0855
Integrating radiomics, pathomics, and biopsy-adapted immunoscore for predicting distant metastasis in locally advanced rectal cancer1National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China, 2GE Healthcare China, Beijing, China
Synopsis
Keywords: Diagnosis/Prediction, Radiomics, Rectal cancer; Neoadjuvant chemoradiotherapy; Distant metastasis; Pathomics; Immunosocre
Motivation: Identifying high-risk patients for distant metastasis (DM) before treatment can facilitate the development of personalized neoadjuvant treatment and improve the prognosis of patients with locally advanced rectal cancer (LARC).
Goal(s): This study aimed to construct a predictive model that integrates radiological information at the macroscale and pathological information at the microscale to estimate the probability of DM in LARC patients after neoadjuvant chemoradiotherapy, using radiomics, pathomics, and biopsy-adapted immunoscore.
Approach: Feature selection and signature construction were performed using the least absolute shrinkage and selection operator (LASSO)-Cox analysis.
Results: The results demonstrated the effectiveness of the nomogram in identifying high-risk DM patients.
Impact: Incorporating multiscale information, including radiomics, pathomics, and the immune microenvironment, enhances the characterization of tumors and provides a robust model for identifying high-risk DM patients in LARC. This approach aids in the development of personalized neoadjuvant treatment strategies.
