0857
Identification of intrinsic imaging phenotype for endometrial carcinoma based on multi-modality MRI using multi-Omics clustering algorithm1Jiangsu Province Hospital, the First Affiliated Hospital With Nanjing Medical University, Nanjing, China, 2Central Research Institute, UIH Group, Shanghai, China
Synopsis
Keywords: Diagnosis/Prediction, Pelvis, Imaging phenotype
Motivation: Heterogeneity of endometrial carcinoma (EC) leads to differences in prognosis among different patients. The method of unsupervised machine learning can classify tumors into different subtypes by identifying heterogeneity and similarity in radiomics features, which may have the ability of preoperative risk stratification.
Goal(s): To identify the intrinsic imaging phenotype for EC using multi-modality MR-based radiomics features.
Approach: Ten multi-omics clustering methods were used for imaging phenotypes identification and reached a consensus.
Results: Among the three identified imaging phenotypes, multiple pathological features and disease-free survival time showed significant differences.
Impact: Based on multi-modality MRI using an unsupervised machine learning approach to classify EC into different imaging phenotypes, which were associated with clinicopathological features and prognosis, and can be used for preoperative risk stratification.
Introduction
The endometrial carcinoma (EC) has significant phenotypic heterogeneity[1]. The radiomics features based on MRI have been widely studied and confirmed to reflect EC heterogeneity, and are correlated with the clinicopathological features[2, 3]. However, most of the previous studies were performed in a supervised fashion, to our knowledge there has been no work done to identify radiomics subtypes of EC in an unsupervised approach. In this study, the method of unsupervised learning was used to extract useful information from image data to identify imaging phenotypes. The tumors with the most similar imaging features were divided into one subtype by clustering method, to increase the ability to describe tumors more comprehensively[4, 5]. We analyzed the differences in pathological manifestations and clinical prognosis among different subtypes.Methods
A total of 227 patients diagnosed with EC in our hospital from January 2018 to June 2023 were enrolled in this study. All of them underwent MRI including T2W, diffusion-weighted imaging, apparent diffusion coefficient map, and contrast-enhanced T1W imaging before surgery. Patients’ clinicopathological features, prognosis, and disease-free survival (DFS) time were collected. The tumor region of interest on 4 MR sequences was manually segmented section by section. The radiomics features were extracted from 4 MR modalities. The dimension reduction of radiomics features were conducted by uniform manifold approximation and projection (UMAP), and 10 multi-omics clustering methods were conducted to identify the phenotypes and reached a consensus. The clinicopathological features were compared among the different phenotypes using χ2 for categorical data and the Kruskal-Wallis test for continuous data, In addition, the DFS of 75 patients (diagnosed between January 2018 and October 2020) was also compared using Kaplan-Meier analysis.Results
