0860
Prediction of pathological complete response in breast cancer by histogram signatures from multi-phase contrast enhanced MRI1Radiology, Peking University Cancer Hospital & Institute, Beijing, China, 2Radiology, Beijing Chao-Yang Hospital, Beijing, China
Synopsis
Keywords: Diagnosis/Prediction, Cancer
Motivation: Accurate prediction of pathological complete response (pCR) after neoadjuvant chemotherapy enables individualized treatment options to avoid unnecessary breast excision and improve patients’ life quality.
Goal(s): To improve the prediction accuracy by simultaneously extracting temporal and spatial features of MRI signal during contrast enhancement.
Approach: A histogram signature is designed by concatenating histograms at different enhancing phases into a 2D picture and classified by convolutional neural network into pCR or non-pCR.
Results: The AUC, sensitivity, specificity of the histogram signature for pCR prediction is 0.833 in the test group (n=132). The model combining histogram signature with ER and HER2 increases AUC to 0.842.
Impact: Histogram signatures from multi-phase MRI can be used as a new marker to measure tumor heterogeneity, estimate drug uptake, evaluate treatment response and predict prognosis for breast cancer or other cancers.
Purpose
Neoadjuvant chemotherapy (NAC) is the standard treatment for locally advanced breast cancer (LABC) [1]. The ideal response to NAC is pathological complete response (pCR) determined by postoperative specimen. If pCR can be accurately predicted after NAC, patients may avoid unnecessary breast excision [2]. Many studies have proposed pCR prediction models based on multi-phase gadolinium enhanced MRI data either by weighted summing spatial features from different phases [3,4] or by extracting texture features from temporally fitted parameter maps [5]. However, these two-step algorithms cannot balance the importance of spatial features and temporal features. It is encouraging to develop new features to simultaneously characterize temporal change and spatial distribution of MRI signal during enhancement. In this study, a method of histogram signature containing both spatial and temporal information is proposed to predict the response to NAC for breast cancer based on post-NAC MRI data.Methods
