0841
Ultrashort Echo Time (UTE) Spiral-VIBE MRI for Lung Nodule Detection and Radiomics Feature Stability Assessment1Department of Radiology, Affiliated Hospital 2 of Nantong University, Nantong, China, 2MR Application Predevelopment, Siemens Healthineers AG, Erlangen, Germany, 3MR Research Collaboration, Siemens Healthineers Ltd, Shanghai, China
Synopsis
Keywords: Lung, Lung, pulmonary nodules,Ultrashort Echo Time (UTE) Spiral-VIBE MR, Radiomics,Radiomics Stability
Motivation: This study aims to assess the efficacy of UTE-MRI in detecting lung nodules compared to CT and to evaluate the stability of radiomics features, along with the factors influencing them.
Goal(s): Through the advancement of UTE scanning technology, we strive to enable MRI to achieve lung nodule detection capability and stability on par with CT.
Approach: To facilitate the clinical integration of UTE technology for lung diseases, UTE scanning was conducted on patients presenting with lung nodules.
Results: UTE-MRI demonstrates a high detection rate for lung nodules larger than 6 mm, and it exhibits a high level of stability in radiomics features.
Impact: Our study shows UTE showcasing a remarkable ability to detect lung nodules larger than 6 mm and maintain consistent radiomics features across repeated scans. UTE holds potential as a radiation-reducing alternative to CT for regularly monitored patients with lung nodules.
Introduction
