0858
Enhancing Prognosis Prediction for Lung Cancer Patients with Brain Metastasis by Combining Brain MR and Lung CT Radiomic Features1Department of Biomedical Imaging and Radiological Sciences, National Yang Ming Chiao Tung University, Taipei, Taiwan, 2Department of Neurosurgery, Neurological Institute, Taipei Veterans General Hospital, Taipei, Taiwan, 3School of Medicine, National Yang Ming Chiao Tung University, Taipei, Taiwan, 4Department of Neurosurgery, Kaohsiung Veterans General Hospital, Kaohsiung, Taiwan, 5Department of Radiology, Taipei Veterans General Hospital, Taipei, Taiwan
Synopsis
Keywords: Diagnosis/Prediction, Radiomics, Brain metastasis
Motivation: Control of metastatic and primary tumors has been identified as prognostic factors for lung cancer patients with brain metastasis. However, prognosis prediction by combining imaging features of metastatic and primary tumors was less explored.
Goal(s): This study investigated the prediction efficacy based on image traits of brain metastasis and primary lung cancer.
Approach: The radiomic features separately extracted from brain MRI and chest CT images were merged to build the survival prediction models.
Results: The proposed prediction model showed superior performance compared to the models based on a single modality in lung cancer with brain metastasis.
Impact: This study suggested that survival prediction can be enhanced by combining features of brain metastasis MRI and lung cancer CT. Imaging characteristics of both primary and secondary (metastatic) tumors are valuable for prognostic prediction in lung cancer with brain metastasis.
