0864
An MRI-based nomogram predicts brain metastasis response to targeted therapy in lung cancer patients: A multi-center study1Sun Yat-Sen Memorial Hospital, Sun Yat-Sen University, Guangzhou, China, 2Sun Yat-sen University Cancer Center, Guangzhou, China, 3Shantou Central Hospital, Shantou, China, 4The Tenth Affiliated Hospital of Southern Medical University, Dongguan People's Hospital, Dongguan, China, 5The First Affiliated Hospital of USTC, University of Science and Technology of China, Hefei, China, 6Qinzhou First People's Hospital, Qinzhou, China, 7Guangdong 999 Brain Hospital, Guangzhou, China, 8Capital Medical University, Beijing, China
Synopsis
Keywords: Diagnosis/Prediction, Machine Learning/Artificial Intelligence, lung cancer patients with brain metastasis
Motivation: To determine an effective individualized treatment decision for lung cancer patients with brain metastasis (BrM) to receive targeted therapy.
Goal(s): we developed an MRI-based nomogram that can predict the response of lung cancer BrM to targeted therapy using multi-center data.
Approach: Clinical predictors, radiomics and deep learning features extracted from BrM baseline MR images were incorporated to establish the nomogram using the LASSO logistics coefficients.
Results: The nomogram can accurately predict the 6-month and 12-month responses of BrM to targeted therapy across the training cohort, internal validation cohort, and external test set, outperforming all other models.
Impact: The MRI-based nomogram can be used as a pretreatment and personalized tool to predict response to targeted therapy in lung cancer patients with BrMs and thus assist in optimizing treatment for lung cancer patients who suffer from BrMs.