Magnetic Resonance Imaging (MRI) is a radiation-free imaging technique. However, its application in lung imaging has been hampered by technical constraints. In recent years, ultrashort echo (UTE) sequences have emerged as a promising technology capable of capturing short T2-weighted signals, which are gradually being used in the examination of lung diseases. In this study, we used a stack-of-spirals trajectory research sequence with adaptive TE. The sequence is based on variable-duration slice encoding to minimize T2* decay, Cartesian sampling along the through-plane direction, and in-plane spiral sampling to reduce the minimum time needed to cover k-space. Nevertheless, there is a paucity of studies comparing the efficacy of UTE versus CT assessing the reproducibility of histologic features through repeated UTE scans. This study aims to (1) evaluate the detection capabilities of UTE, contrast CT, and T1-Starvibe for lung nodules of varying sizes, locations, and types, and (2) assess the reproducibility of histological features based on semiautomatic segmentation of lung nodules in repeat UTE images. These efforts lay the groundwork for advancing imaging histology and providing objective, consistent information for disease diagnosis.Methods
In this prospective study, patients with lung nodules enrolled between February 2013 and October 2023 underwent examinations using conventional CT, MRI research sequence Spiral UTE, and T1-Starvibe on a 3T system (MAGNETOM Prisma, Siemens Healthineers, Erlangen, Germany) before surgery. Among them, 27 patients underwent repeated UTE scans, and semi-automatic outlining of lesion regions of interest (ROIs) was conducted on UTE sequence images using the Deepwise Medical platform (https://keyan.deepwise.com/). Eligibility criteria included: (1) pulmonary nodules detected by CT with a size <30 mm, (2) an interval between CT and MRI scans ≤7 days, (3) obtaining informed consent from study subjects, and (4) the absence of other significant underlying lung diseases. Exclusion criteria included: (1) calcified nodules and (2) dyspnea leading to failed or poor-quality chest CT and MR scans. Scanning parameters were as follows: Spiral UTE (TR/TE = 3.93/0.05, slice thickness 1 mm, FOV = 512×512 mm2, scan time: 8-10minutes, dependent on patient's respiration,Base revolution:512,Voxel size:1.0mm×1.0mm×1.0mm), and T1-Starvibe (TR/TE = 3.05/1.44, slice thickness 1 mm, FOV = 380×380 mm2, scan time: 5 minutes 30 seconds). Detection abilities of the three methods were compared using the Chi-square test for nodule detection rates, ANOVA for nodule diameters, Bland-Altman analysis to depict differences in nodule size between CT, UTE, and T1-Starvibe, and ICCs to assess agreement in nodule size measurements. Inter-assessor concordance was evaluated using Kappa's consistency test, while t-tests assessed inter-measurement agreement between ROI outlines. A significance level of P < 0.05 was considered statistically significant.Results
