0859
Multiparametric MRI Radiomic Features Improve Patient Selection for Active Surveillance in Prostate Cancer1Department of Radiation Oncology, University of Miami Miller School of Medicine, Miami, FL, United States, 2Department of Urology, University of Miami Miller School of Medicine, Miami, FL, United States, 3Department of Radiology, University of Miami Miller School of Medicine, Miami, FL, United States, 4Department of Pathology, University of Miami Miller School of Medicine, Miami, FL, United States
Synopsis
Keywords: Diagnosis/Prediction, Cancer
Motivation: Accurate selection of prostate cancer patients to undergo active surveillance (AS) is crucial to ensure suitable treatment.
Goal(s): To develop an automated framework for mpMRI analysis to assist clinical decision making about whether a patient should remain on AS.
Approach: We developed a progression risk stratification model using mpMRI data from an AS trial, and incorporating clinical biomarkers and radiomic features from lesions identified by a deep neural network.
Results: The lesion segmentation network achieved a median DSC of 60.7%, and the progression prediction model an AUC of 81.1% in determining likelihood of progression within 12 months.
Impact: We present a fully automated methodology to assess prostate cancer progression risk for AS patients within the timeframe between their follow-up visits, thereby providing essential data for clinicians that can prospectively improve AS patient selection.
Introduction
Out of the around 250,000 patients who are yearly diagnosed with prostate cancer in the U.S, about half are at low risk1 and may consider active surveillance (AS)2,3, a safe alternative to immediate treatment that can reduce the burden of overtreatment. Yet, due to a lack of robust risk-stratification tools predicting histological progression, uncertainties around optimal patient selection remain. Identification of suitable AS candidates is of primary importance to (i) avoid delays in treatment for patients with high-risk of progression as emerging data show an increased risk of metastasis with long follow-up4, (ii) postpone treatment to preserve quality of life for low-risk patients, (iii) safely tailor the intensity of follow-up biopsies. Guidelines for reading prostate multiparametric MRI (mpMRI) using the standardized Prostate Imaging Reporting and Data System (PI-RADS)5, follow a semi-quantitative assessment, susceptible to low inter-reader agreement (<50%) and sub-optimal interpretation6,7. Among the many