0867
Pathology Without a Knife: MRI-based Non-invasive Determination of Prostate Cancer Grade with Physics-Informed Deep Learning1University of Chicago, Chicago, IL, United States
Synopsis
Keywords: Diagnosis/Prediction, Cancer
Motivation: Millions of prostate biopsies are being ordered each year, a great majority of which yield negative results. A reliable and non-invasive method for detecting prostate cancer grade is critical.
Goal(s): To develop a robust and efficient MRI-based non-invasive model to detect the Gleason score of the lesions without the need for a biopsy.
Approach: We propose a physics-informed autoencoder that integrates the strengths of model-based and deep learning-based methods, while overcoming their respective weaknesses.
Results: Physically-interpretable biomarkers that our model yields correlate strongly with Gleason score, providing important new diagnostic markers, and laying the groundwork for a potential new quantitative MRI method.
Impact: The proposed model offers for many potential usages in diagnostic radiology, by presenting a non-invasive method for diagnosing and staging prostate cancer, potentially affecting about a million patients annually by reducing unnecessary biopsies and saving millions in healthcare costs.
Introduction
MRI is the current non-invasive screening paradigm for prostate cancer, however histopathology remains the gold standard for diagnosis. Consequently, millions of biopsies are being ordered each year, a great majority of which yield negative results. A reliable and non-invasive method for analyzing prostate tissue is critical to reduce the massive number of unnecessary biopsies performed annually. The treatment plan (active surveillance, radiotherapy, prostatectomy etc.) for the patient is decided per the pathology’s determination of the cancer severity, measured with the Gleason scoring system. To date, there’s no validated and clinically accepted MRI-based non-invasive model to detect the Gleason score of the lesions without the need for a biopsy. This study proposes a zero-shot deep learning framework that predicts the Gleason score of a lesion using the diffusion-relaxation model of MR signals.Methods
