0856
Deep learning models for predicting responses to neoadjuvant systemic therapy in triple-negative breast cancer using pre-treatment MRI1Department of Imaging Physics, The University of Texas MD Anderson Cancer Center, Houston, TX, United States, 2Department of Breast Imaging, The University of Texas MD Anderson Cancer Center, Houston, TX, United States, 3Department of Biostatistics, The University of Texas MD Anderson Cancer Center, Houston, TX, United States, 4Department of Breast Medical Oncology, The University of Texas MD Anderson Cancer Center, Houston, TX, United States
Synopsis
Keywords: Diagnosis/Prediction, Cancer
Motivation: Neoadjuvant systemic therapy (NAST) followed by surgery is the standard of care for triple-negative breast cancer (TNBC) patients. However, only approximately half of these patients achieve pathological complete response (pCR).
Goal(s): To build a prediction model to identify non-pCR patients before the initiation of NAST.
Approach: We evaluated multiple prediction models using pretreatment multi-parametric MRI from a cohort of 282 TNBC patients.
Results: Our findings revealed that combined with clinical information, the best-performing model achieved an AUC of 0.74 on an independent testing set. We further observed that the performance of our models is not sensitive to the voxel selections in tumor segmentation.
Impact: Deep learning models for predicting pathological complete response to neoadjuvant systemic therapy of triple-negative breast cancer were developed using baseline multi-parametric MRI data and clinical information and achieved an AUC of 0.74 on the independent testing dataset.
Introduction:
Triple-negative breast cancer (TNBC) is an aggressive subtype of breast cancer and is refractory to targeted therapy1. Surgery preceded by neoadjuvant systemic therapy (NAST) has been the standard of care treatment for locally advanced TNBC. Patients who achieve a pathological complete response (pCR) to NAST have better recurrence-free survival rates than non-pCR patients. However, only about 50-60% of patients achieve pCR2, defined as the absence of invasive residual disease by surgical pathology after the completion of NAST. An accurate prediction of pCR at an early timepoint is currently not possible but could be valuable for more personalized treatment of the patients, including potentially sparing non-pCR patients from ineffective chemotherapy. In this study, we investigated multiple deep learning (DL) models for pCR prediction with different data inputs including dynamic contrast enhanced (DCE) MRI, diffusion weighted imaging (DWI), and clinical information that were acquired before the start of the patients’ NAST.Methods:
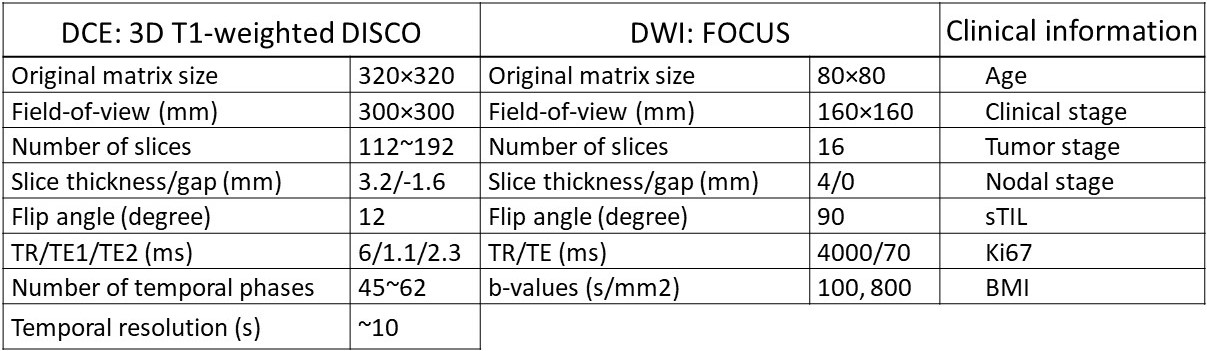
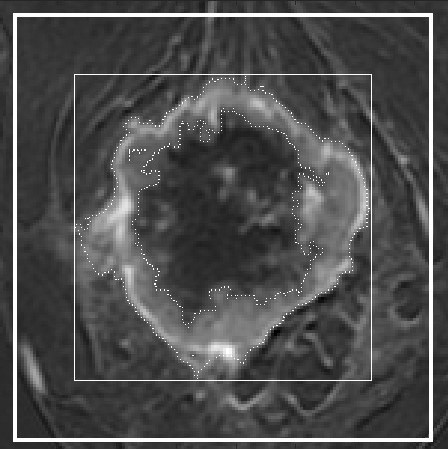
Datasets: Our study included 282 biopsy-confirmed stage I-III TNBC patients. All patients were enrolled in an IRB approved prospective clinical trial (NCT02276443) and underwent multiparametric MRI prior to the initiation of NAST that included DCE and DWI. The primary scan parameters of these two sequences are listed in Table 1. For the DL model development, we used the subtraction image (labelled as DCE) between the arterial phase at 2.5 minute after the contrast agent injection and baseline phase of the DCE-MRI images and the b=800 s/mm2 image (labelled as DWI) as the image input. For both DCE and DWI, manual segmentation by two experienced breast radiologists3 was used as reference masks for tumor voxels. The categorical data, such as tumor stage, in the clinical information were converted into numerical values. Image data were self-normalized at the subject level, and clinical information was normalized at the group level.Models: We systematically investigated the pCR prediction performance with the following variations : (1) Two different 3D DL networks: ResNet18 and ResNeXt504; (2) tumor volume preprocessing: normalized (to the median tumor matrix size) and original tumor matrix size; (3) tumor containing masks (Figure 1): voxels within reference masks of tumors; voxels within the bounding box of the reference masks; and voxels within an enlarged bounding box (dilated by 5 voxels along the top, bottom, left, and right sides) of the reference masks; (4) input channel(s): DCE; DWI; DCE + DWI; DCE + DWI + clinical information. In total, 48 variations of the prediction models were evaluated.