Consensus clustering showed a sharp decrease in the relative change in area under the conditional density function curve at a k value of 3. The EC was divided into 3 phenotypes, 72 patients belonged to phenotype 1, 105 patients belonged to phenotype 2, and 50 patients belonged to phenotype 3. The clustering result of the three phenotypes is shown in Figure 1, and differences in the distribution of radiomics features among the three phenotypes can be seen clearly (Figure 2). Clinicopathological features grouped into phenotypes are summarized in Figure 3 (Table 1). The median follow-up time of 75 patients was 36.0 months; 6 recurrences were recorded (median DFS 9.5 months). Deep myometrial invasion (MI) is associated with higher recurrence risk (5/17 vs. 1/58, p=0.002, median DFS: 30.5 months). Patients with endometrioid subtype have a lower recurrence risk (4/72 vs. 2/3, p=0.016). Other clinicopathological features in our study did not show a significant correlation with recurrence. Patients with phenotype 3 have larger lesion volumes (p<0.001), and higher frequency of cervical stroma invasion (CSI) (22.0%, p<0.001), deep MI (52.0%, p<0.001), and lymphovascular space invasion (LVSI) (28.0%, p=0.003). Phenotype 3 lesions showed higher histopathological grade (p<0.001), and pathological subtypes such as serous, clear cell, and undifferentiated are also more common (14.0%, p=0.006). The frequency of these pathological features was lowest in phenotype 1. Survival analysis showed that phenotype 3 had the highest risk of recurrence compared with phenotypes 1 and 2, and there was a significant difference between phenotype 1 and 3 (p=0.049, Figure 4). The MR images of three patients with different imaging phenotypes are shown in Figure 5.Discussion
To our knowledge, this work is the first application of unsupervised machine learning methods in identifying imaging phenotypes of EC. In our study, three EC imaging phenotypes were identified based on MRI radiomics features. Multiple pathological features, including CSI, MI, LVSI, FIGO, histopathologic subtype, and histopathologic grade, showed significant differences among the three imaging phenotypes. This finding suggested that image-based classification has a real biological basis. In addition, the Kaplan-Meier curve showed the differences in DFS among the three imaging phenotypes and suggested the significant differences between phenotype 1 and phenotype 3. Patients classified as phenotype 3 had a higher risk of recurrence and a shorter DFS time. It can be seen that imaging phenotype is valuable in further improving our description of tumor heterogeneity and can be used for preoperative risk stratification.Conclusion
The intrinsic imaging phenotypes were correlated with clinicopathological features, which might be a potential biomarker for EC diagnosis and treatment guidance.Acknowledgements
No acknowledgement found.References