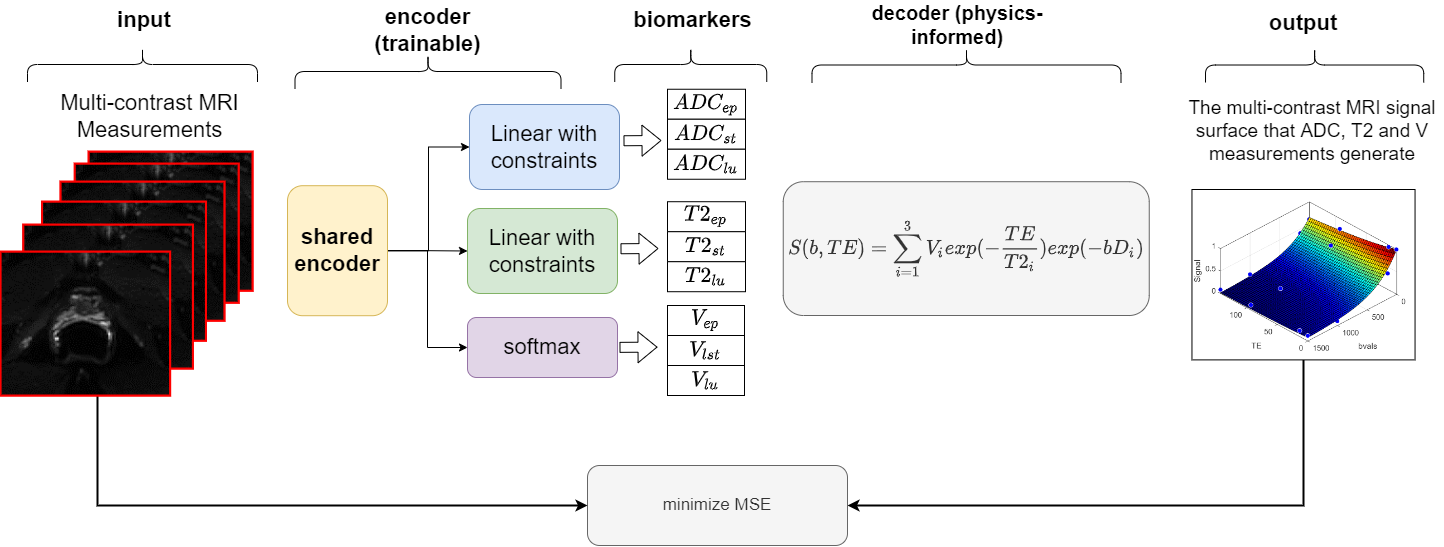
Our novel Physics-Informed Autoencoder (PIA) model leverages a multi-dimensional diffusion-relaxation MR signal model, acquired at multiple b-values and echo times (TE), for self-supervision. The diffusion-relaxation model is designed to determine the volume fractions (v) and the T2 and apparent diffusion coefficient (ADC) values for three distinct tissue compartments—epithelium, stroma, and lumen—by fitting the signal to the model in equation below:$$$\S(b,TE)/S0 = \sum_{n=1}^3 v_n\times exp(-ADC_n\times b-\frac{TE}{T2_n})$$$
We have re-envisioned tissue composition estimation with PIA, transitioning from a nonlinear least squares (NLLS) fit to a more robust deep learning framework. PIA consists of two parts: the encoder, a multi-head neural network that predicts the underlying biomarkers for the given MR signals, and a decoder, non-trainable biophysical model function, that reproduces the MR signals using the output of the encoder (Fig.1). During training, the encoder learns to emulate the decoder's physical rules, hence the term 'Physics-Informed.' PIA is trained in an unsupervised manner by minimizing the squared error between its input S and the so-called "physics-informed output". First, we first conducted Monte Carlo experiments to compare the accuracy of PIA against the simulated ground truth and also the conventional NLLS solution. For this, we simulated signals based on various tissue compositions where ground truth values (v, ADC, T2) were uniformly sampled from the possible range of values for each compartment. For instance, the ADC of stroma was sampled from the range (0.7-1.7um2/s) and so on. Like denoising autoencoders, we