Vision and Pattern Recognition (CVPR). Honolulu, HI: Institute of Electrical and Electronics Engineers, 2017; 5967-5976. doi: 10.1109/CVPR.2017.632.
Figures