Introduction
Brain metastases (BrMs) are the most common intracranial neoplasms, which occur ten times more frequently than primary brain tumors1. Among patients with BrMs, lung cancer is the most prevalent primary tumor site2. Up to 40% of lung cancer patients experience BrM over the disease course3. Targeted therapy played a significant role in lung cancer patients with BrMs. However, the non-response of targeted therapy may delay the optimal timing of treatment. Therefore, we developed and externally validated an MRI-based nomogram for predicting brain metastasis response to targeted therapy, facilitating clinical decision-making and treatment planning in lung cancer patients with BrMs.Methods
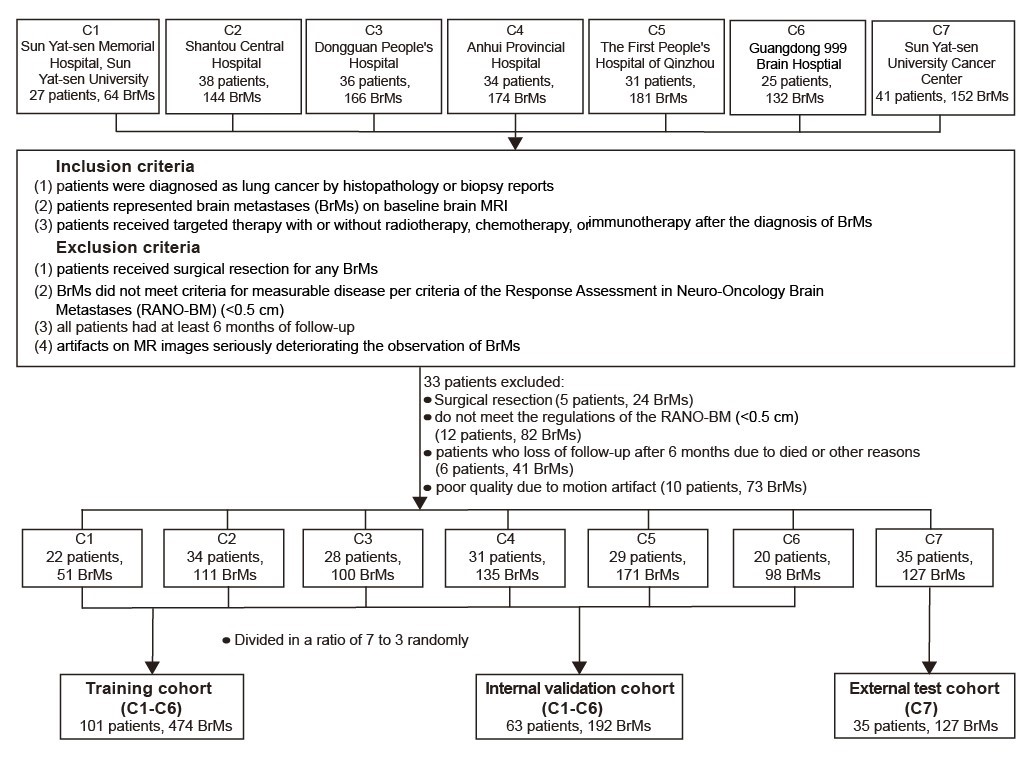
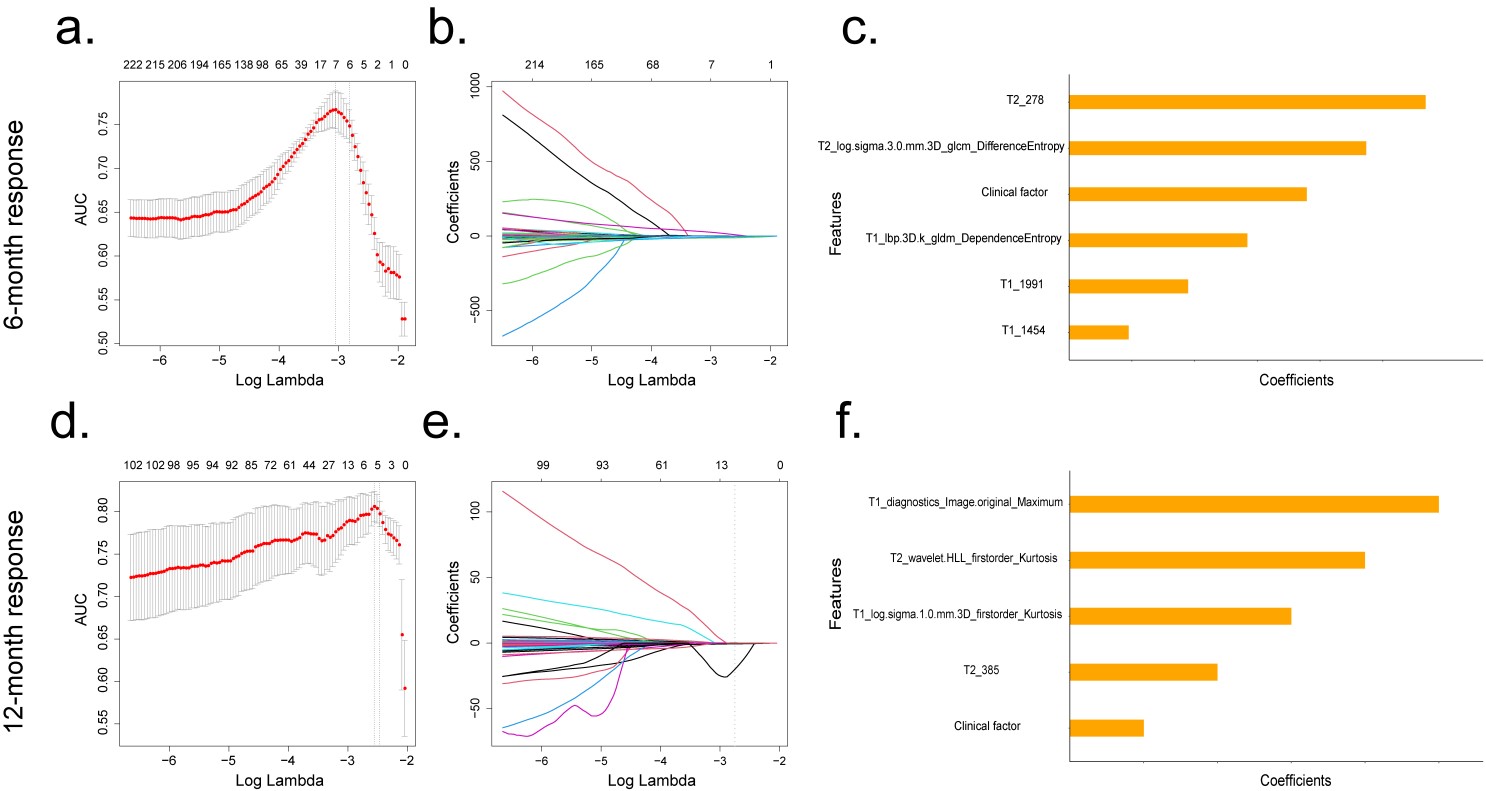
One hundred and ninety-nine lung cancer patients with 793 BrMs who underwent targeted therapy were retrospectively included from seven centers (training cohort: 101 patients, 474 BrMs; internal validation cohort: 63 patients, 192 BrMs; external test set: 35 patients, 127 BrMs). The inclusion and exclusion standards are shown in Figure 1. A total of 4350 radiomics features (2175 features from CE-T1WI and 2175 features from T2WI) and 4096 deep learning-based features (2048 features from CE-T1WI and 2048 features from T2WI) were extracted from the corresponding BrM MR images. The least absolute shrinkage and selection operator (LASSO) logistic regression was performed to select independent clinical predictors, significant