pretrained PIA on millions of such synthetic MRI signals using additive Gaussian noise in the input. Subsequently, we evaluated the biomarker accuracy of PIA against a separate set of 2500 simulated tissue samples and the NLLS solution, using a Pearson correlation coefficient (PCC). In-vivo evaluations were performed on 25 pathology-proven prostate cancer patients, using 75 lesions from various grades of cancers (Gleason score) as well as healthy regions from peripheral and transition zones. The PIA estimates were validated with quantitative histology-based true tissue compositions using PCC. For estimating the Gleason scores, we used these new biomarkers (volume, ADC and T2 of epithelium, stroma and lumen) and calculated the PCC and Lin Concordance Correlation Coefficient (CCC) with the Gleason scores of the lesions.
Results
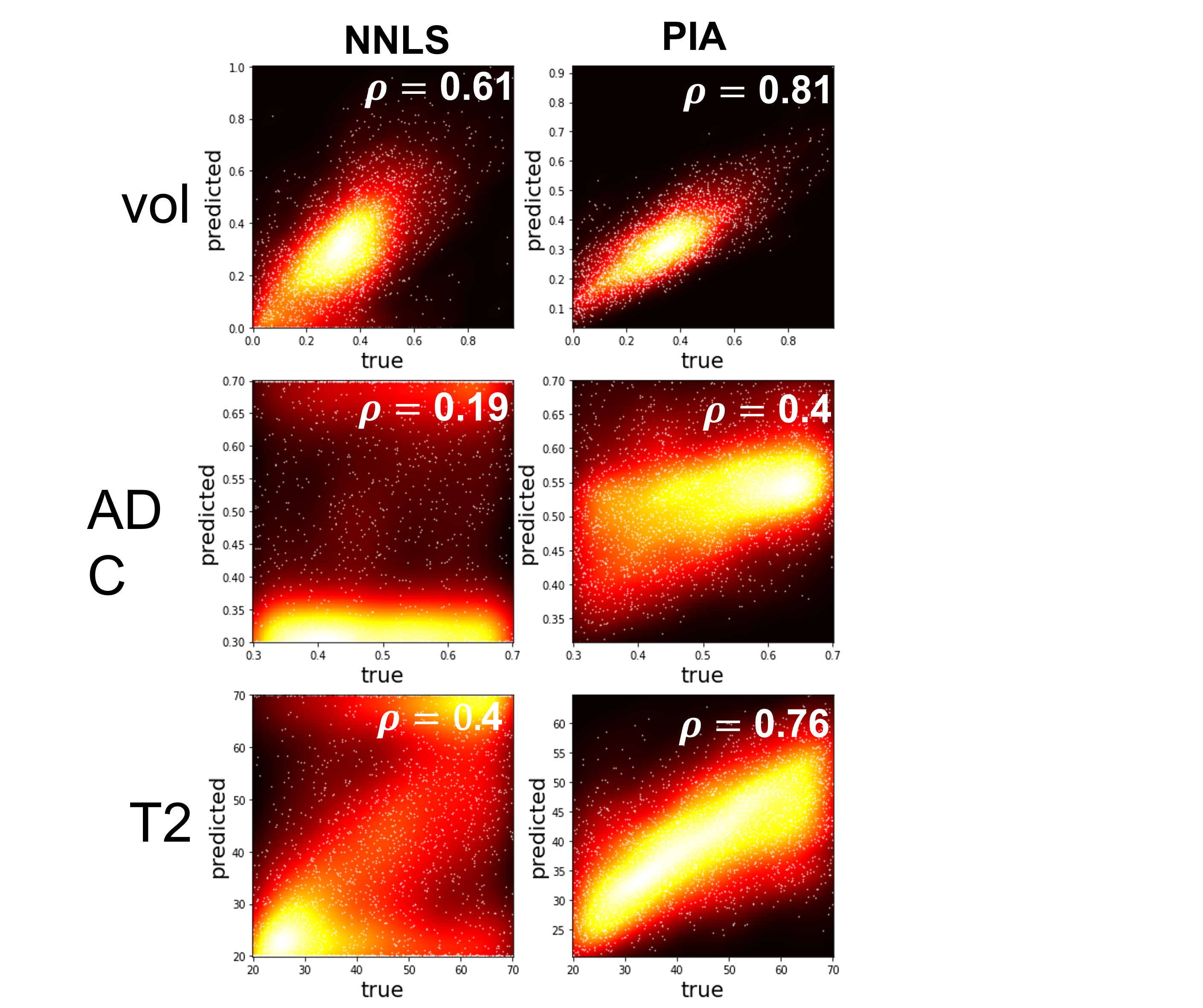
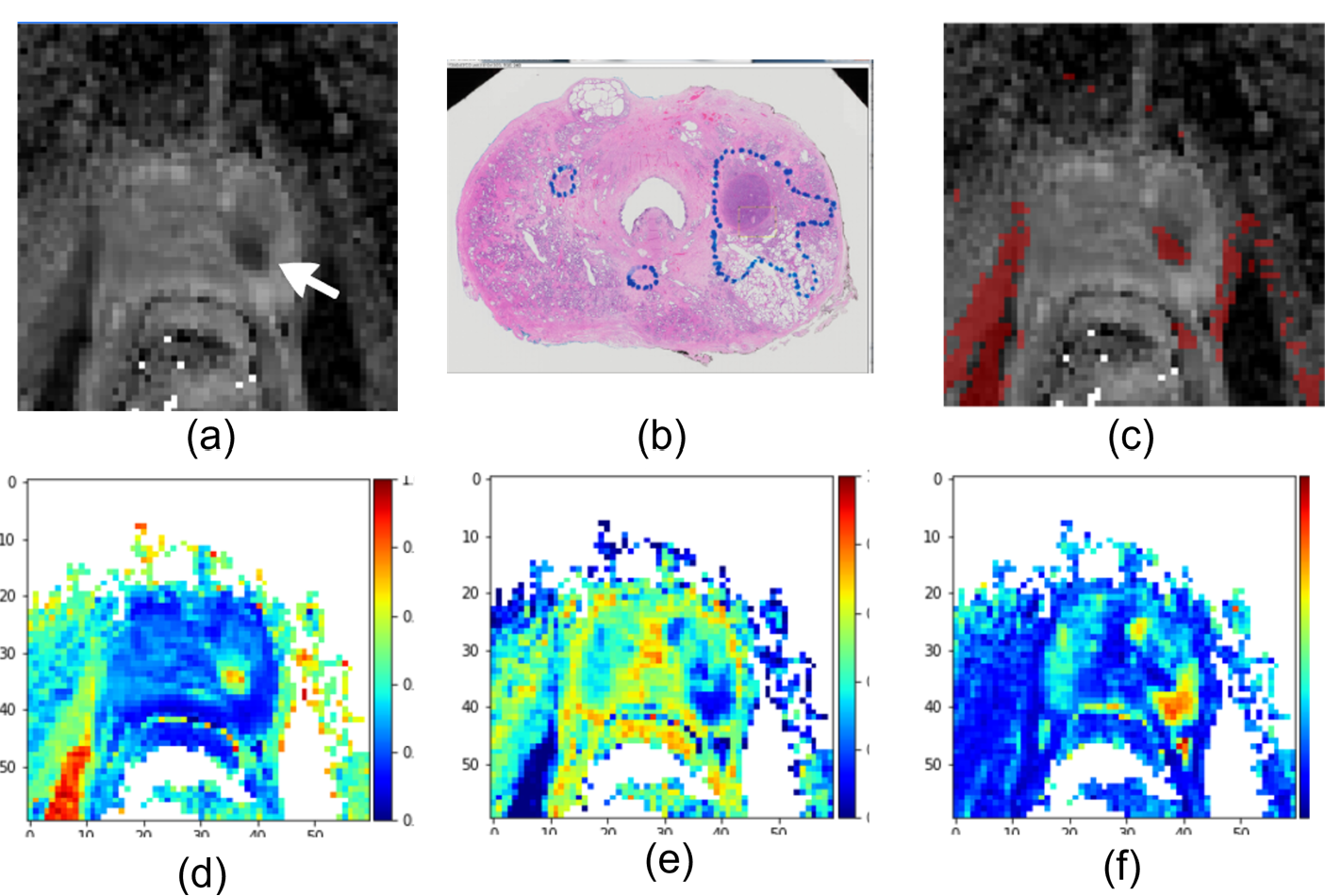
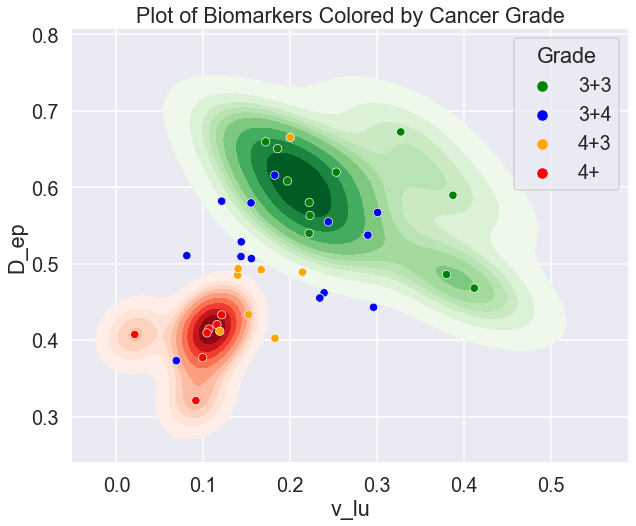
In Monte Carlo Simulations, PIA delivered significantly more accurate measurements than the NLLS-based solution across all biomarkers. One very important finding is that PIA has significant superiority over NLLS solution especially for the terms in the exponents, i.e., the ADC and T2 of the compartments. Scatter plots in Fig. 2 illustrate the predictive performance of PIA versus actual measurements for epithelium, highlighting the method's advantage. In in-vivo experiments, PIA yielded a significant correlation with the histology with r=0.911 for epithelium, r=0.851 for stroma, and r=0.912 for lumen, which was superior to the NNLS-based solution and also about 10,000 times faster (Fig.3). PIA's biomarkers showed strong correlation with Gleason Scores yielding coefficients (r=0.69, CCC=0.63 for epithelium volume; r=0.68, CCC=0.62 for epithelium ADC; r=0.65, CCC=0.60 for lumen volume). The scatter plot on axes spanned by the epithelium ADC and lumen volume showing lesions with different Gleason scores is given in Fig.4.Discussion
