0834
Cerebral Quantitative Susceptibility Mapping in Neonates with Congenital Heart Disease1Radiology and Biomedical Imaging, UCSF, San Francisco, CA, United States, 2Pediatric Cardiology, UCSF, San Francisco, CA, United States, 3Pediatrics, UCSF, San Francisco, CA, United States
Synopsis
Keywords: Neuro, Quantitative Susceptibility mapping, congenital heart disease
Motivation: QSM has potential in monitoring altered cerebral oxygenation and quantifying cerebral microhemorrhages (CMH) in neonates with congenital heart disease (CHD).
Goal(s): To use 1) QSM to detect post-surgical changes in cerebral oxygenation and 2) a deep-learning algorithm to quantify CMH.
Approach: Cerebral susceptibility (χ) normalized to the ventricle was compared pre- vs. post-surgery and between CHD types. Deep-learning based quantification of CMH burden was compared pre- vs. post-surgery and assessed for relationship to cardiac bypass duration.
Results: Normalized post-surgery χ trended lower in neonates with transposition of great arteries compared to single ventricle physiology. Post-operative CMH burden was associated with cardiac bypass duration.
Impact: QSM-derived cerebral susceptibility post-surgery varies based on lesion type in congenital heart disease (CHD), supporting a potential role for QSM in detecting cerebral oxygenation changes. Cerebral microhemorrhages are common in neonates with CHD and are associated with surgical parameters.
Introduction
Children with congenital heart disease (CHD) often have abnormal neurodevelopment1 which is thought to be related to multiple factors including altered cerebral perfusion and oxygenation in early life. 2,3 Imaging-based metrics for early prediction of neurodevelopmental delay are critical for early intervention. Quantitative susceptibility mapping (QSM) shows potential due to 1) its ability to differentiate paramagnetic deoxyhemoglobin from diamagnetic oxyhemoglobin and 2) quantification of cerebral microhemorrhages (CMH) which are often encountered in neonates with congenital heart disease (CHD)4 and have been suggested to contribute to neurodevelopmental delay.5Methods
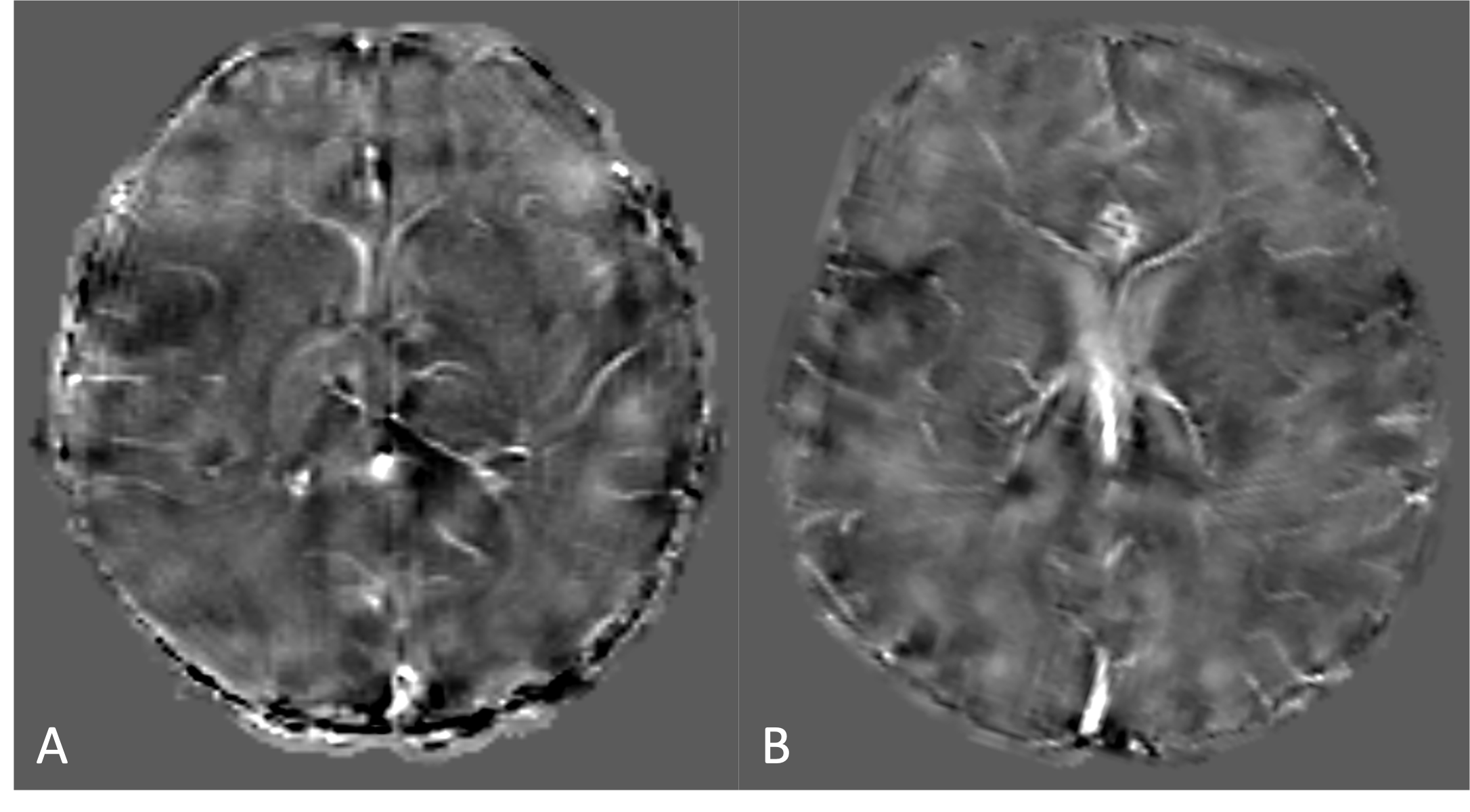
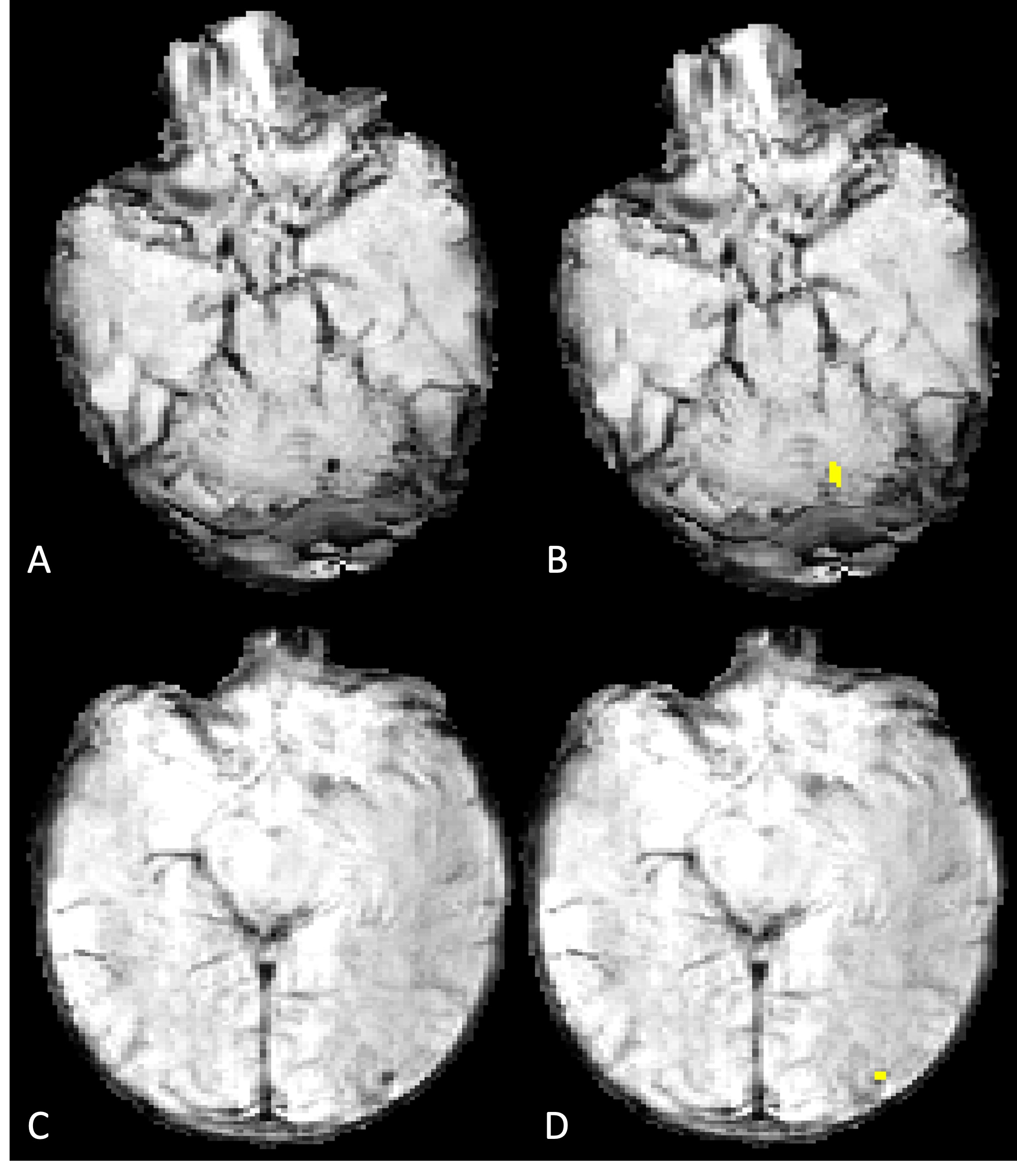