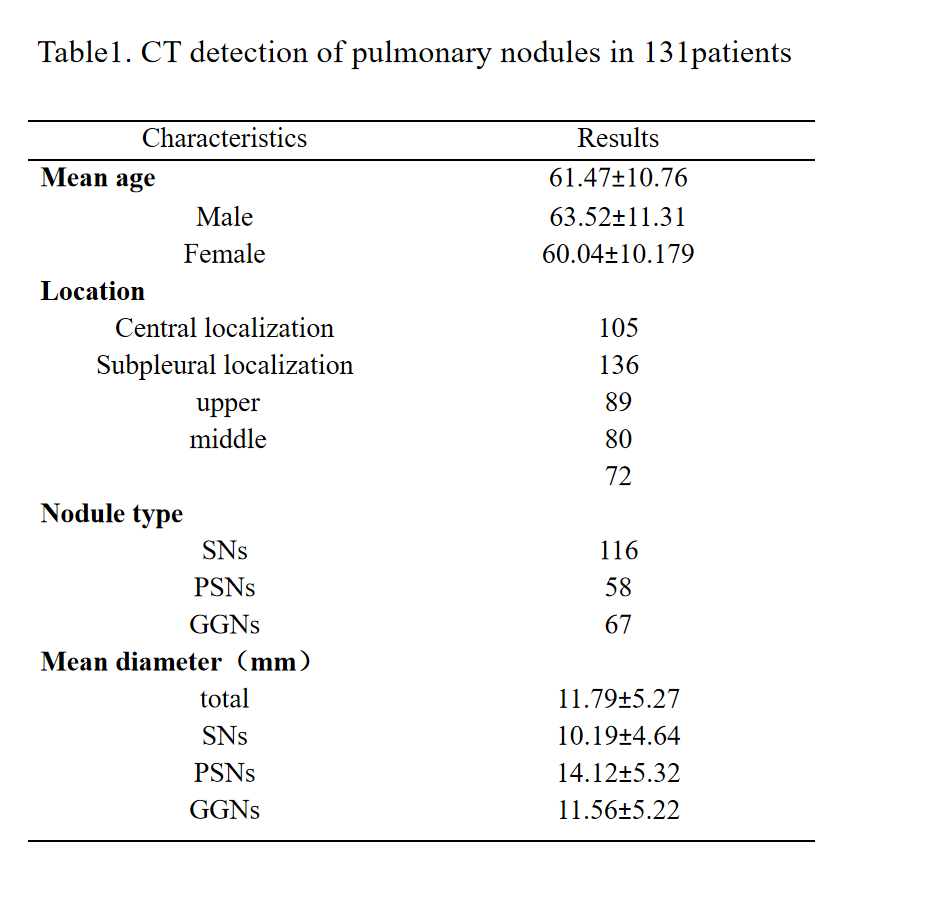
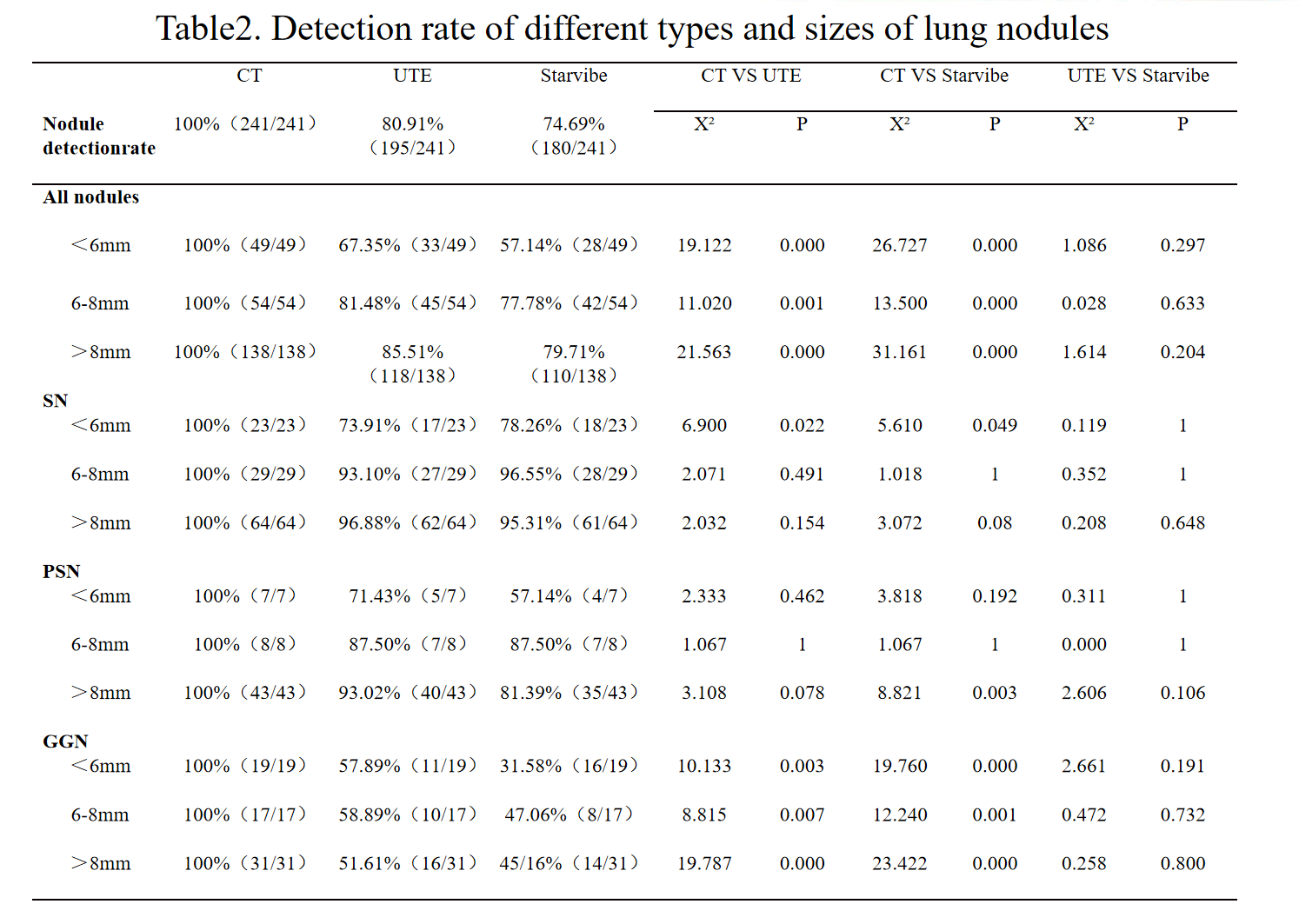
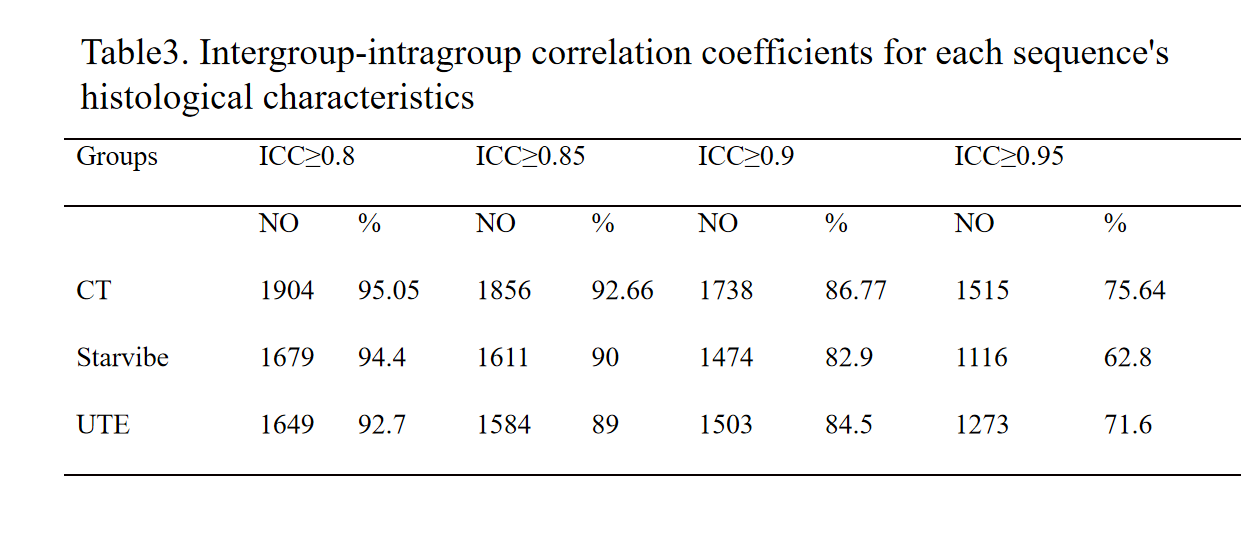
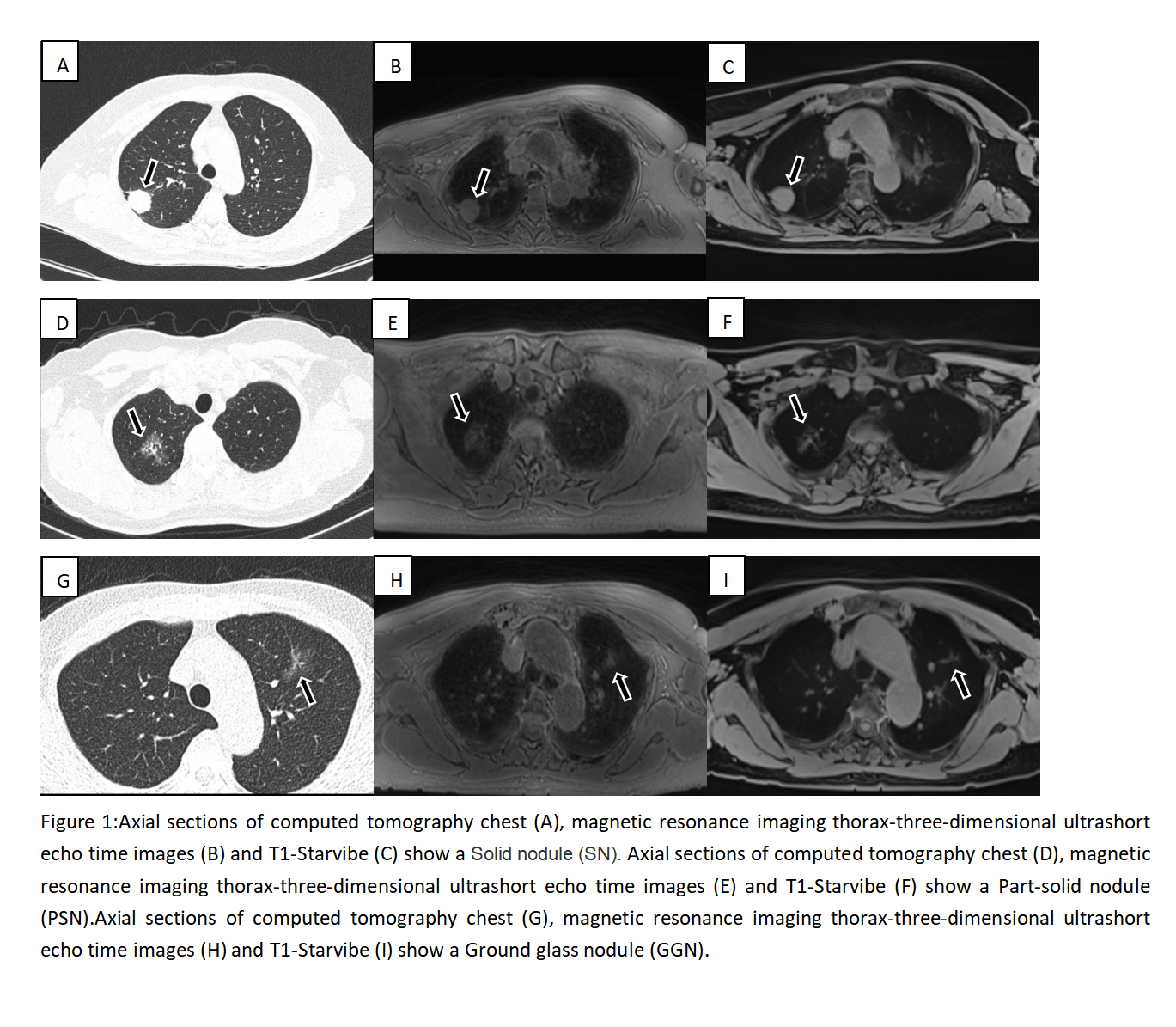
A total of 131 patients were included in the study, with 27 patients undergoing repeated scans. CT detected a total of 241 nodules in 131 patients, while UTE and T1-Starvibe detected 195 and 180 nodules, respectively, resulting in detection rates of 80.91% and 74.69%, respectively (P<0.05). The detailed results are shown in Table 1. Table 2 shown that when comparing UTE and T1-Starvibe to CT, statistically significant differences were observed for nodules <6mm, 6-8mm, and >8mm (P<0.05). Similarly, significant differences were found (P<0.05) when comparing UTE and T1-Starvibe to CT for nodules <6mm, 6-8mm, and >8mm. Notably, for ground glass nodules of 6-8 mm size, the difference was remarkable between CT and UTE as well as T1-Starvibe (P<0.05). While for solid, partially solid, and ground glass nodules larger than 8mm, the difference was statistically significant between CT and T1-Starvibe (P<0.05). Moreover, for ground-glass nodules larger than 8mm, the difference between CT and UTE was statistically significant (P<0.05). Different types of lung nodules are shown in Figure 1. UTE exhibited the highest sensitivity for detecting nodules in the central and upper lung fields, with detection