[1] Levine D A. Integrated genomic characterization of endometrial carcinoma [J]. Nature, 2013, 497(7447): 67-73.
[2] Jacob H, Dybvik J A, Ytre-Hauge S, et al. An MRI-Based Radiomic Prognostic Index Predicts Poor Outcome and Specific Genetic Alterations in Endometrial Cancer [J]. J Clin Med, 2021, 10(3):
[3] Yan B C, Li Y, Ma F H, et al. Preoperative Assessment for High-Risk Endometrial Cancer by Developing an MRI- and Clinical-Based Radiomics Nomogram: A Multicenter Study [J]. Journal of magnetic resonance imaging : JMRI, 2020, 52(6): 1872-82.
[4] Haldar D, Kazerooni A F, Arif S, et al. Unsupervised machine learning using K-means identifies radiomic subgroups of pediatric low-grade gliomas that correlate with key molecular markers [J]. Neoplasia, 2023, 36(
[5] Perez-Johnston R, Araujo-Filho J A, Connolly J G, et al. CT-based Radiogenomic Analysis of Clinical Stage I Lung Adenocarcinoma with Histopathologic Features and Oncologic Outcomes [J]. Radiology, 2022, 303(3): 664-72.Figures
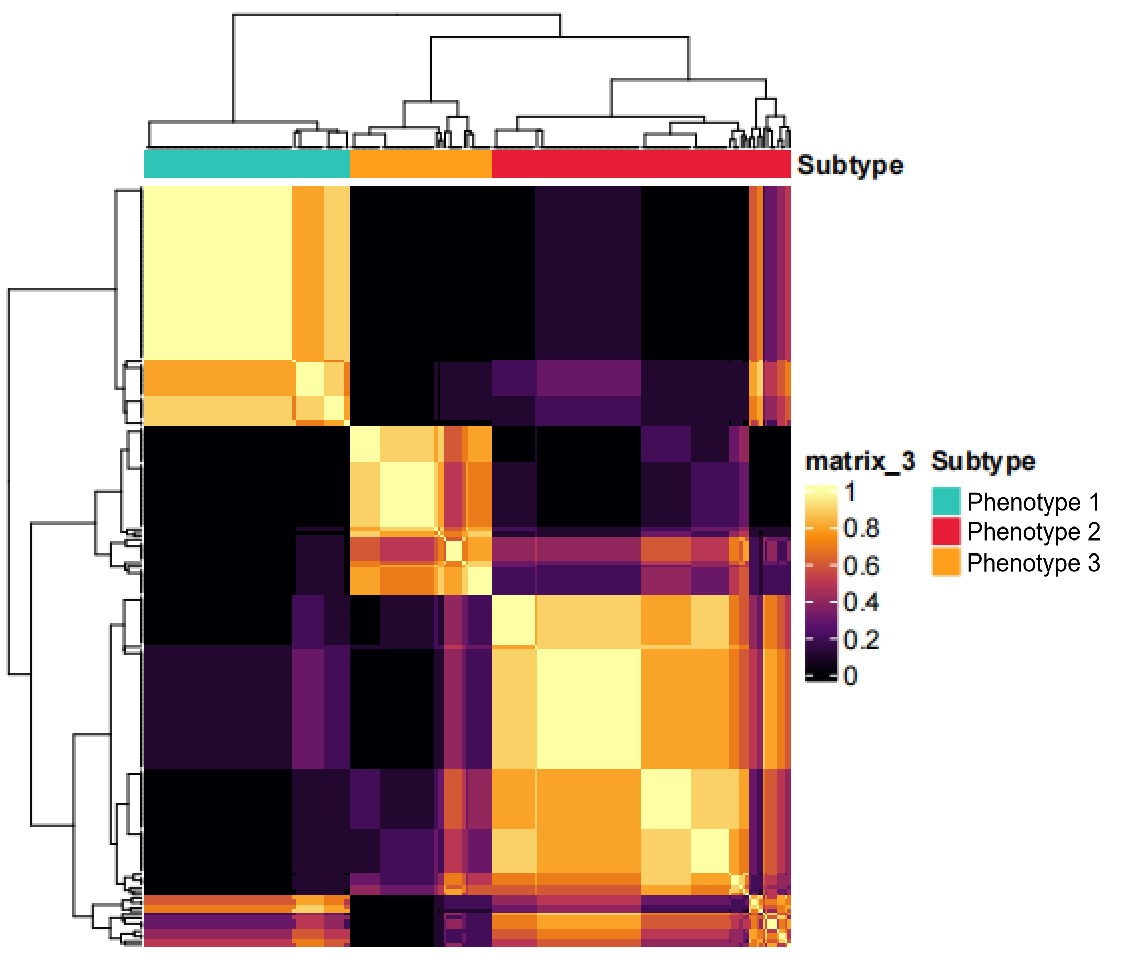
Figure 1: The consensus clustering of the three imaging phenotypes based on ten multi-omics clustering methods.
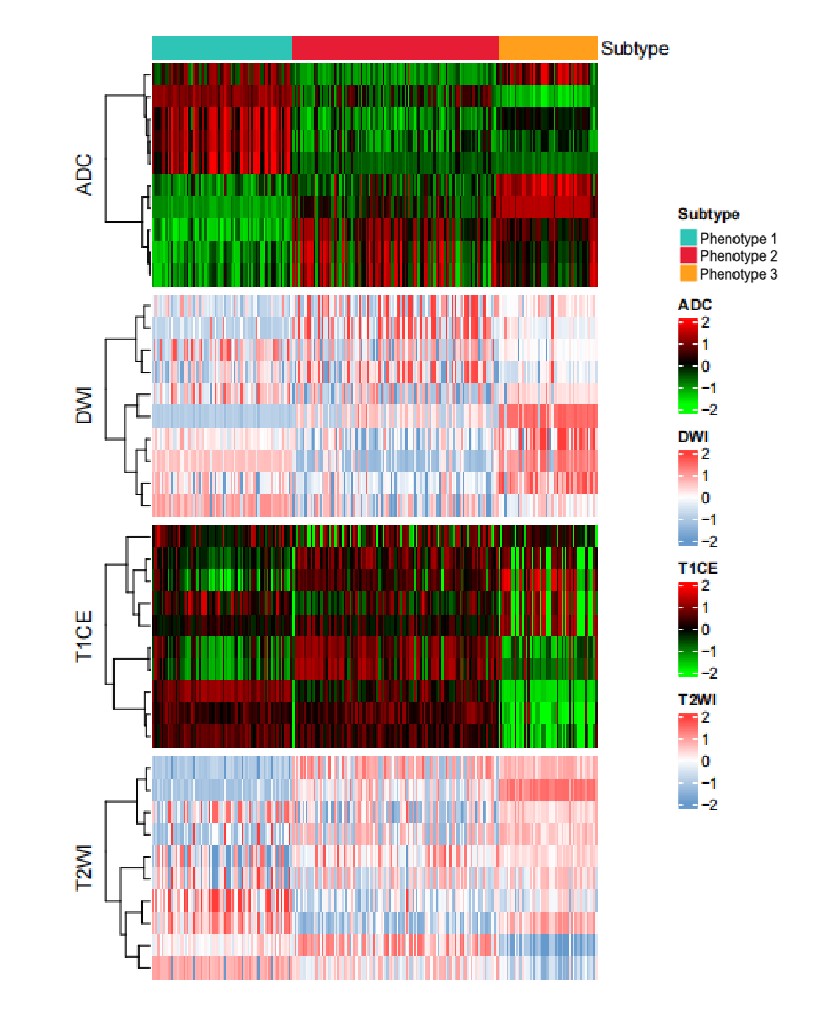
Figure 2: Differences in the distribution of multi-modality MRI radiomics features among the three imaging phenotypes can be seen clearly.
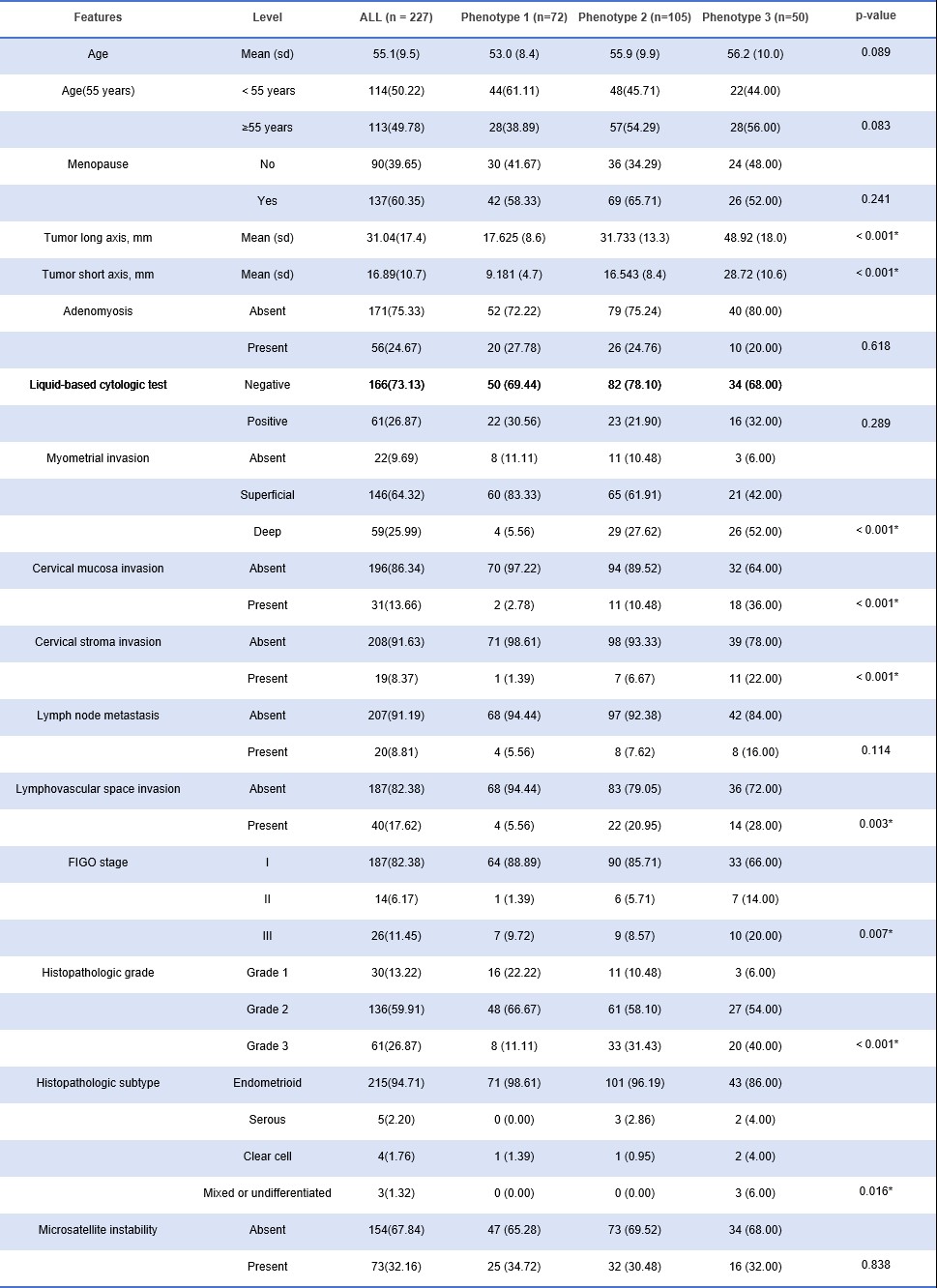
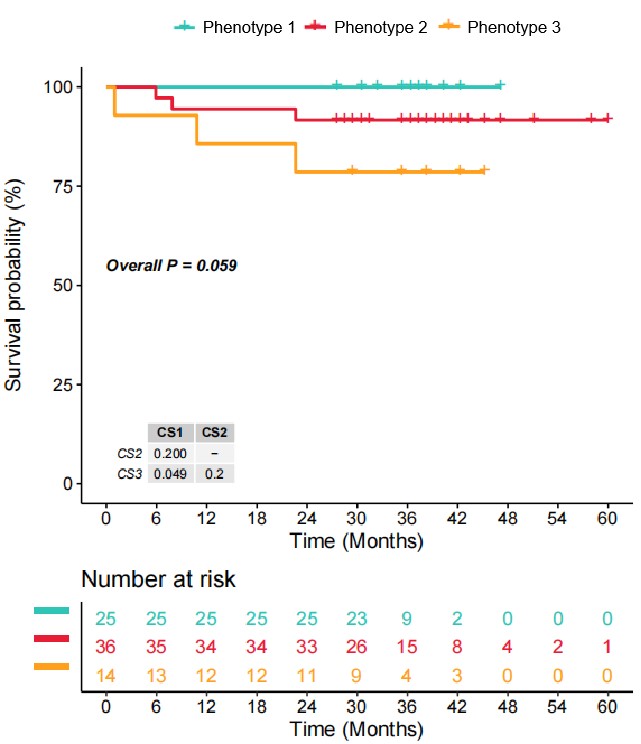
Figure 4: Three-year disease-free survival for each of the imaging phenotypes of 75 patients (diagnosed as EC between January 2018 and October 2020).