Neonates with critical CHD requiring surgery who underwent pre- and/or post-operative MRI with 3D T2* GRE were identified. QSM images were generated using custom-built processing pipeline6 and registered to the UNC brain atlas7 to derive total and regional (deep gray nuclei (DGN) and white matter (WM)) susceptibility (χ). The total and regional χ were normalized to the ventricle χ and compared between pre- and post-operative MRI and by CHD lesion type (transposition of great arteries (TGA) vs. single ventricle physiology (SVP)) using student’s t-test. We developed a deep-learning method for quantification of CMH.8 The number, total per-patient volume, and average per-lesion volume of CMH were compared between pre- and post-operative MRI using Wilcoxon rank sum test. The association of cardiopulmonary bypass duration during surgery with number and volume of CMH was assessed using linear regression.Results
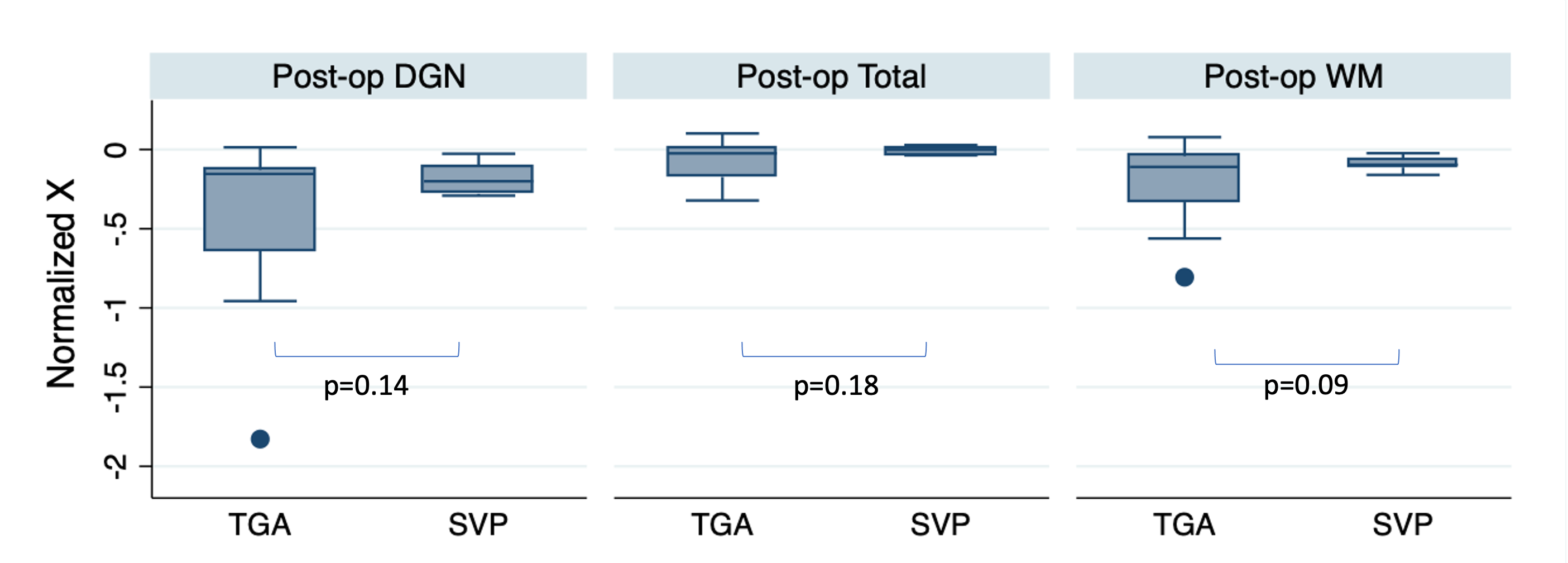
The study included 38 neonates who underwent either pre- or post-operative MRI with QSM (total 51 MRIs). The cohort was majority male (28/38, 73.7%) with a mean gestational age (GA) at birth of 38.8±1.0 weeks. The mean GA at time of pre-operative MRI was 