rates of 82.35% and 86.52%, respectively. Strong agreement was observed between CT-measured lung nodules and those measured by UTE and T1-Starvibe, with ICCs of 0.971 and 0.949, respectively. Most eigenvalues for UTE images (ICC > 0.8) indicated excellent intra-observer reproducibility, inter-observer agreement, and reproducibility in short-term repeat scans (ICC ≥ 0.8). The detailed results are shown in Table 3.Conclusion and Discussion
MRI UTE sequences demonstrated high sensitivity for lung nodule detection, concordance in nodule size measurements, and good reproducibility in both intra- and inter-observer assessments, as well as short-term repeat scans. Although UTE is not yet poised to replace CT for lung nodule detection, it holds potential as a follow-up tool for patients with lung nodules.Acknowledgements
The authors thank Lei Cui MD, PhD (Department of Radiology, Affiliated Hospital of Nantong University), Xiayin Cao(Department of Radiology, Affiliated Hospital of Nantong University)Thomas Benkert (MR Application Predevelopment, Siemens Healthineers AG, Erlangen, Germany), Yunzhu Wu (MR Research Collaboration, Siemens Healthineers Ltd., Shanghai, China) for their valuable contributions to this study.References
[1] Yongxian Qian and Fernando E. Boada. Acquisition-Weighted Stack of Spirals for Fast High-Resolution Three-Dimensional Ultra-short Echo Time MR Imaging. Magnetic Resonance in Medicine 60:135–145 (2008).