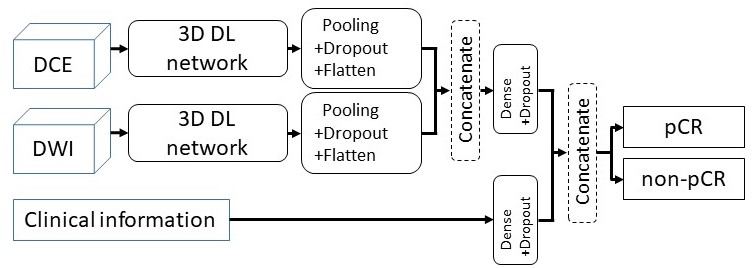
The dataset was randomly split into six folds, with 47 subjects per fold. A five-fold cross validation was applied for model training (using four folds) and validation (using the remaining fold), while the sixth fold was reserved for independent testing. The percentage of pCR cases among the entire cohort was 47%, and the same pCR ratio was maintained in each fold. The model structure is illustrated in Figure 2.
Statistics: For each of the 48 prediction models, the AUCs on the testing dataset were averaged over the 5-fold classifiers as the model's performance. These AUCs were compared using ANOVA and post-hoc paired t-tests. α=0.05 was considered as the threshold for significance and was adjusted with Bonferroni correction for multiple comparisons.
Results and Discussion:
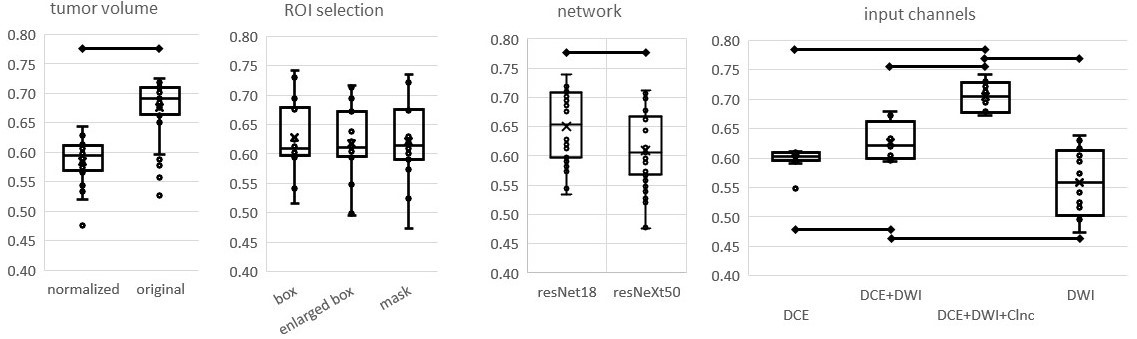
Of the 48 models, the model with ResNet18, the original tumor volume, using voxels within enlarged box, and with both DCE/DWI images and clinical information produced the best performance with an AUC of 0.74. At the group level, using the original data outperformed using the normalized tumor volume (Figure 3). Interestingly, different tumor containing masks did not affect the model performance, indicating that using the bounding box was as effective as using the manually segmented tumor mask, potentially obviating the need for contouring the exact tumor masks, which is tedious and time-consuming.Conclusion:
We have successfully developed a DL model for predicting pCR to NAST in TNBC using multiparametric MR images and clinical information that are available prior to the initiation of therapy. Our investigation has shown that an AUC of 0.74 was achieved in an independent testing dataset using a combination of DCE, DWI, and clinical information.Acknowledgements
This work was supported by the University of Texas MD Anderson Moon Shots Program and Robert D. Moreton Distinguished Chair Funds in Diagnostic Radiology. This study was supported by the NIH/NCI under award number P30CA016672.References
- Foulkes WD, Smith IE, Reis-Filho JS. Triple-Negative Breast Cancer. New England Journal of Medicine. 2010;363(20):1938-1948. doi: 10.1056/NEJMra1001389.
- Lee JS, Yost SE, Yuan Y. Neoadjuvant Treatment for Triple Negative Breast Cancer: Recent Progresses and Challenges. Cancers. 2020;12(6). doi: 10.3390/cancers12061404.
- Xu Z, Rauch DE, Mohamed RM, et al. Deep Learning for Fully Automatic Tumor Segmentation on Serially Acquired Dynamic Contrast-Enhanced MRI Images of Triple-Negative Breast Cancer. Cancers. 2023;15(19). doi: 10.3390/cancers15194829.
- He K, Zhang X, Ren S, Sun J. Deep residual learning for image recognition. Proc IEEE Conf Comput Vis Pattern Recognit. 2016:770-778. doi: 10.1109/CVPR.2016.90.
Figures