Background and Purpose
Approximately 50% of lung cancer patients were observed with distant metastasis at first examination, in which more than 45% are brain metastasis. [1] The one-year survival rate of lung cancer patients with brain metastasis is 28.2%. [1] Xue et al. observed a wide range of prognoses, from 1 to 120 months, among lung cancer patients with brain metastasis. [2] Developing the overall survival (OS) prediction model can benefit the clinical management of lung cancer patients with brain metastasis. The control of brain metastasis and primary tumor have been proposed to be correlated with prognosis. [3, 4] However, the potential prediction enhancement achieved by combining features of metastasis and primary tumor was unexplored. The aim of this study was to investigate the efficacy of prognosis prediction achieved by combining the brain MRI and chest CT features in lung cancer.Materials and Methods
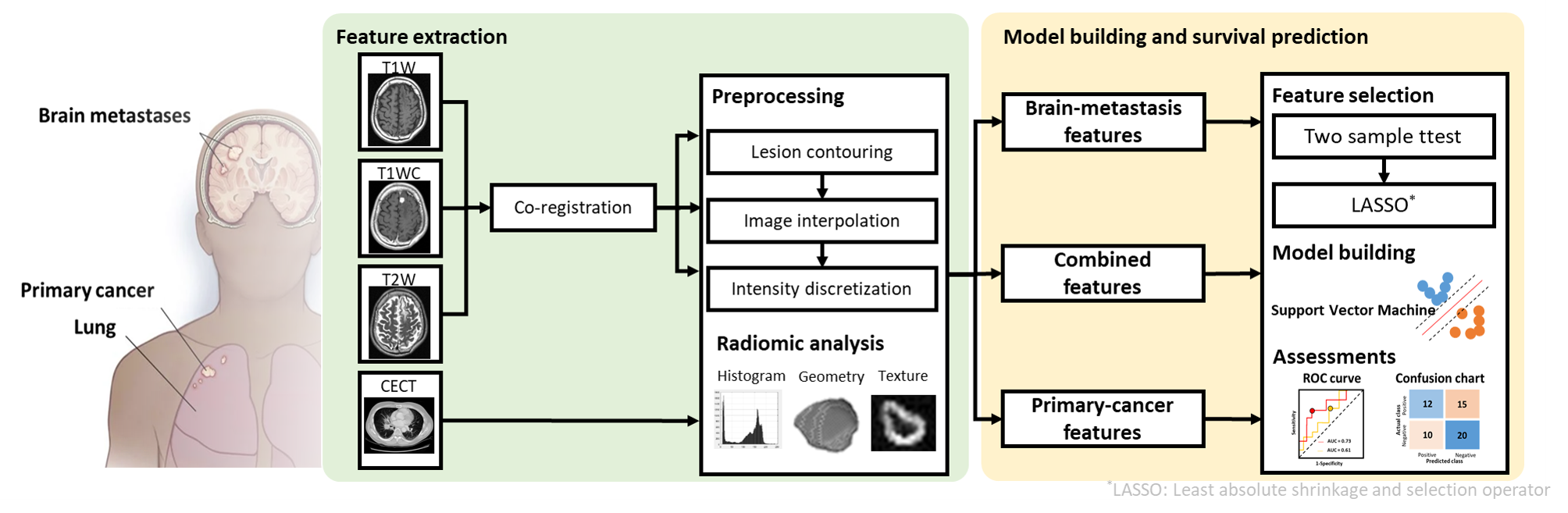
This study retrospectively recruited 237 lung cancer subjects with brain metastasis from Taipei Veterans General Hospital. Routine brain magnetic resonance images (MRIs) were acquired from each subject, including T1-weighted (T1W, TR/TE=500/9 ms), contrast-enhanced T1-weighted (T1WC, TR/TE=500/9 ms), and T2-weighted (T2W, TR/TE=4000/109 ms) images. Additionally, the subjects received contrast-enhanced chest computed