[2] Fielden S, Mugler J, Miller W, et al. A Variable UTE stack-of-spirals sequence for 3D UTE imaging. In: 24rd Annual Meeting International of the Society for Magnetic Resonance in Medicine. 2016.
[3] Ohno Y, Takenaka D, Yoshikawa T, et al. Efficacy of Ultrashort Echo Time Pulmonary MRI for Lung Nodule Detection and Lung-RADS Classification. Radiology. 2022. 302(3): 697-706.
[4] Ma Y, Jang H, Jerban S, et al. Making the invisible visible-ultrashort echo time magnetic resonance imaging: Technical developments and applications. Appl Phys Rev. 2022. 9(4): 041303.
[5] Bae K, Jeon KN, Hwang MJ, et al. Comparison of lung imaging using three-dimensional ultrashort echo time and zero echo time sequences: preliminary study. Eur Radiol. 2019. 29(5): 2253-2262.
[6] Yang B, Metze P, Balasch A, et al. Reproducibility of functional lung parameters derived from free-breathing non-contrast-enhanced 2D ultrashort echo-time. Quant Imaging Med Surg. 2022. 12(10): 4720-4733.
[7] Huang YS, Niisato E, Su MM, et al. Applying Compressed Sensing Volumetric Interpolated Breath-Hold Examination and Spiral Ultrashort Echo Time Sequences for Lung Nodule Detection in MRI. Diagnostics (Basel). 2021. 12(1).
[8] Müller A, Jagoda P, Fries P, et al. Three-dimensional ultrashort echo time MRI and Short T(2) images generated from subtraction for determination of tumor burden in lung cancer: Preclinical investigation in transgenic mice. Magn Reson Med. 2018. 79(2): 1052-1060.
[9] Periaswamy G, Arunachalam VK, Varatharajaperumal R, et al.Comparison of Ultrashort TE Lung MRI and HRCT Lungs for Detection of Pulmonary Nodules in Oncology Patients. Indian J Radiol Imaging. 2022. 32(4): 497-504.
[10] Huang YS, Niisato E, Su MM, et al. Detecting small pulmonary nodules with spiral ultrashort echo time sequences in 1.5 T MRI. MAGMA. 2021. 34(3): 399-409.
[11] Darçot E, Jreige M, Rotzinger DC, et al. Comparison Between Magnetic Resonance Imaging and Computed Tomography in the Detection and Volumetric Assessment of Lung Nodules: A Prospective Study. Front Med (Lausanne). 2022. 9: 858731.
[12] Wang F, Lin X, Lin C, et al. Ability of three-dimensional 3-Tesla ultrashort echo time magnetic resonance imaging to display the morphological characteristics of pulmonary nodules: a sensitivity analysis. Quant Imaging Med Surg. 2023. 13(3): 1792-1801.
[13] Delacoste J, Dunet V, Dournes G, et al. MR Volumetry of Lung Nodules: A Pilot Study. Front Med (Lausanne). 2019. 6: 18.
[14] Wielpütz MO, Lee HY, Koyama H, et al. Morphologic Characterization of Pulmonary Nodules With Ultrashort TE MRI at 3T. AJR Am J Roentgenol. 2018. 210(6): 1216-1225.
[15] Olthof SC, Reinert C, Nikolaou K, et al. Detection of lung lesions in breath-hold VIBE and free-breathing Spiral VIBE MRI compared to CT. Insights Imaging. 2021. 12(1): 175.
[16] Kumar S, Rai R, Stemmer A, et al. Feasibility of free breathing Lung MRI for Radiotherapy using non-Cartesian k-space acquisition schemes. Br J Radiol. 2017. 90(1080): 20170037.
Figures