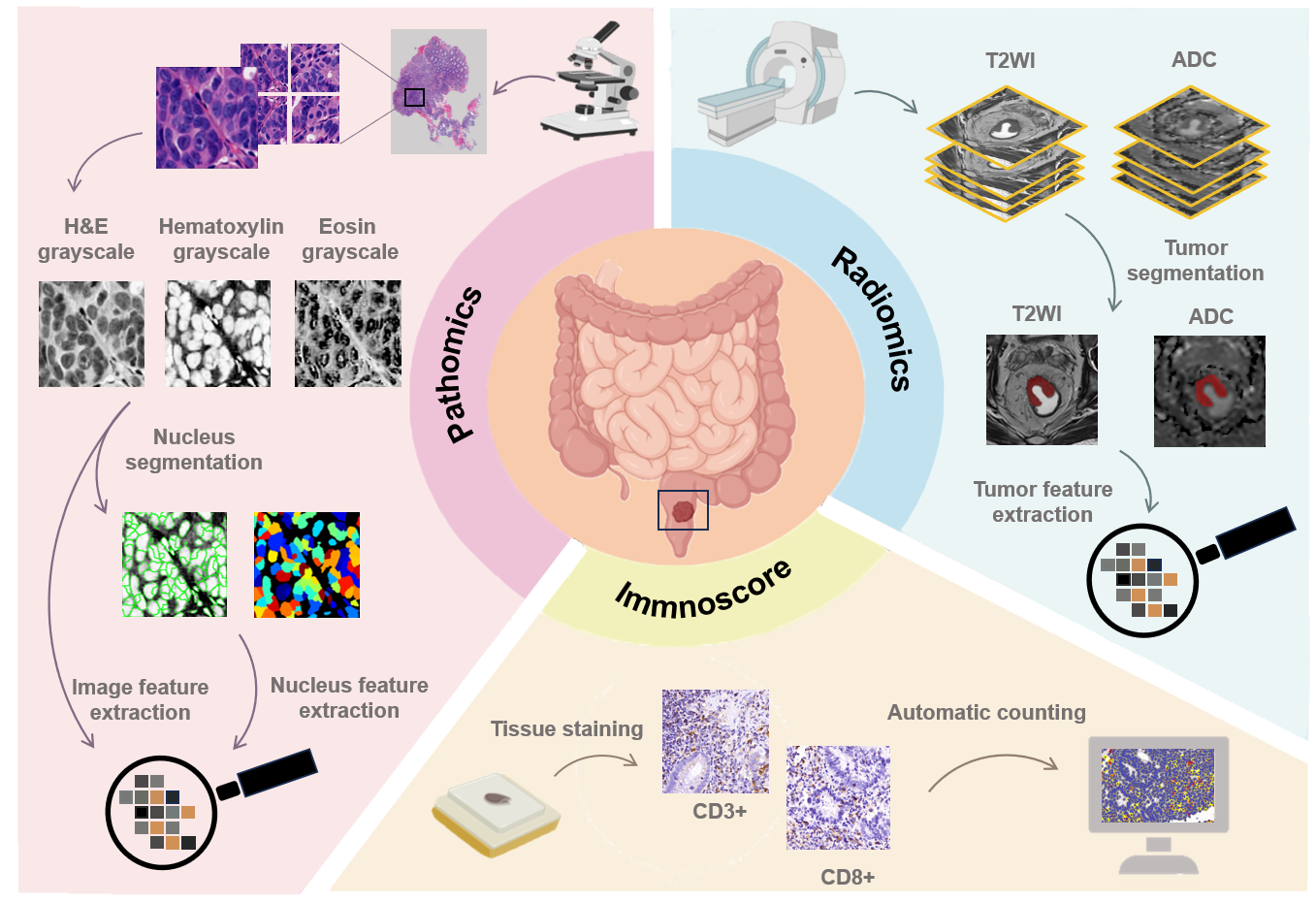
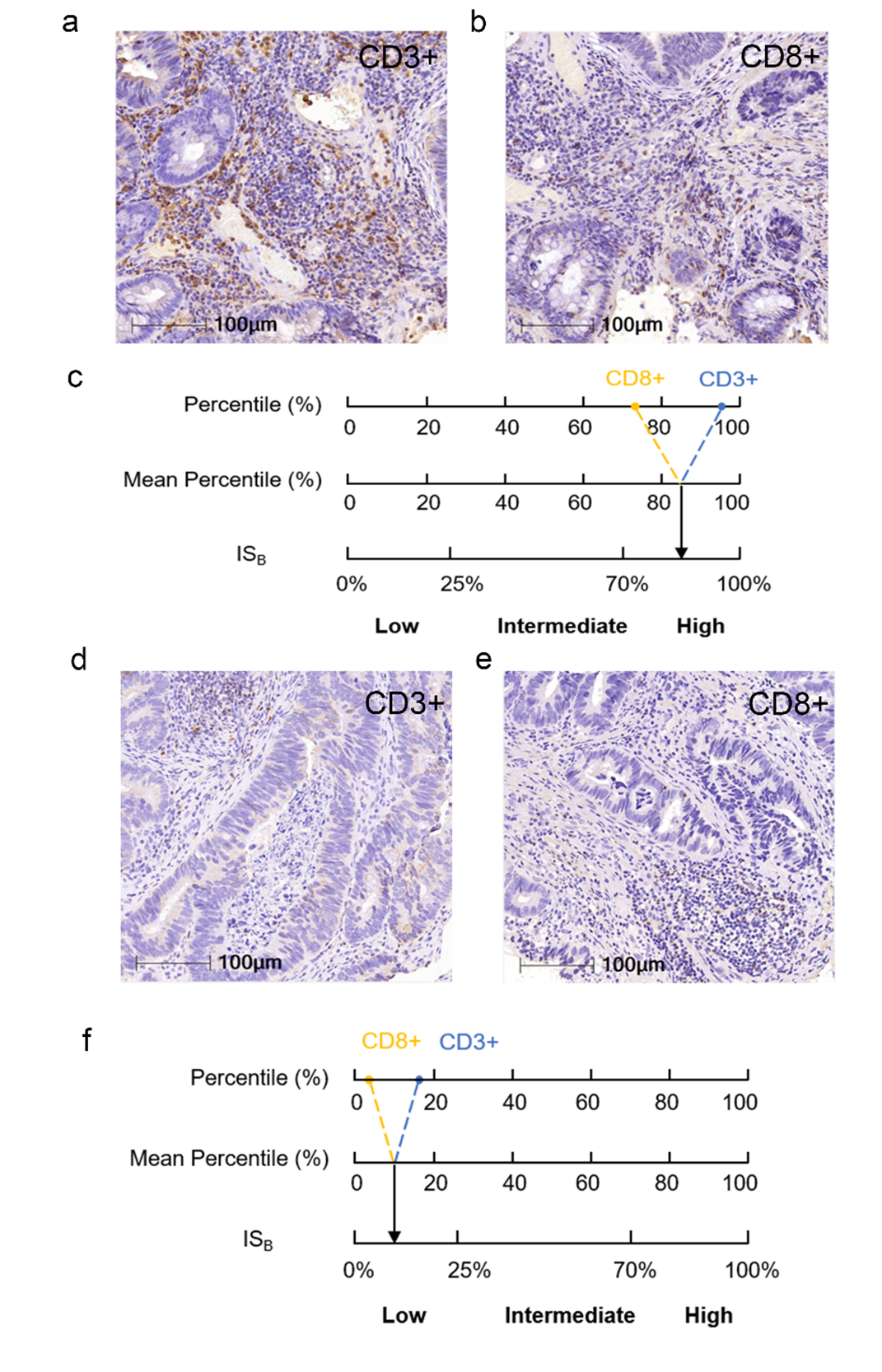
Materials and Methods: This retrospective study included 201 LARC patients (142 men, 59 women; mean age 54.5±10.6 years; range 23-79 years) who underwent NCRT and surgery. The median follow-up duration was 91 months (interquartile range, 82–113 months). Radiomics features were extracted from the gross tumor volume using T2-weighted images and apparent diffusion coefficient maps. Pathomics features including global pattern (features of the entire image) and local pattern (features of the tumor nuclei) were extracted from whole-slide images of hematoxylin and eosin-stained biopsy specimens using Cellprofiler software. ISB was calculated from the densities of CD3+ and CD8+ T cells in the tumor region using immunohistochemistry on biopsy specimens. CD3+ and CD8+ T cell densities in the tumor region of each patient were compared to that obtained in all patients and converted into percentile. Then, the mean of the two percentiles (CD3+ and CD8+ T cells) was translated into one of the three ISB categories: Low (0–25%), Intermediate (> 25–70%), and High (> 70–100%)5. Feature selection and signature construction were performed using the least absolute shrinkage and selection operator (LASSO)-Cox analysis. The nomogram's performance in predicting DMFS was assessed using the concordance index (C-index) and area under the receiver operating characteristic curve (AUC) of the time-independent receiver operating characteristic (ROC) curve.