tomography (CECT) scans.Image preprocessing and feature extraction were conducted using our customized platform (Figure 1). [5] The T1W and T2W images were co-registered with the T1WC image. [6] An experienced radiologist delineated the regions of brain metastasis and primary lung tumors. The resolution and voxel values of the MRIs and CECT were adjusted using interpolation and intensity discretization, followed by radiomic analysis. Through radiomic analysis, 1765 brain-metastasis and 593 primary-cancer features were extracted from MRIs and CECT, respectively. In this study, 20% of dataset was held out and assigned as the test dataset (N=47).
To identify the distinct predictors between patients with good (OS > 12 months) and poor prognosis (OS ≤ 12 months), the two-sample t-test and least absolute shrinkage and selection operator (LASSO) regression were employed to the combined (brain-metastasis + primary-cancer), brain-metastasis, and primary-cancer feature sets. [7] These predictors were employed to build three Support Vector Machine (SVM) models, respectively. The performance of the three models were evaluated with ROC curves and confusion matrices. Furthermore, the comparisons of area under the ROC curves (AUC), sensitivity, specificity, accuracy between the three models were conducted using permutation tests.
Results and Discussion
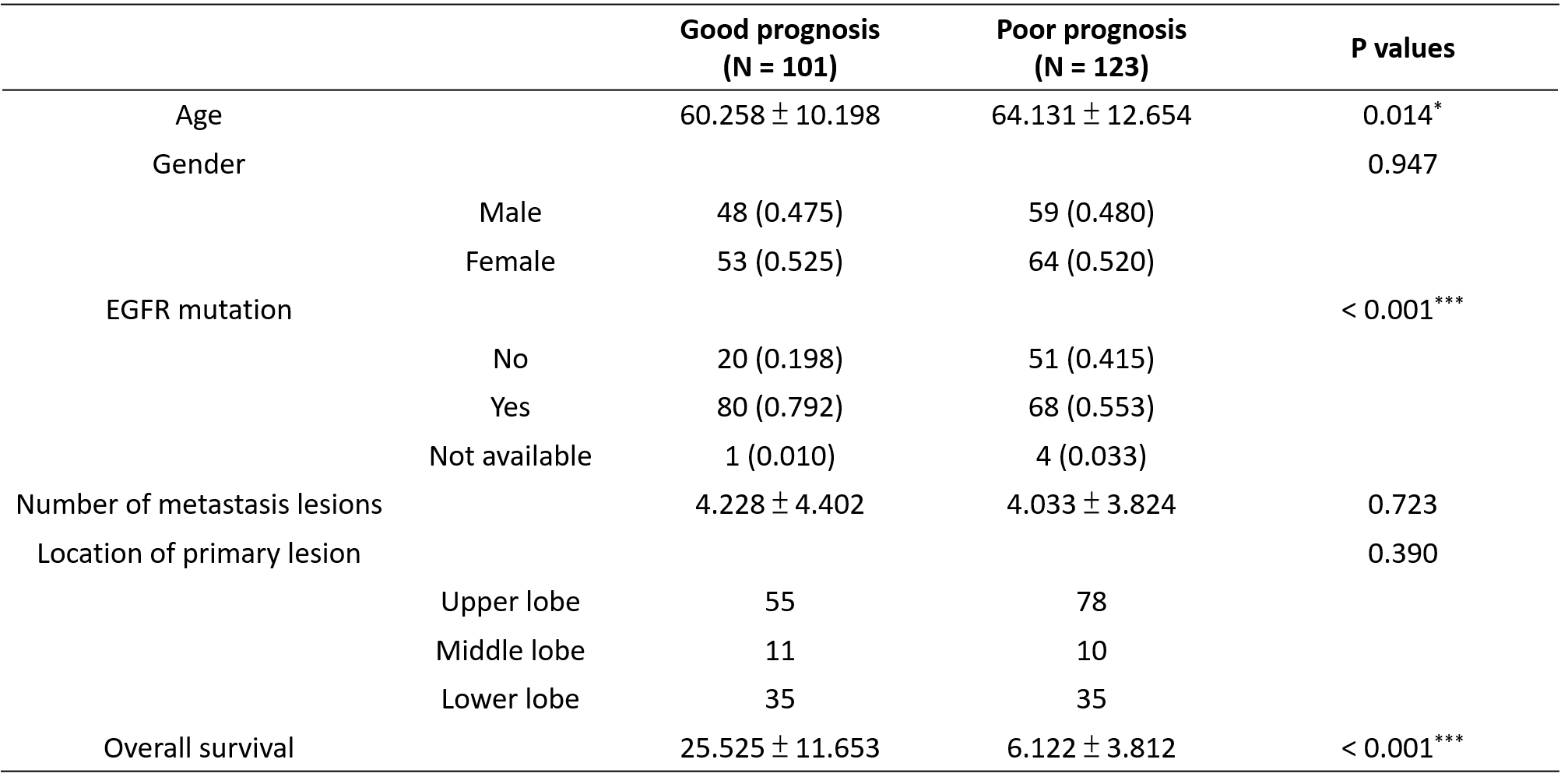
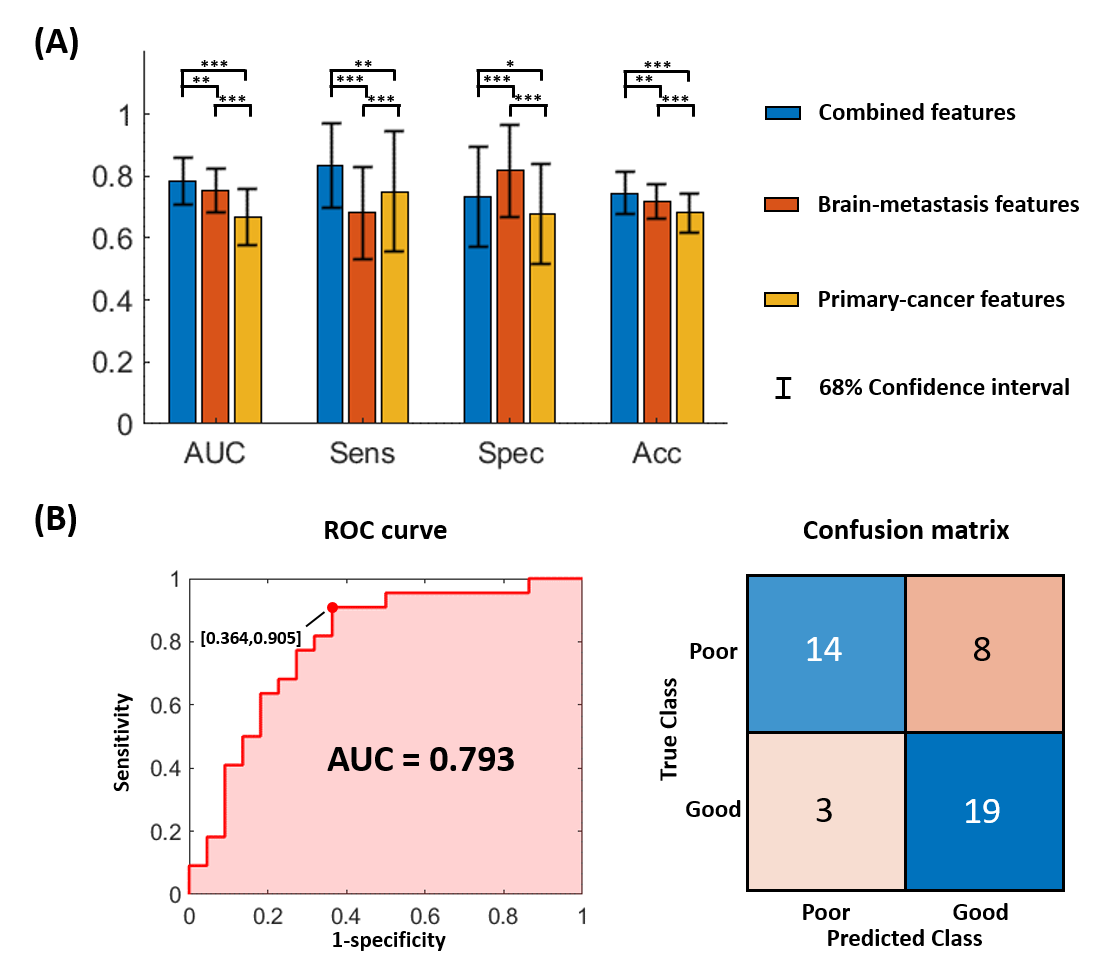