This study introduces a new paradigm that integrates the strengths of physics model-based and deep learning-based methods, while overcoming their respective weaknesses, including the need for large amounts of annotated data. The advantage of our model is that it treats the biomarkers not as unknowns of an equation set but as latent variables of an autoencoder.Conclusion
These findings position PIA as a promising non-invasive instrument for predicting the Gleason score from MRI, providing important new diagnostic markers, and laying the groundwork for a potential new quantitative MRI method.Acknowledgements
Supported by the National Institutes of Health (R01 CA227036, 1R41CA244056-01A1, R01 CA17280, and 1S10OD018448-01), Sanford J. Grossman Charitable Trust and University of Chicago Medicine Comprehensive Cancer Center (P30 CA014599-37).References
[1] R. L. Siegel, K. D. Miller, N. S. Wagle, and A. Jemal, “Cancer statistics, 2023,” CA A Cancer J Clinicians, vol. 73, no. 1, pp. 17–48, Jan. 2023, doi: 10.3322/caac.21763.
[2] T. Barrett, B. Turkbey, and P. L. Choyke, “PI-RADS version 2: what you need to know,” Clinical Radiology, vol. 70, no. 11, pp. 1165–1176, Nov. 2015, doi: 10.1016/j.crad.2015.06.093.
[3] A. Chatterjee et al., “Validation of Prostate Tissue Composition by Using Hybrid Multidimensional MRI: Correlation with Histologic Findings,” Radiology, vol. 302, no. 2, pp. 368–377, Jan. 2022, doi: 10.1148/radiol.2021204459.
[4] H. Li, C. H. Lee, D. Chia, Z. Lin, W. Huang, and C. H. Tan, “Machine Learning in Prostate MRI for Prostate Cancer: Current Status and Future Opportunities,” Diagnostics, vol. 12, no. 2, p. 289, Jan. 2022, doi: 10.3390/diagnostics12020289.
[5] G. E. Karniadakis, I. G. Kevrekidis, L. Lu, P. Perdikaris, S. Wang, and L. Yang, “Physics-informed machine learning,” Nat Rev Phys, vol. 3, no. 6, pp. 422–440, May 2021, doi: 10.1038/s42254-021-00314-5.
Figures