radiomics, and deep learning features for predicting BrM 6-month and 12-month responses to targeted therapy (Figure 2). Clinical, radiomics, and deep learning models were established, respectively. The combined model was developed by incorporating the above models with the LASSO logistics coefficients and then presented as a nomogram. Model performances were evaluated and compared.Results
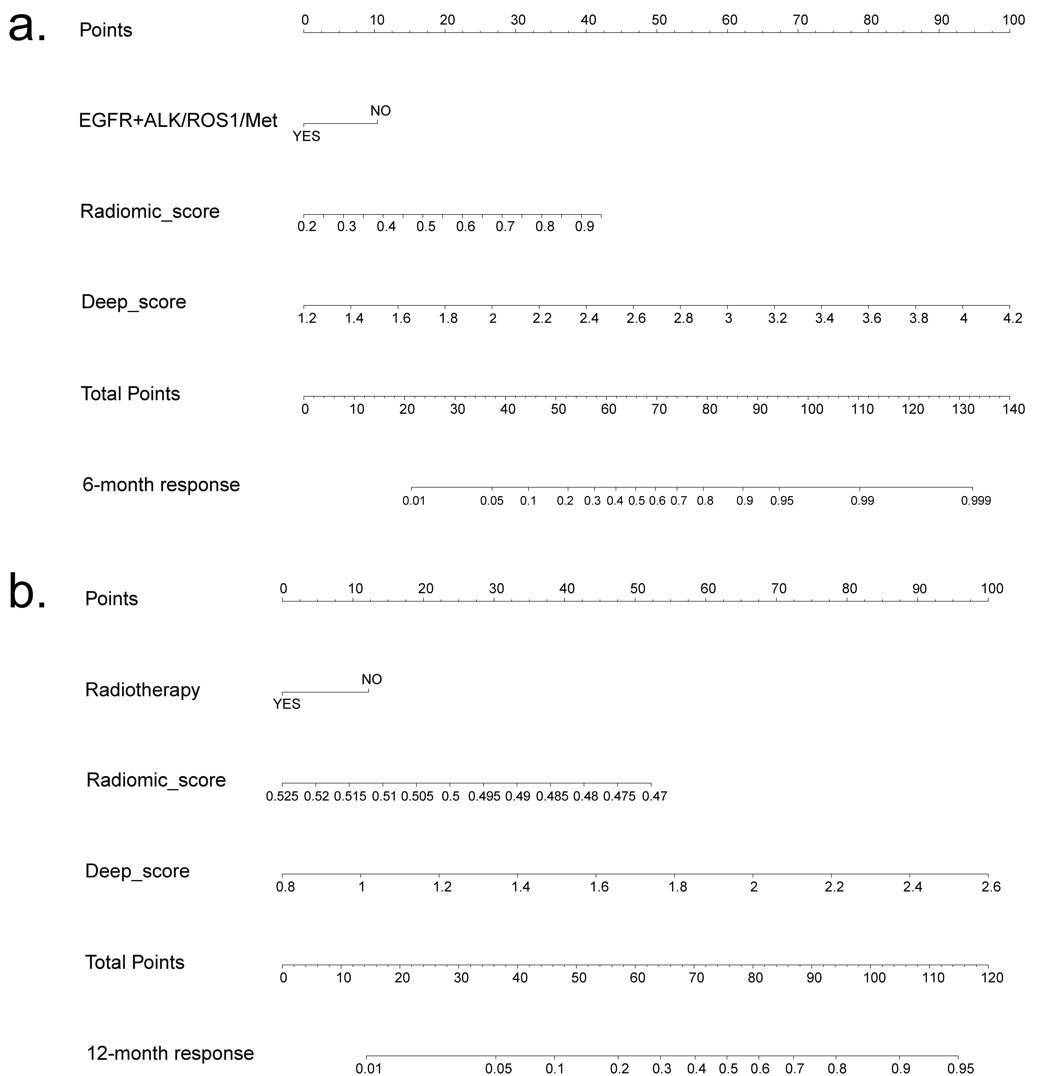
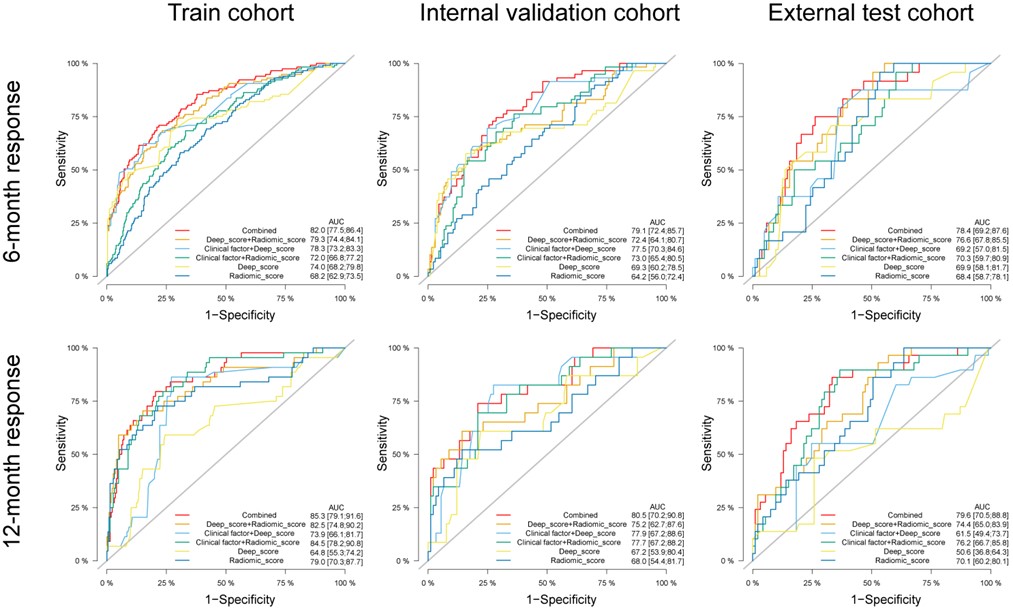
A mutant gene of targeted therapy, two radiomics features, and three deep learning features were selected for the 6-month response-predicted nomogram (Figure 3a). The 12-month predicted nomogram consisted of radiotherapy, 3 radiomics features and 1 deep learning feature (Figure 3b). Both nomograms showed a high level of concordance with the actual probability of BrM response in training, validation, and the test cohort (Figures 3b and 4b). The diagnostic performance of all models is presented in Figure 4. The AUCs of 6-month predicted nomogram were 0.820, 0.791, and 0.784 in the training, internal validation, and external test cohorts, respectively. For the 12-month predicted nomogram, the AUCs in each cohort were 0.853, 0.805 and 0.796. In both 6- and 12-month response prediction, combined models outperformed other models (all P < 0.05).Discussion
To the best of our knowledge, this is the first study to predict BrM-targeted therapy responses in lung cancer patients. Our results suggested that an MRI-based nomogram could accurately predict the treatment response of BrM at different time points. A total of six centers were set as the