The prospective study was approved by our institutional ethics committee. 331 patients from January 2015 to December 2016 were included and randomly divided into a training group (n=165), a validating group (n=34), and a test group (n=132). 5 clinical features were collected, including: estrogen receptor (ER), progesterone receptor (PR), human epidermal growth factor receptor 2 (HER2) and Ki-67. HER2 negative patients received doxorubicin and cyclophosphamide every two weeks for four cycles followed by four cycles of paclitaxel. HER2 positive patients received treatment with docetaxel and trastuzumab every three weeks for six cycles. All patients were scanned on the same 1.5T MR scanner (GE Optima MR360). A sagittal vibrant SPGR sequence was used (TR=6.4ms, TE=3.0ms, FA=10°, slice thickness=4mm, gap=0, matrix=256×256, FOV=20-22cm). Acquisition was performed at 6 phases, with one phase before and 5 phases (2.0, 3.5, 5.0, 6.5, 8.0 minutes) after Gd-DTPA enhancement. Figure 1 shows the steps of creating histogram signature from multi-phase MRI data. First, tumor center was manually marked by an experienced radiologist. Second, a L×L×3 box is automatically generated (L=10, 20, 30, 40 pixels). Third, histogram of the signals inside the box at each phase was calculated with 50 bins dividing gray level from 100 to 2600. The low limit of 100 HU excludes most noise from the background. Finally, all 6 histograms were concatenated vertically to construct a histogram signature as a 6×50 picture. The histogram signature contains spatial information along one dimension and temporal information along the other dimension. Standard histopathological analysis was processed for the pathologic assessment of the response to NAC as the ground truth. An absence of invasive cancer cells in the breast surgical specimen or ipsilateral sentinel lymph node or resected axillary lymph nodes was defined as pCR. The histogram signatures were trained by a classification network (Figure 2) that was composed by 7 repetitions of a convolutional layer and a ReLU layer. The final fully-connected layer followed by a softmax function outputs the probability of the two labels: pCR and non-pCR. Clinical model was constructed by a logistical regression that forwardly selects the 5 clinical features. A combined model was constructed by including the histogram signature score and the selected clinical features into a linear model.Results
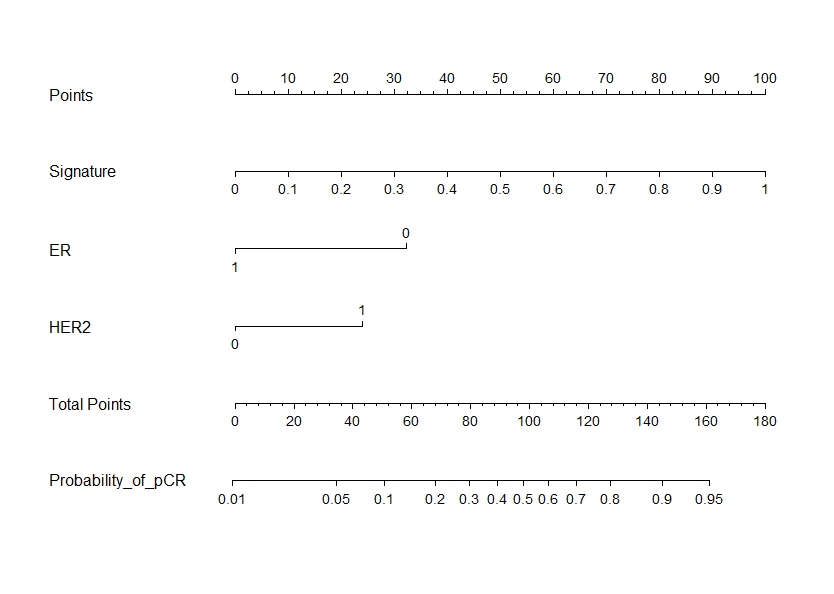
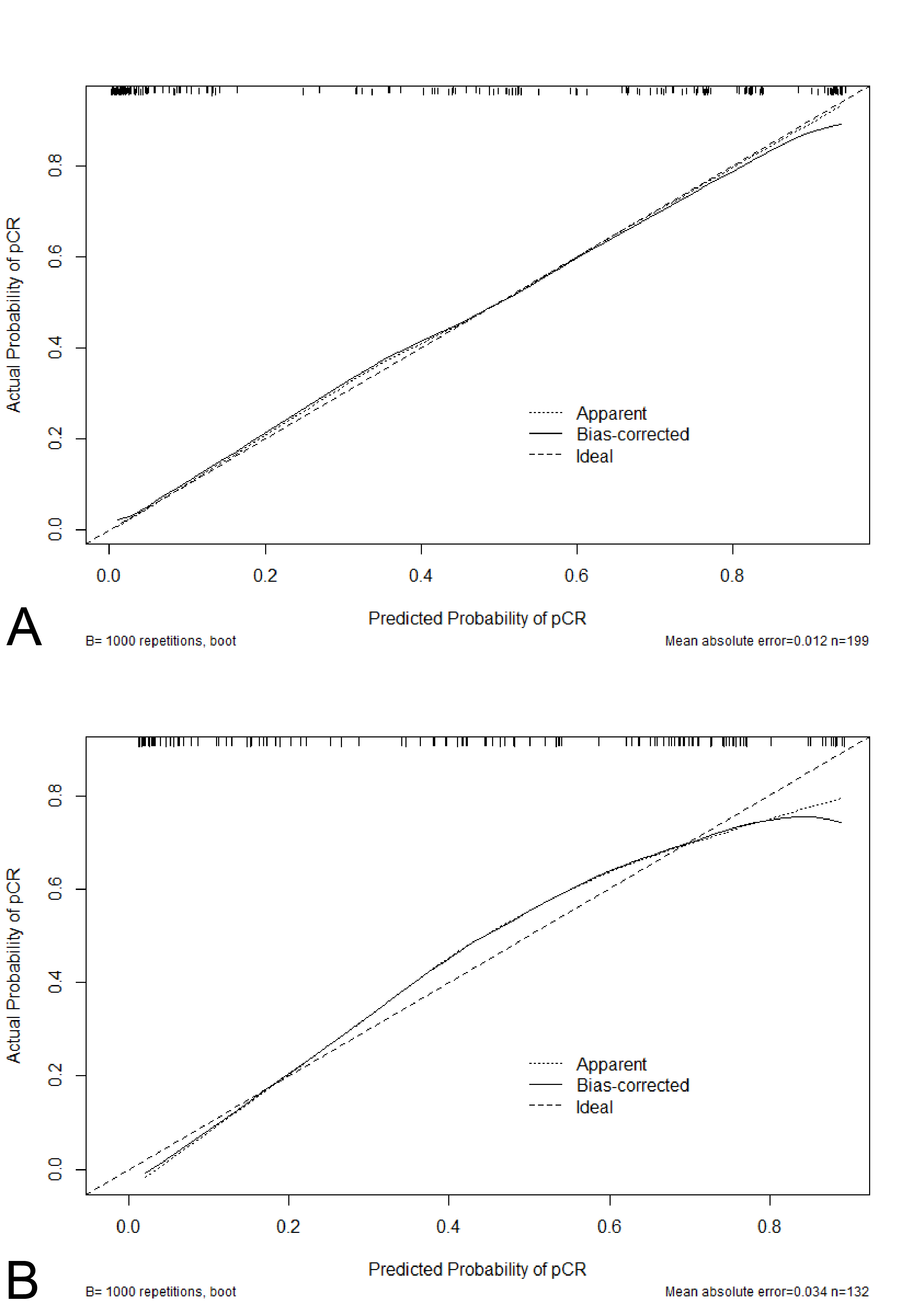