This study included 101 patients with good prognosis and 123 with poor prognosis. The two groups showed significant difference in age and epidermal growth factor receptor (EGFR) mutation status (Table 1). In lung cancer patients with brain metastasis, a young age and EGFR mutation have been associated with a good prognosis. [8, 9]Figure 2 displays the comparisons of model performance using permutation tests. The model based on combined features showed the highest AUC (0.793), sensitivity (0.905), and accuracy (0.75), indicating that the combination of brain-metastasis and primary-cancer information can improve prognosis prediction performance. Furthermore, the model based on brain-metastasis features showed better performance compared to the one based on primary-cancer features. Cancer cells that metastasize to brain parenchyma may trigger neuro-inflammation and lead to symptoms such as fatigue, sleep disturbance, and decreased appetite. [10] The association between brain-metastasis induced neuro-inflammation and prognosis has been proposed. [11]
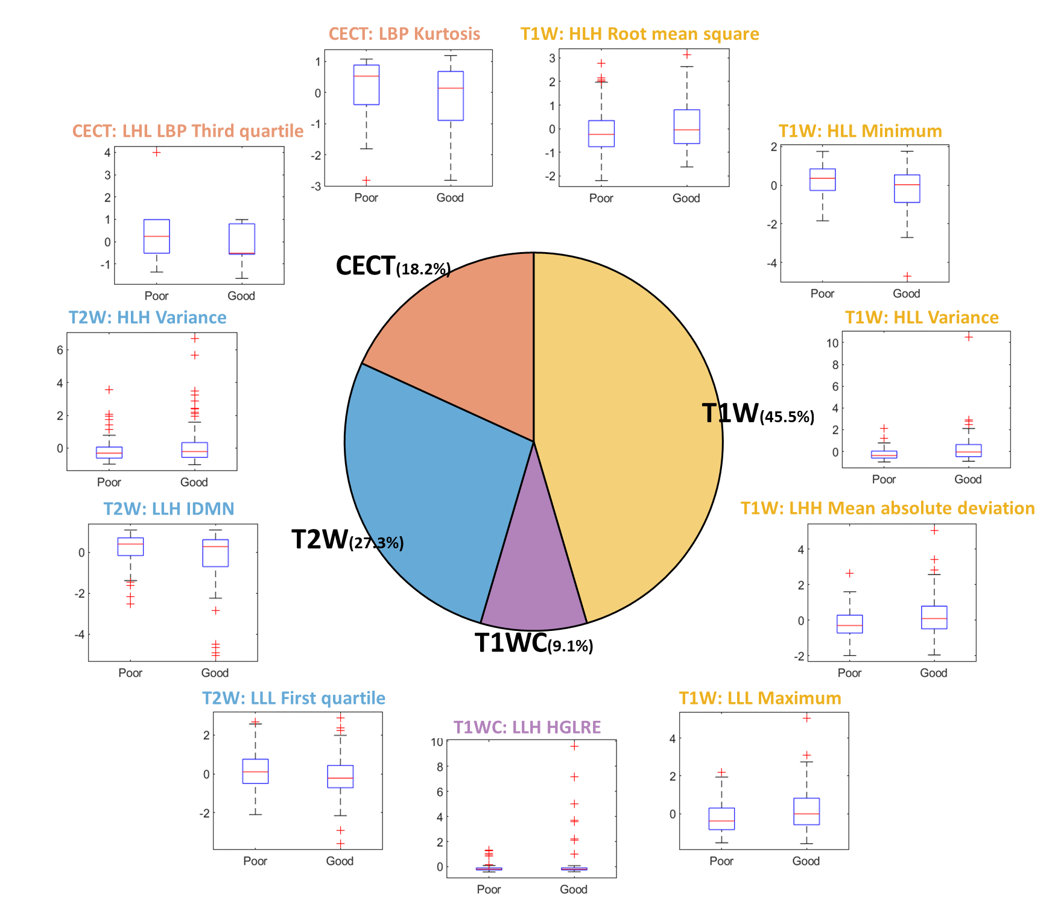
Eleven predictors for the model based on combined features contained 5, 1, 3, and 2 features from T1W, T1WC, T2W, and CECT images, respectively (Figure 3). The 81.8% of predictors were derived from MRIs, reflecting the strong association between brain-metastasis lesions and prognosis. [11] Most of the T1W- and T2W-derived predictors were histogram features, with the exception of T2W-derived LLH Inverse Difference Moment Normalized (IDMN). The predictors extracted from T1WC and CECT images were textural features, potentially indicating importance of the enhanced vascular information after injection of contrast agent.