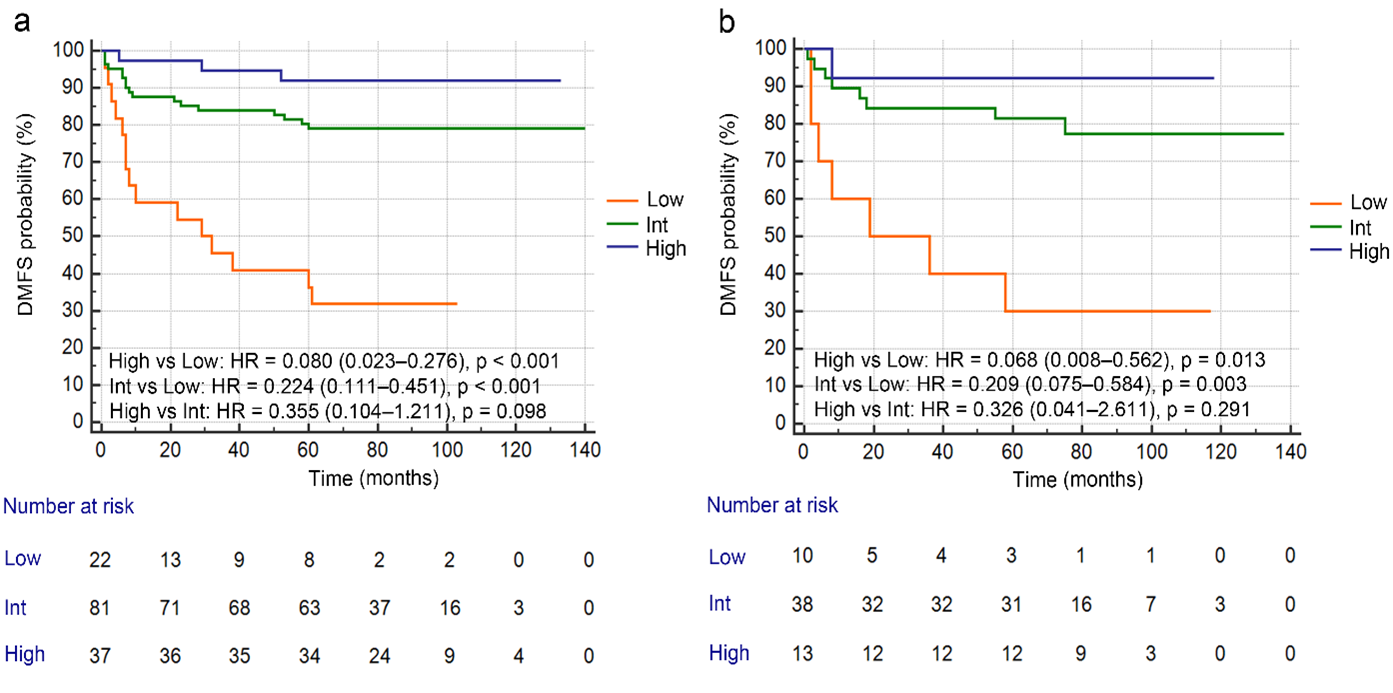
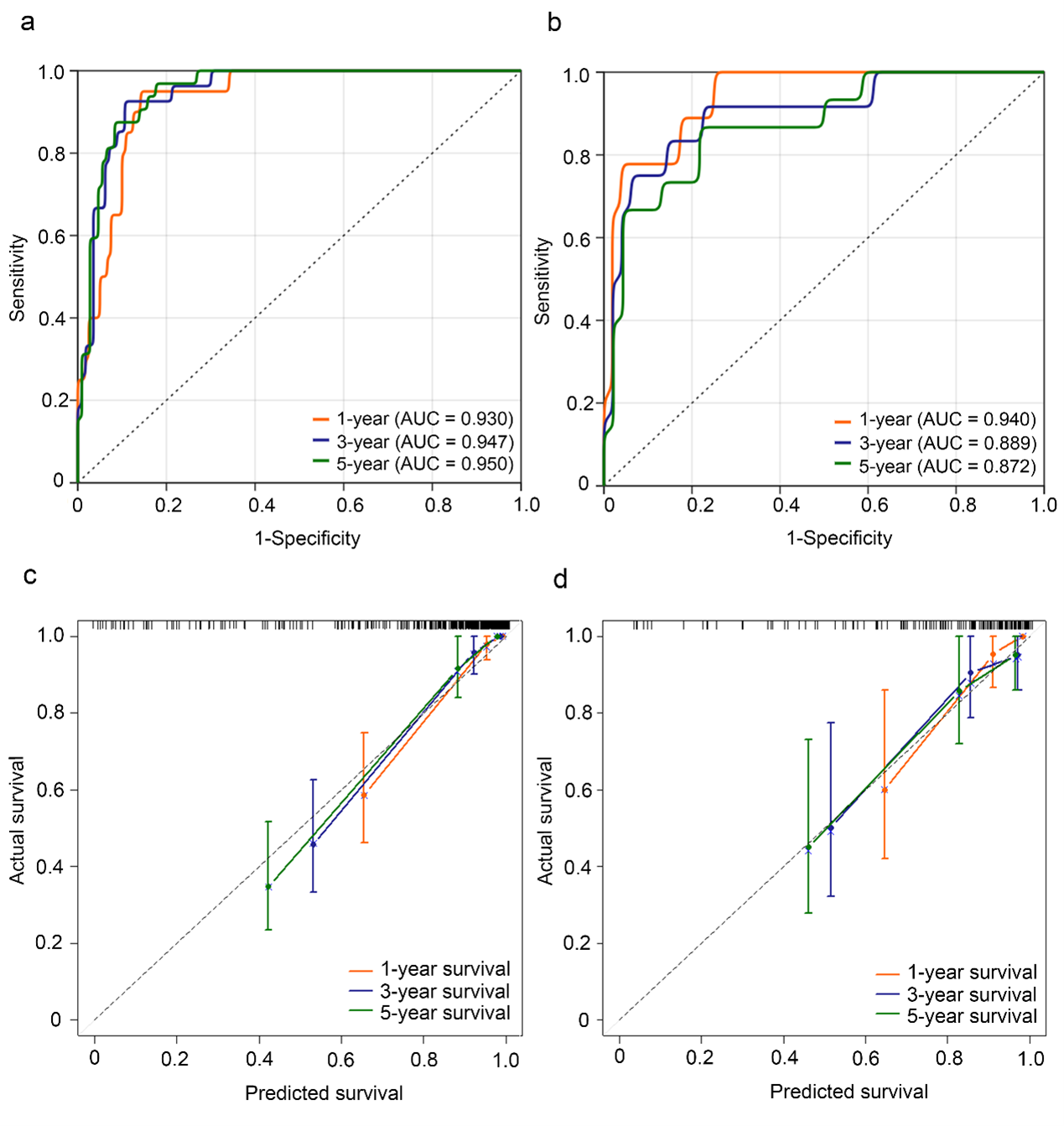
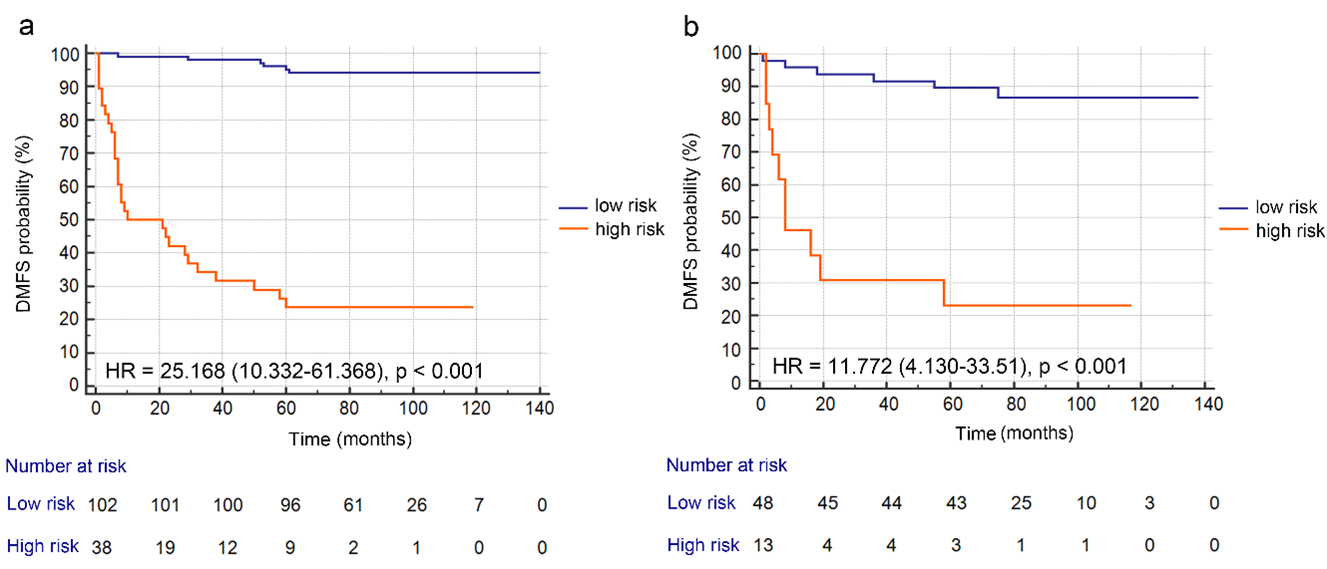
Results: In the final feature selection with LASSO-Cox analysis, seven radiomics features and seven pathomics features were included to construct the radiomics and pathomics signatures, respectively. The radiomics signature achieved C-indexes of 0.811 (95% CI, 0.746–0.877) in the training cohort and 0.752 (95% CI, 0.615–0.881) in the validation cohort for predicting DMFS. The pathomics signature achieved C-indexes of 0.713 (95% CI, 0.625–0.800) in the training cohort and 0.702 (95% CI, 0.569–0.835) in the validation cohort. After multivariable Cox analysis, clinical N stage, ISB, radiomics signature, and pathomics signature were identified as independent factors for DMFS prediction. The nomogram achieved C-indexes of 0.902 (95% CI, 0.870–0.933) in the training cohort and 0.848 (95% CI, 