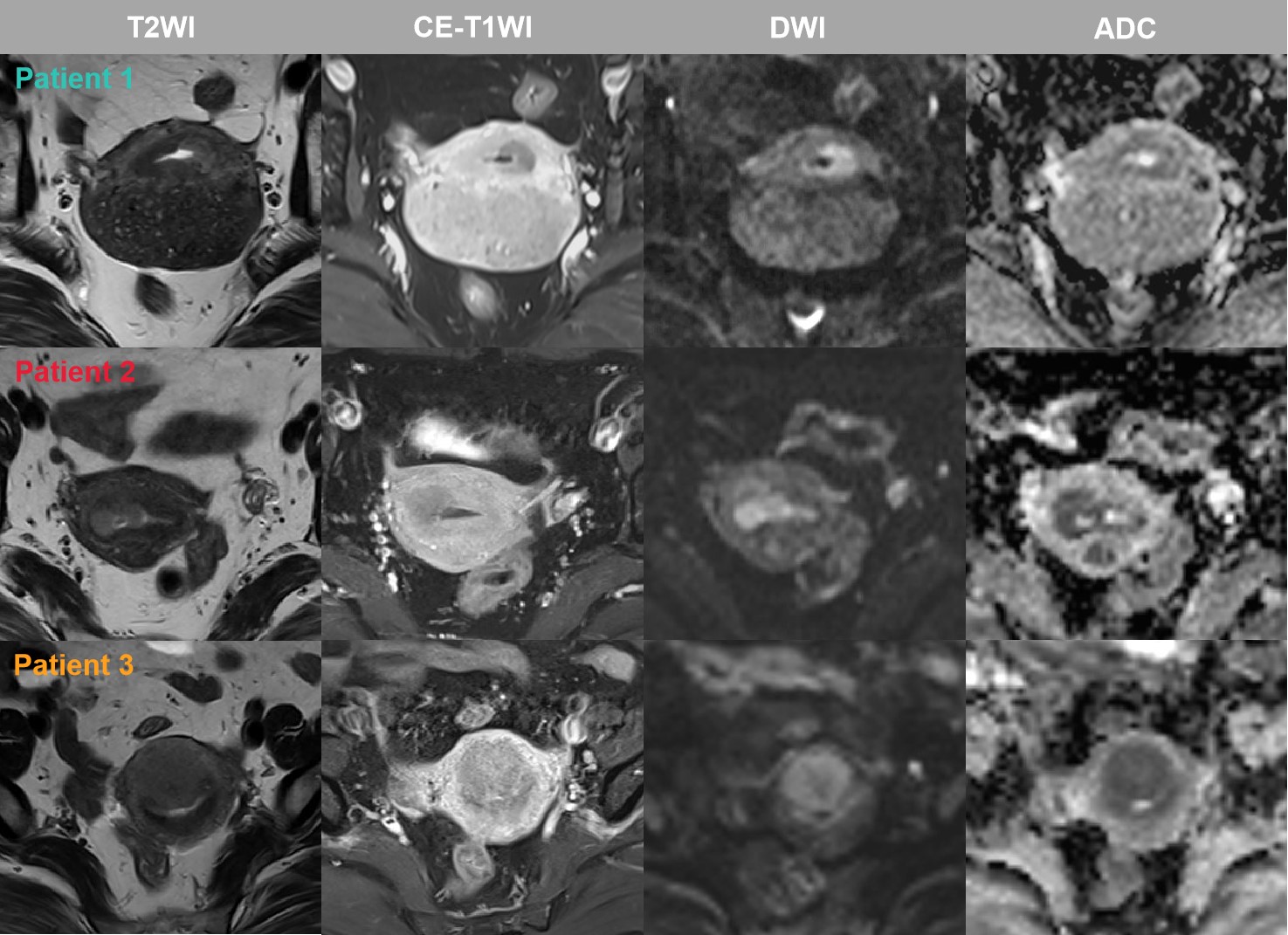
Figure 5: The MR images of three patients with different imaging phenotypes
Patient 1 (phenotype 1): Endometrioid carcinoma; superficial MI; LVSI (-); CSI (-); histopathologic grade 1; FIGO I; DFS: 36 months; without recurrence
Patient 2 (phenotype 2): Endometrioid carcinoma; deep MI; LVSI (-); CSI (-); histopathologic grade 3; FIGO I; DFS: 29 months; without recurrence
Patient 3 (phenotype 3): Endometrioid carcinoma; deep MI; LVSI (-); CSI (+); histopathologic grade 3; FIGO II; DFS: 1 months; with recurrence