implemented computer-aided techniques for quantitative mpMRI analysis8,9, methods predicting histological progression are limited10,11. Based on recent findings10, our hypothesis is that using mpMRI to uncover the problem of tumor heterogeneity through quantitative imaging combined with clinical biomarkers can improve risk estimation, resulting in reliable identification of AS candidates.Methods
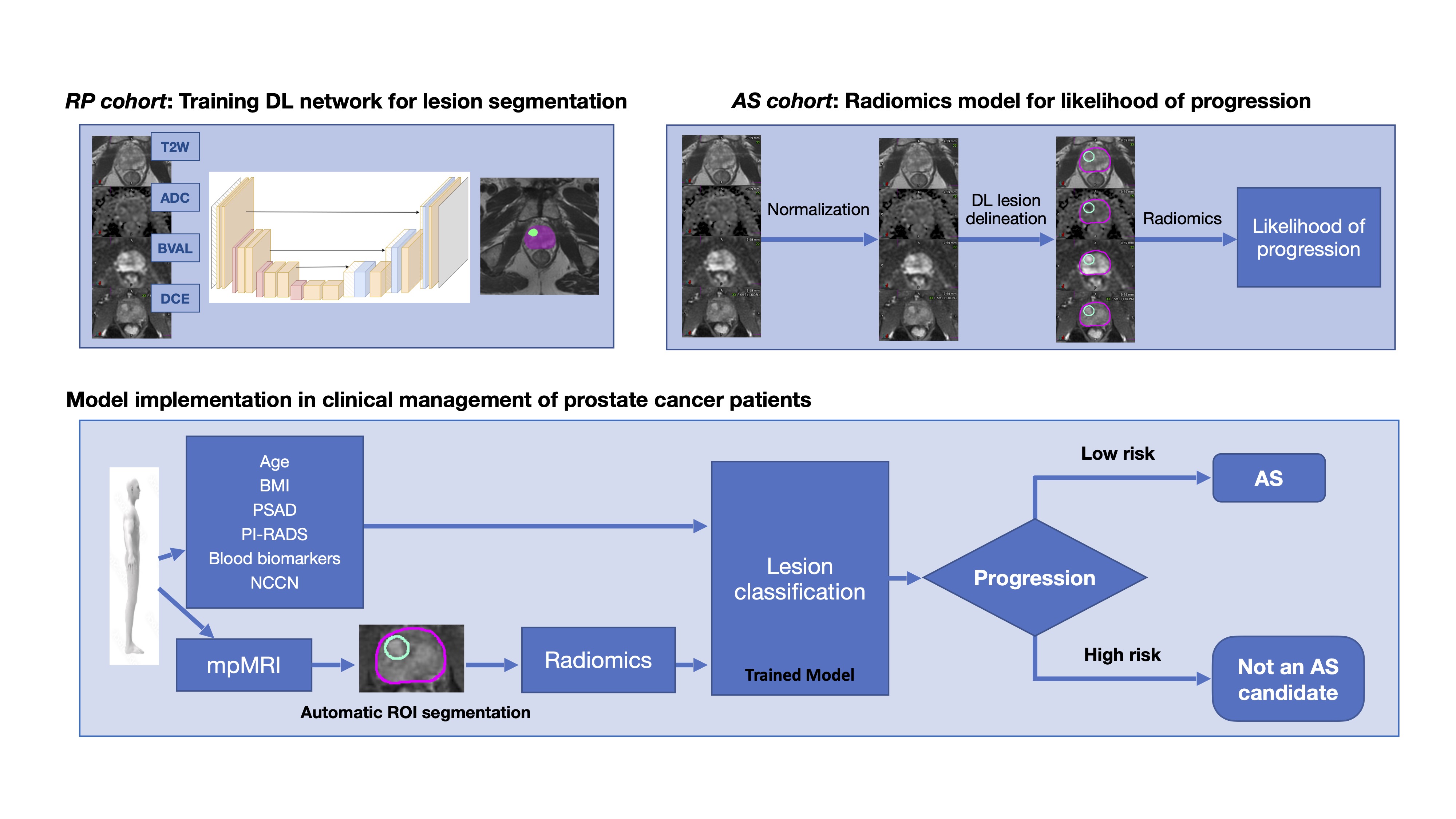
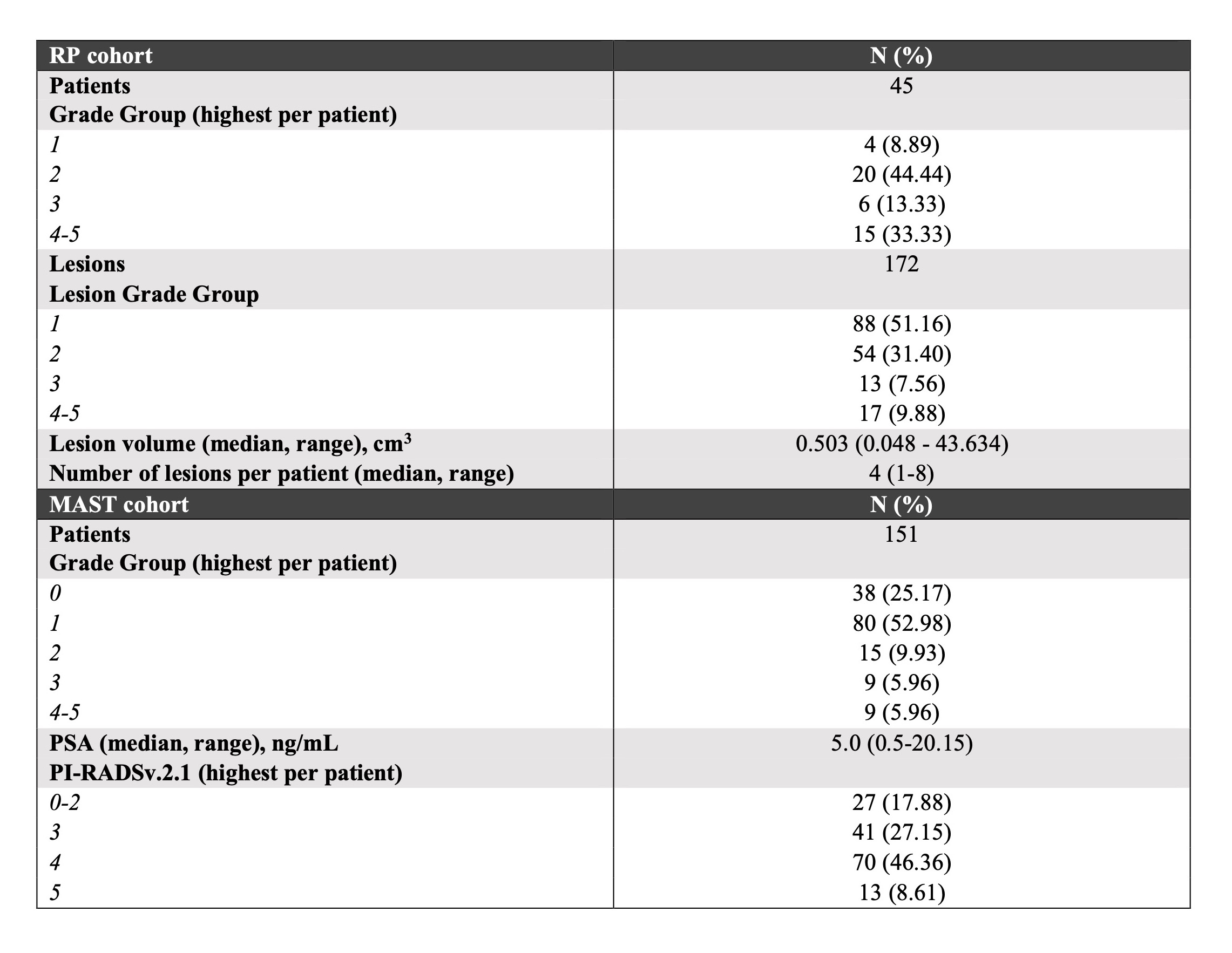
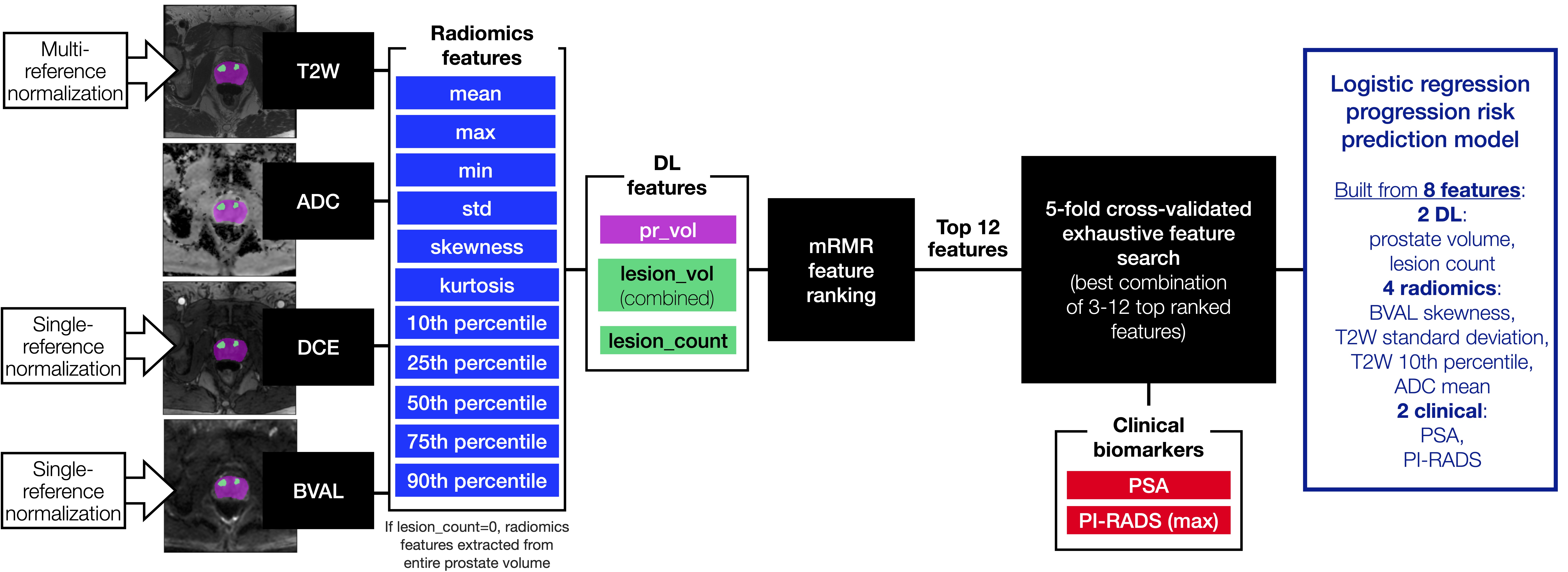
We present a method to predict likelihood of change in prostate cancer histology that consists of three integrated steps (Figure 1): (i) training a neural network by deep learning (DL) for automatic segmentation of prostate and lesions suspicious for cancer; (ii) application of the network to identify lesions on mpMRI for AS patients; (iii) image intensity normalization; and (iv) extraction of radiomics features from the lesions, (v) predicting the likelihood of progression by fusing radiomics with clinical variables.Data from two patient cohorts were utilized for development of the lesion segmentation and risk prediction model, respectively (Table 1):- RP cohort (n=45): mpMRI data with lesions annotated after radical prostatectomy (RP)12.