Student's t test and chi-square test shows no significant difference of age, molecular type and pathological result among the 3 groups (p>0.05). Figure 3 shows the change of AUC in the training group and validating group for histogram signatures with L=10, 20, 30, 40 voxels from 1 to 10000 epochs. L=20 voxels and epochs=5258 were selected as the optimal parameters by considering the performance on both groups. The corresponding weights of the network were used for pCR prediction in the testing group. Receiver operating characteristic (ROC) curves are shown in Figure 4A. The AUC is 0.897 (95%CI: 0.847-0.947), 0.881 (95%CI: 0.765-0.996) and 0.833 (95%CI: 0.764-0.903) for the training, validating and testing groups respectively. The sensitivity and specificity in the testing group is 83.9% and 72.4%. The AUC of histogram signature is significantly (Z=2.960, P=0.003) larger than the clinical model including ER and HER2 with an AUC of 0.676 (95%CI: 0.588-0.765) in the testing group. Figure 5 is the nomogram of linearly combining histogram signature score with ER and HER2. Its calibration curves are shown in Figure 6. The AUC, sensitivity and specificity of the combined model is 0.842 (95%CI: 0.775-0.909), 82.1% and 75.0% in the testing group. ROC curves of different models are shown in Figure 4B.Conclusion
Histogram signatures containing both temporal and spatial features can be used to predict pCR after NAC for locally advanced breast cancer by convolutional neural networks and a manually marked tumor center in post-NAC MRI images.Acknowledgements
No acknowledgement found.References
[1] Kaufmann M, von Minckwitz G, Bear HD, et al. (2007). Recommendations from an international expert panel on the use of neoadjuvant (primary) systemic treatment of operable breast cancer: new perspectives 2006. Ann Oncol;18(12):1927-1934.
[2] Cortazar P, Zhang L, Untch M, Mehta K, Costantino JP, Wolmark N, et al. (2014). Pathological complete response and long-term clinical benefit in breast cancer: the CTNeoBC pooled analysis. Lancet; 384(9938):164-72.
[3] Qu Y-H, Zhu H-T, Cao K, Li X-T, Ye M, Sun Y-S (2020). Prediction of pathological complete response to neoadjuvant chemotherapy in breast cancer using a deep learning (DL) method. Thoracic Cancer; 11: 651-658.
[4] Eun NL, Kang D, Son EJ, et al. (2020). Texture analysis with 3.0-T MRI for association of response to neoadjuvant chemotherapy in breast cancer. Radiology, 294(1), 31–41.
[5] Mazurowski MA, Saha A, Harowicz MR, Cain EH, Marks JR, Marcom PK. (2019). Association of distant recurrence-free survival with algorithmically extracted MRI characteristics in breast cancer. Journal of Magnetic Resonance Imaging, 231–240.
Figures