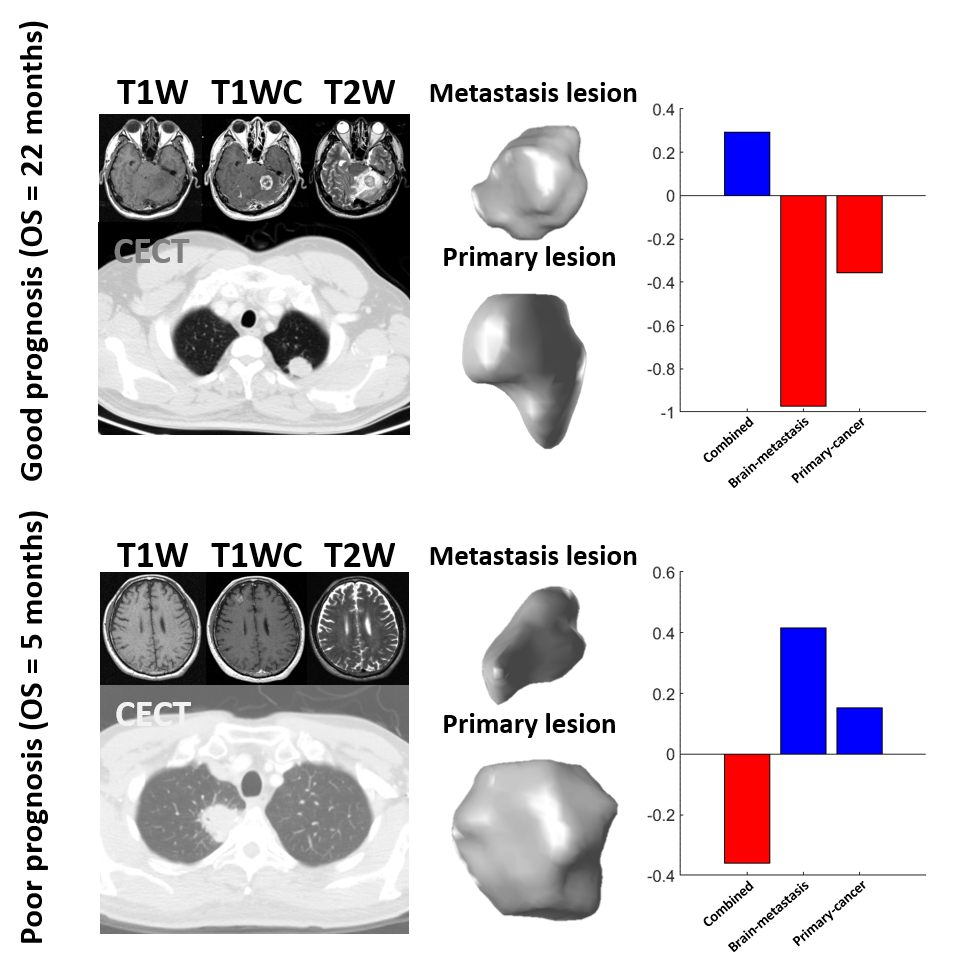
Figure 4 illustrates two lung cancer patients with brain metastasis. Both patients were predicted correctly only by the combined model, indicating that the combined model demonstrated high precision in assessing the combination of brain-metastasis and primary-cancer information.
Conclusions
In this study, we evaluated the improvement of performance achieved by combining the features of brain metastasis and primary cancer. The absence information regarding the primary cancer may lead to an incorrected prediction. Therefore, this study suggested that radiomic features extracted from both metastasis and primary tumors are necessary in prognosis prediction for lung cancer patients with brain metastasis.Acknowledgements
This work was supported by Veterans General Hospitals and University System of Taiwan Joint Research Program (VGHUST112-G1-3-3), and National Science and Technology Council (NSTC 112-2314-B-A49-060).References
1. Niu, F.Y., et al., Distribution and prognosis of uncommon metastases from non-small cell lung cancer. BMC Cancer, 2016. 16: p. 149.
2. Xue, J., et al., The role of brain metastases in patients with pulmonary adenocarcinoma: a retrospective study. Ann Palliat Med, 2021. 10(12): p. 12262-12272.