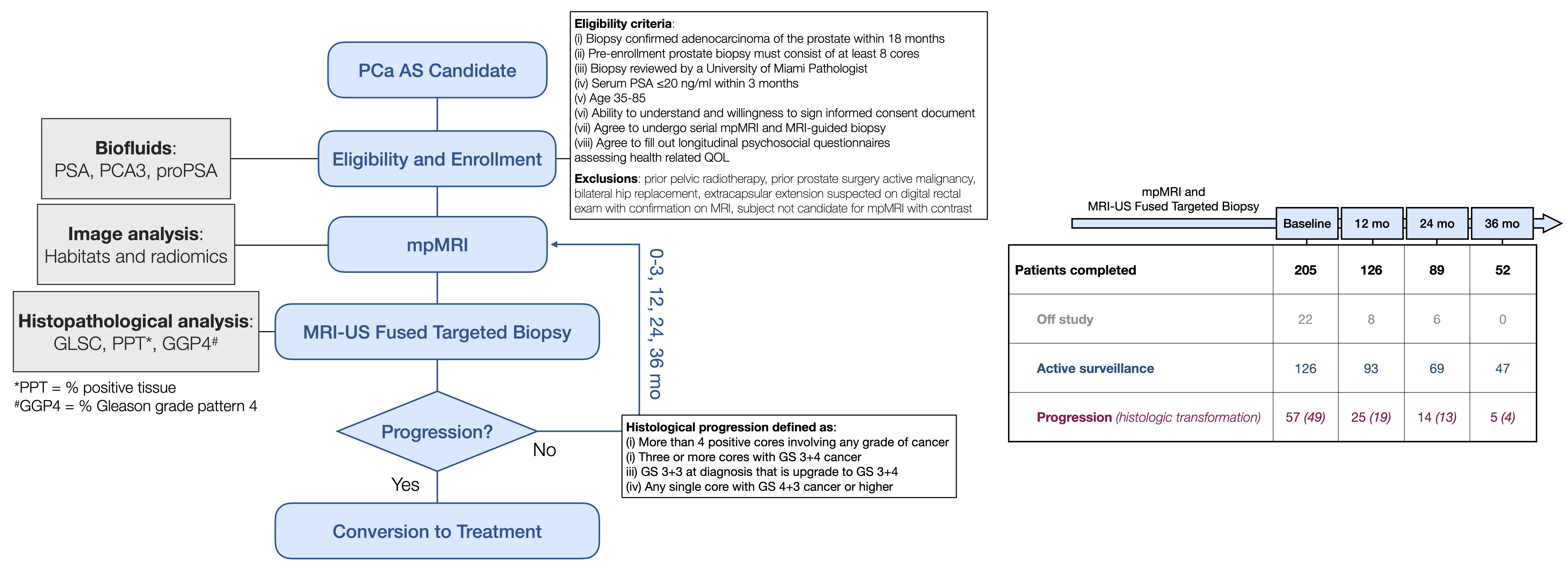
- MAST cohort (n=151): confirmatory mpMRI and clinical data from AS patients enrolled in the MAST trial (Figure 2). The data were further divided into: (a) Training and validation (n=135): patients who showed histological progression at the confirmatory visit or at the first follow-up visit (n=67), and patients who completed the full study without progressing or who are currently on AS with at least the first year follow-up completed without progressing (n=68). (b) Test (n=16): patients who progressed after 12 months were manually reviewed and the time of progression was retroactively adjusted to between 0-24 months and used as ground truth to verify the progression risk model (adjustment applied to 37.5% of patients).