39.8±1.2 weeks and at the time of postoperative MRI was 42.9±2.1 weeks. The cohort included 55.3% (21/38) TGA, 34.2% (13/38) SVP, and 10.5% (4/38) other CHD lesion.The mean normalized pre- vs. post-operative χ were -0.03±0.04 vs. -0.04±0.09 (p=0.81) for the whole brain, -0.21±0.24 vs. -0.32±0.39 (p=0.23) for the DGN and -0.12±0.10 vs. -0.16±0.19 (p=0.35) for the WM. The post-operative normalized total and regional χ trended to be lower in TGA compared to SVP (total: -0.06 vs. -0.01, p=0.18, DGN: -0.44 vs -0.19, p=0.14, WM: -0.23 vs. -0.09, p=0.09).
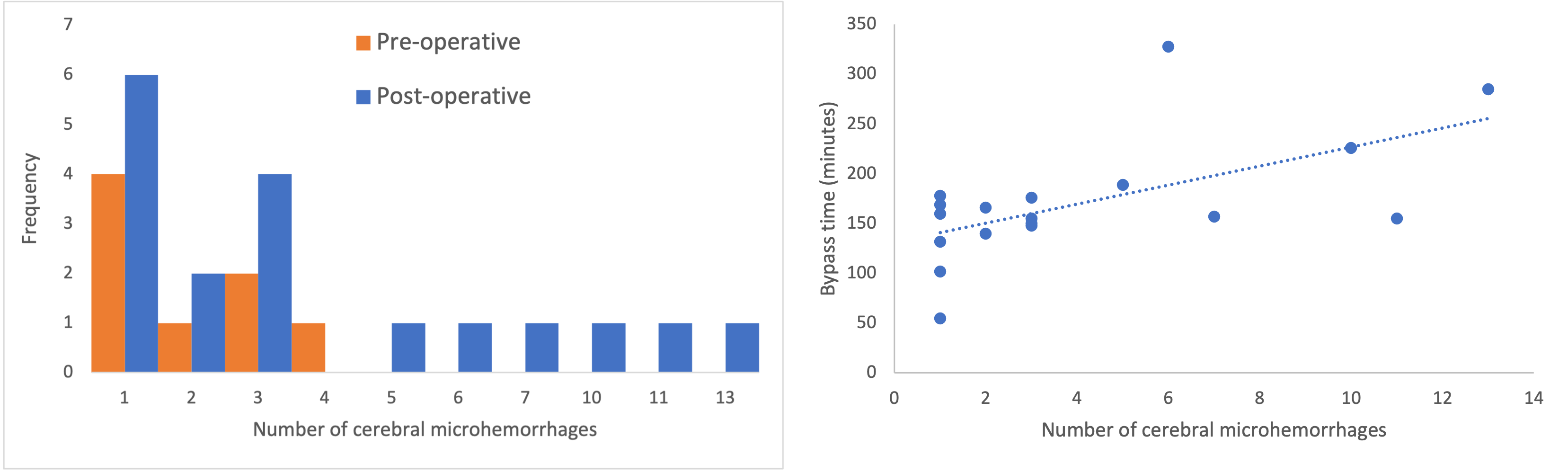
Automated quantification of CMH was successful in 22/38 neonates (26/51 MRIs). There was a trend towards more CMH postoperatively (Figure 3), though the median number of CMH was similar on pre- and post-operative MRI (median (IQR): 1.5 (1-3) vs. 3 (1-5.75), p=0.23). The total per-patient volume and average per-lesion volume of CMH were similar between pre- and post-operative MRI (p=0.12-0.66). Cardiac bypass duration was associated with number of CMH on post-operative MRI (b=0.04, p=0.009), but not with total or average CMH volume (p=0.19-0.90).