0.743–0.951) in the validation cohort, with corresponding AUCs of 0.950 (95% CI, 0.916–0.985) and 0.872 (95% CI, 0.769–0.976) for 5-year DMFS. Kaplan-Meier analysis demonstrated that a cutoff value of 0.188 effectively stratified patients into high- and low-risk DM groups in both the training and validation cohorts (both, p < 0.001).
Discussion and Conclusions: This study investigated a novel approach that integrates radiomics, pathomics, and ISB for predicting DM before treatment in LARC patients. The nomogram serves as a valuable tool for clinicians to identify high-risk DM patients and develop personalized neoadjuvant treatment strategies.
Acknowledgements
Funding: This research is supported by the National Natural Science Foundation of China [grant number 81971589].References
1. Bosset, J. F., Collette, L., Calais, G., et al. (2006) Chemotherapy with preoperative radiotherapy in rectal cancer, N Engl J Med 355, 1114-1123.
2. Sauer, R., Becker, H., Hohenberger, W., et al. (2004) Preoperative versus postoperative chemoradiotherapy for rectal cancer, N Engl J Med 351, 1731-1740.
3. van Gijn, W., Marijnen, C. A., Nagtegaal, et al. (2011) Preoperative radiotherapy combined with total mesorectal excision for resectable rectal cancer: 12-year follow-up of the multicentre, randomised controlled TME trial, Lancet Oncol 12, 575-582.
4. Fokas, E., Liersch, T., Fietkau, R., et al. (2014) Tumor regression grading after preoperative chemoradiotherapy for locally advanced rectal carcinoma revisited: updated results of the CAO/ARO/AIO-94 trial, J Clin Oncol 32, 1554-1562.
5. El Sissy, C., Kirilovsky, A., Van den Eynde, et al. (2020) A Diagnostic Biopsy-Adapted Immunoscore Predicts Response to Neoadjuvant Treatment and Selects Patients with Rectal Cancer Eligible for a Watch-and-Wait Strategy, Clin Cancer Res 26, 5198-5207.
Figures