Results
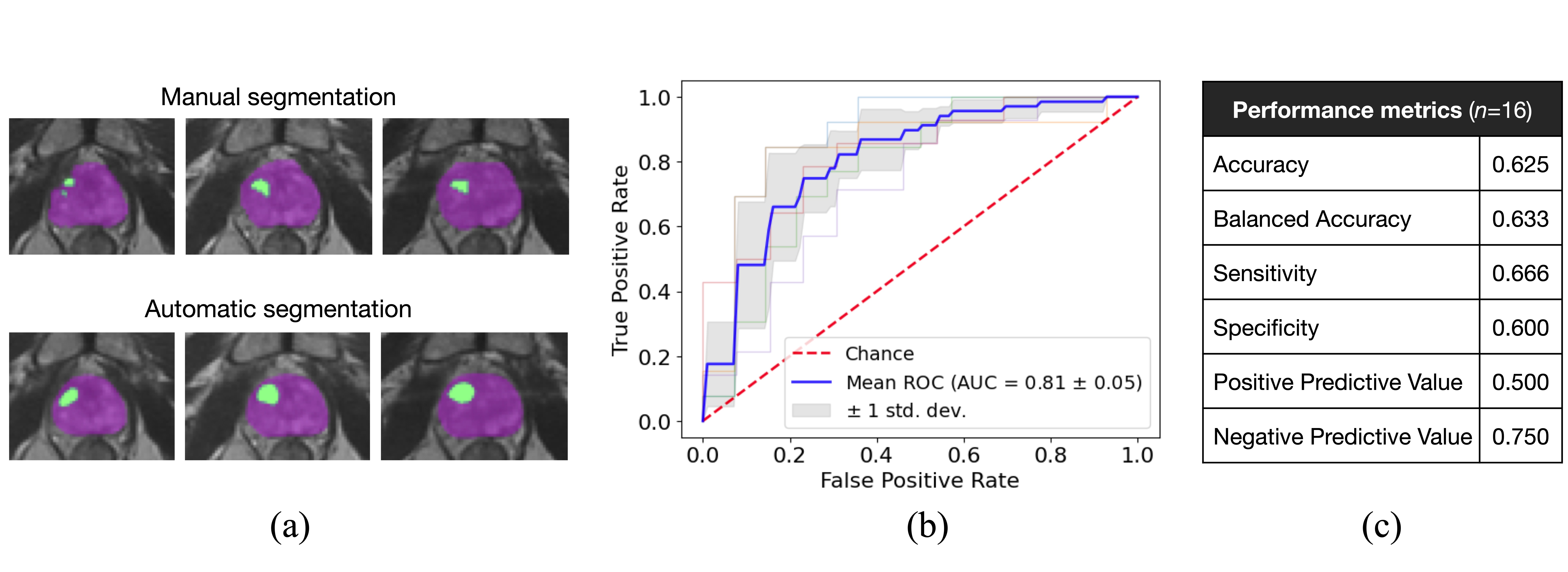
Lesion detection, assessed using the Dice Similarity Coefficient (DSC) through criteria defined in recent work of others15,16, resulted in a median DSC of 0.607 (0.130-0.958). Figure 4a shows the predicted prostate and lesion masks compared to manual masks. The clinical-radiomics model achieved a mean AUC of 0.811±0.01 (averaged over 100 repetitions) on the validation set (Figure 4b). The sensitivity of the model in correctly labeling patients as high-risk was 66.7% when applied to an unseen test set (MAST test subset) (Figure 4c).Discussion and Conclusions
The median DSC of the lesion segmentation network falls in the upper bound compared to similar studies15. The prediction sensitivity among missed progressors indicates that undetected progression, accumulated over 6 years, can be avoided by using the progression risk model. The model performance is promising for future clinical utilization to identify low-risk patients who will benefit by avoiding biopsies and remain on AS using monitoring through imaging only. More importantly, the model can help in avoiding delays in treatment of patients identified as high-risk.Acknowledgements
The research was supported by the National Cancer Institute of the National Institutes of Health under Award Number P30CA240139, RO1CA189295, R01CA190105, and U01CA239141.References
1. Siegel RL, Miller KD, Wagle NS, Jemal A. Cancer statistics, 2023. CA Cancer J Clin 2023;73(1):17-48.
2. Schaeffer E, Srinivas S, Antonarakis ES, Armstrong AJ, Bekelman JE, Cheng H, et al. NCCN guidelines insights: prostate cancer, version 1.2021. J Natl Compr Canc Netw. 2021;19:134–43.