Discussion
Patients with TGA undergo definitive corrective surgery with resolution of hypoxia compared to patients with SVP who undergo palliative surgery with increased blood flow without correction of hypoxia in the first stage. This might explain the differences in postoperative normalized χ, which trended to be lower in patients with TGA which might be due to the correction of hypoxia and lower deoxyhemoglobin content (lower χ) compared to patients with SVP. This is consistent with prior literature using near infrared spectroscopy.9Automated quantification of CMH is feasible in neonates with CHD. CMH are often detected in neonates with CHD, but the number of lesions and total lesion volume are relatively low. Our study did not demonstrate a statistically significant change in number or volume of lesions between pre- and post-operative MRI which may be related to small sample size. There is an association between duration of cardiac bypass and number of post-operative CMH.
Conclusion
In this preliminary study, variations in post-operative χ in neonates with different CHD lesions demonstrate the potential of QSM in detecting altered cerebral hemodynamics. Low burden of CMH is often present in neonates with CHD and postoperative CMH appears to be related to cardiac bypass. Automated techniques can enable efficient quantification of CMH burden and future studies should assess its effect on neurodevelopmental outcomes.Acknowledgements
No acknowledgement found.References
1. Marino BS, Lipkin PH, Newburger JW, et al. Neurodevelopmental outcomes in children with congenital heart disease: evaluation and management: a scientific statement from the American Heart Association. Circulation 2012; 126(9): 1143-72.
2. Claessens NHP, Kelly CJ, Counsell SJ, Benders M. Neuroimaging, cardiovascular physiology, and functional outcomes in infants with congenital heart disease. Dev Med Child Neurol 2017; 59(9): 894-902.
3. Lee FT, Seed M, Sun L, Marini D. Fetal brain issues in congenital heart disease. Transl Pediatr 2021; 10(8): 2182-96.
4. Niwa T, Aida N, Takahara T, et al. Imaging and clinical characteristics of children with multiple foci of microsusceptibility changes in the brain on susceptibility-weighted MRI. Pediatr Radiol 2010; 40(10): 1657-62.
5. Soul JS, Robertson RL, Wypij D, et al. Subtle hemorrhagic brain injury is associated with neurodevelopmental impairment in infants with repaired congenital heart disease. J Thorac Cardiovasc Surg 2009; 138(2): 374-81.
6. Yao J, Morrison MA, Jakary A, et al. Comparison of quantitative susceptibility mapping methods for iron-sensitive susceptibility imaging at 7T: An evaluation in healthy subjects and patients with Huntington's disease. Neuroimage 2023; 265: 119788.
7. Shi F, Yap PT, Wu G, et al. Infant brain atlases from neonates to 1- and 2-year-olds. PLoS One 2011; 6(4): e18746.
8. Chen Y, Villanueva-Meyer JE, Morrison MA, Lupo JM. Toward Automatic Detection of Radiation-Induced Cerebral Microbleeds Using a 3D Deep Residual Network. J Digit Imaging 2019; 32(5): 766-72.
9. McQuillen PS, Nishimoto MS, Bottrell CL, et al. Regional and central venous oxygen saturation monitoring following pediatric cardiac surgery: concordance and association with clinical variables. Pediatr Crit Care Med 2007; 8(2): 154-60.
Figures