train cohort, while one center was set as the external test cohort. Various MRI scanners and different imaging acquisition parameters were included. Our results show that the nomogram performed well to predict the response of BrM to targeted therapy across the training cohort, internal validation cohort, and external test set, further highlighting its potential generalizability. The nomogram incorporates clinical features such as radiotherapy, targeted therapy targeting mutated genes (EGFR+ALK/ROS1/Met), along with radiomics features and deep learning-based features. Previous studies have shown that the combination of radiotherapy and targeted therapy can significantly prolong the survival time of patients4. Besides, it had been proven that BrM patients with EGFR and ALK gene alterations had a better prognosis for lung cancer5, consistent with the clinical characteristics that the nomogram included. The nomogram included radiomics features associated with the texture heterogeneity of lesions. Previous studies have proved that texture heterogeneity is relevant to the treatment response and prognosis of tumor6-7. Except for radiomic features, our models also contained deep learning features that were extracted by the MedicalNet model. Previously, either radiomics models or deep signature-based models have been used to predict therapy response or survival in patients with brain tumors, and the addition of radiomics features or deep features could enhance the predictive abilities of clinical models8-9.Conclusion
The nomogram showed excellent and stable performance in predicting BrM response to targeted therapy pretreatment, providing a noninvasive and practical way to optimize treatment planning for lung cancer patients with BrMs.Acknowledgements
NoneReferences
- Epidemiology of brain metastases and leptomeningeal disease. Neuro Oncol. 2021 ;23(9):1447-1456.
- Incidence and prognosis of patients with brain metastases at diagnosis of systemic malignancy: a population-based study. Neuro Oncol. 2017 ;19(11):1511-1521.
- Suppressed immune microenvironment and repertoire in brain metastases from patients with resected non-small-cell lung cancer. Ann Oncol. 2019 ;30(9):1521-1530.
- Effect of EGFR-TKIs combined with craniocerebral radiotherapy on the prognosis of EGFR -mutant lung adenocarcinoma patients with brain metastasis: A propensity-score matched analysis. Front Oncol.2023 ;9:13:1049855.
- An Update of the Graded Prognostic Assessment for Lung Cancer Using Molecular Markers (Lung-molGPA). JAMA Oncol. 2017 ;3(6):827-831.
- Predicting response to cancer immunotherapy using noninvasive radiomic biomarkers. Ann Oncol. 2019 ;30(6):998-1004.
- Radiomic machine learning for predicting prognostic biomarkers and molecular subtypes of breast cancer using tumor heterogeneity and angiogenesis properties on MRI. Eur Radiol. 2022 ;32(1):650-660.
- Development and validation of a radiomics-based prediction pipeline for the response to stereotactic radiosurgery therapy in brain metastases. Eur Radiol. 2023 Jul 28. doi: 10.1007/s00330-023-09930-4.
- Prediction of Response to Stereotactic Radiosurgery for Brain Metastases Using Convolutional Neural Networks. Anticancer Res. 2018 ;38(9):5437-5445.
Figures