3. Dall’Era MA, Albertsen PC, Bangma C, Carroll PR, Carter HB, Cooperberg MR, Freedland SJ, Klotz LH, Parker C, Soloway MS. Active surveillance for prostate cancer: a systematic review of the literature. European urology. 2012 Dec 1;62(6):976-83.
4. Yamamoto, T. et al. Metastatic Prostate Cancer in Men Initially Treated with Active Surveillance. The Journal of urology 195, 1409-1414, doi:10.1016/j.juro.2015.11.075 (2016).
5. Barentsz JO, Richenberg J, Clements R, et al. ESUR prostate MR guidelines 2012. Eur Radiol. 2012;22(4):746-757.
6. Rosenkrantz AB, Ginocchio LA, Cornfeld D, Froemming AT, Gupta RT, Turkbey B, Westphalen AC, Babb JS, Margolis DJ. Interobserver reproducibility of the PI-RADS version 2 lexicon: a multicenter study of six experienced prostate radiologists. Radiology. 2016 Sep;280(3):793-804.
7. Westphalen AC, McCulloch CE, Anaokar JM, Arora S, Barashi NS, Barentsz JO, Bathala TK, Bittencourt LK, Booker MT, Braxton VG, Carroll PR. Variability of the positive predictive value of PI-RADS for prostate MRI across 26 centers: experience of the society of abdominal radiology prostate cancer disease-focused panel. Radiology. 2020 Jul;296(1):76-84.
8. Delgadillo R, Ford JC, Abramowitz MC, Dal Pra A, Pollack A, Stoyanova R. The role of radiomics in prostate cancer radiotherapy. Strahlenther Onkol. 2020;196(10):900-912.
9. Lemaître G, Martí R, Freixenet J, Vilanova JC, Walker PM, Meriaudeau F. Computer-aided detection and diagnosis for prostate cancer based on mono and multi-parametric MRI: a review. Computers in biology and medicine. 2015 May 1;60:8-31.
10. Ploussard G, Rouvière O, Rouprêt M, van den Bergh R, Renard-Penna R. The current role of MRI for guiding active surveillance in prostate cancer. Nature Reviews Urology. 2022 Jun;19(6):357-65.
11. Rajwa P, Pradere B, Quhal F, Mori K, Laukhtina E, Huebner NA, D’andrea D, Krzywon A, Shim SR, Baltzer PA, Renard-Penna R. Reliability of serial prostate magnetic resonance imaging to detect prostate cancer progression during active surveillance: a systematic review and meta-analysis. European urology. 2021 Nov 1;80(5):549-63.
12. Tschudi Y, Pollack A, Punnen S, et al. Automatic Detection of Prostate Tumor Habitats using Diffusion MRI. Sci Rep. 2018;8(1):16801.
13. Isensee F. et al. nnU-Net: a self-configuring method for deep learning-based biomedical image segmentation. Nature methods 18, 203-211, doi: 10.1038/s41592-020-01008-z (2020).
14. Algohary A, Zacharaki EI, Breto AL, Alhusseini M, Wallaengen V, Xu IR, Gaston SM, Punnen S, Castillo P, Pattany PM, Kryvenko ON, Spieler B, Abramowitz MC, Dal Pra A, Ford JC, Pollack A, Stoyanova R. Uncovering Prostate Cancer Aggressiveness Signal in T2-weighted MRI through a Deep Learning-based Normalization Technique, NMR in Biomedicine, in press.
15. Simeth J, Jiang J, Nosov A, Wibmer A, Zelefsky M, Tyagi N, Veeraraghavan H. Deep learning‐based dominant index lesion segmentation for MR‐guided radiation therapy of prostate cancer. Medical Physics. 2023 Mar 1.
16. Saha A, Hosseinzadeh M, Huisman H. End-to-end prostate cancer detection in bpMRI via 3D CNNs: effects of attention mechanisms, clinical priori and decoupled false positive reduction. Medical image analysis. 2021 Oct 1;73:102155.
17. Peng H, Long F, Ding C. Feature selection based on mutual information criteria of max-dependency, max-relevance, and min-redundancy. IEEE Transactions on Pattern Analysis and Machine Intelligence, vol. 27, no. 8, pp. 1226-1238, Aug. 2005, doi: 10.1109/TPAMI.2005.159.
Figures