3. Liao, C.Y., et al., Enhancement of Radiosurgical Treatment Outcome Prediction Using MRI Radiomics in Patients with Non-Small Cell Lung Cancer Brain Metastases. Cancers (Basel), 2021. 13(16).
4. Su, S., et al., Might radiation therapy in addition to chemotherapy improve overall survival of patients with non-oligometastatic Stage IV non-small cell lung cancer?: Secondary analysis of two prospective studies. BMC Cancer, 2016. 16(1): p. 908.
5. Lu, C.F., et al., Machine Learning-Based Radiomics for Molecular Subtyping of Gliomas. Clin Cancer Res, 2018. 24(18): p. 4429-4436.
6. Challis, J.H., A procedure for determining rigid body transformation parameters. Journal of Biomechanics, 1995. 28(6): p. 733-737.
7. Tibshirani, R., Regression Shrinkage and Selection via the Lasso. Journal of the Royal Statistical Society. Series B (Methodological), 1996. 58(1): p. 267-288.
8. Baek, M.Y., et al., Epidermal growth factor receptor mutation and pattern of brain metastasis in patients with non-small cell lung cancer. Korean J Intern Med, 2018. 33(1): p. 168-175.
9. Yuan, J., et al., Prognosis of lung cancer with simple brain metastasis patients and establishment of survival prediction models: a study based on real events. BMC Pulm Med, 2022. 22(1): p. 162.
10. Niccolai, L.M. and J.L. Rexer, Chapter 14 - Cognitive Impairment in Lung Cancer and Brain Metastases, in Lung Cancer Rehabilitation, A. Cristian, Editor. 2023, Elsevier. p. 177-184.
11. Doron, H., T. Pukrop, and N. Erez, A Blazing Landscape: Neuroinflammation Shapes Brain Metastasis. Cancer Res, 2019. 79(3): p. 423-436.
Figures