0833
Functional connectivity of motor resting-state networks in infants who are HIV-exposed uninfected in a South African birth cohort study1Paediatrics and Child Health, University of Cape Town, Cape Town, South Africa, 2Neuroscience Institute, Cape Town, South Africa, 3King's College London, London, United Kingdom, 4University College London, London, United Kingdom, 5Cardiff University, Wales, United Kingdom
Synopsis
Keywords: Neuro, Brain Connectivity, Neurodevelopment, Paediatrics, HIV exposure, resting state fMRI
Motivation: Children who are HIV-exposed uninfected present with an increased risk of adverse motor developmental outcomes. Little is known about the pathophysiological mechanisms governing these outcomes.
Goal(s): This study aimed to investigate functional connectivity within the motor resting-state network in infants who are HIV-exposed uninfected using resting-state functional MRI.
Approach: We used Group Independent Component Analysis to identify the motor resting-state network and multivariate linear regression was used to compare its functional connectivity between groups.
Results: Infants who are HIV-exposed uninfected showed significant connectivity alterations in 26 connections within the motor resting-state network when compared to infants who are unexposed.
Impact: Functional connectivity alterations observed in the motor resting-state network could be linked to adverse motor developmental outcomes in children who are HIV-exposed uninfected. Future research will look at associations between functional connectivity of motor resting state network and motor development.
Introduction
Interventions aimed at reducing mother-to-child transmission of HIV have been successful in reducing the number of perinatal paediatric HIV infections. This has resulted in a growing population of children who are HIV-exposed uninfected (CHEU), with 15.4 million CHEU reported globally in 2020 1. CHEU are exposed to HIV and often antiretroviral therapy (ART) during prenatal brain development, a critical stage for important cellular neurodevelopmental processes such as neurogenesis, neuronal migration, brain maturation and synaptogenesis 2,3. A growing body of literature has been found on brain development in CHEU, studies have found evidence for increased risk of impaired neurodevelopmental performance in cognition, language and motor function during the first two years of life, compared to children who are HIV-unexposed (CHU) 4. Potential pathophysiological mechanisms governing impaired motor development in CHEU have been identified, with significant associations reported with quantitative inflammatory biomarkers 5, and regional neurometabolic signatures 6. The development, refinement and maturation of brain functional networks occurs rapidly during the first months and years of life and our current understanding of functional networks has been primarily informed through the study of spontaneous intrinsic brain activity at rest using resting-state functional MRI (RS-fMRI). High order functional brain networks including the posterior default mode, salience and language networks, have been found to be associated with language outcomes in young typically developing children 7. The present study aimed to investigate functional connectivity within the motor resting-state network in infants who are HIV-exposed and matched controls.Methods
High field MRI data were acquired from 59 six-month-old infants enrolled in a longitudinal birth cohort study, with 394 mothers and their infants recruited from local community clinics in Gugulethu, in Cape Town, South Africa. Using a 16-channel infant head coil, 360 functional RS-fMRI volumes were acquired during natural sleep on a 3 Tesla Siemens Skyra MRI scanner using the following parameters: slice thickness 2.0mm, voxel size 2.0×2.0×2.0 mm, FOV = 216×216×144mm3, TR/TE = 940.0 /35.0 ms, flip angle 52°. RS-fMRI data were pre-processed in AFNI and were registered onto the UNC-BCP 4D Infant Brain Volumetric Atlas 8. This was followed by spatial smoothing and denoising by regressing six motion parameters. We used group Independent Component Analysis (ICA) to compute and identify spatiotemporally distinct patterns of the motor resting state network (RSN) using the MELODIC function in FSL 9. The motor RSN was visually identified and functional connectivity within the network was determined by calculating Pearson correlation (r) coefficients between the mean time series for each atlas region of interest (ROI) that falls within the motor network and every other ROI within the network. Between-group ROI connectivity differences were investigated using multivariate linear regression correcting for child sex, age at the scan, prenatal alcohol exposure and maternal depression. A Bonferroni correction was applied to correct for multiple comparisons.Results
After quality control measures, 41 infants (14 CHEU, 27 CHU, 61% Male) had usable RS-fMRI data available, with a mean age of 40.6 weeks at the MRI visit. Within the motor RSN, there were 31 ROIs with 465 connections. CHEU showed greater connectivity in 26 ROI connections within the motor RSN when compared to CHU. Some of the group connectivity differences were found bilaterally between the following regions: the caudal anterior cingulate and post central gyrus (left, B=0.18, SE=0.038, p=0.004 ; right, B=0.13 , SE=0.04, p =0.002), the caudal anterior cingulate and pre central gyrus (left, B=0.13, SE=0.04 , p=0.003 ; right, B=0.16 , SE=0.04, p=0.001) and the post central gyrus and superior frontal (left, B=0.15, SE=0.05, p=0.004; right, B=0.20 , SE=0.06, p=0.008). These findings held after correcting for covariates and multiple comparisons.Discussion
Increased functional connectivity within the motor RSN as reported in our study, potentially reflects aberrant processing within the motor RSN of CHEU. Functional connectivity increases have previously been observed in children with other neurodevelopmental disorders, such as attention-deficit/hyperactivity disorder10 and early-onset schizophrenia11, and has been linked to neurotransmitter imbalances, differences in sensory processing and integration, and compensatory mechanisms. Furthermore, increased functional connectivity within motor regions were found to be associated with motor, socio-communicative and executive functions in children and adolescents with autism spectrum disorder12.Conclusion
This is the first study reporting functional connectivity alterations in the motor RSN of CHEU. Future research will look at associations between functional connectivity of motor RSN and motor development in CHEU. Exploring the relationship between RSNs and neurodevelopmental outcomes can help us better understand the pathways through which HIV exposure impacts motor development in CHEU.Acknowledgements
We are hugely thankful to the mothers and their infants for their participation in the study. We would also like to express our gratitude to the Khula recruitment team in South Africa for their hard work and support throughout the duration of the project, as well as the radiographers at the Cape Universities Body Imaging Centre (CUBIC). This research is supported by funding from the Wellcome Leap 1kD Program to DCA, SCW, DKJ, KAD.
References
1 Slogrove, A. L., Powis, K. M., Johnson, L. F., Stover, J. & Mahy, M. Estimates of the global population of children who are HIV-exposed and uninfected, 2000–18: a modelling study. The Lancet Global Health 8, e67-e75 (2020). https://doi.org:https://doi.org/10.1016/S2214-109X(19)30448-6
2 Silbereis, J. C., Pochareddy, S., Zhu, Y., Li, M. & Sestan, N. The Cellular and Molecular Landscapes of the Developing Human Central Nervous System. Neuron 89, 248-268 (2016). https://doi.org:10.1016/j.neuron.2015.12.008
3 Dehorter, N. & Del Pino, I. Shifting Developmental Trajectories During Critical Periods of Brain Formation. Front Cell Neurosci 14, 283 (2020). https://doi.org:10.3389/fncel.2020.00283
4 Hertzman, C. & Wiens, M. Child development and long-term outcomes: a population health perspective and summary of successful interventions. Soc Sci Med 43, 1083-1095 (1996). https://doi.org:10.1016/0277-9536(96)00028-7
5 Wedderburn, C. J. et al. Neurodevelopment of HIV-exposed uninfected children in South Africa: outcomes from an observational birth cohort study. Lancet Child Adolesc Health 3, 803-813 (2019). https://doi.org:10.1016/s2352-4642(19)30250-0
6 Sevenoaks, T. et al. Association of maternal and infant inflammation with neurodevelopment in HIV-exposed uninfected children in a South African birth cohort. Brain, Behavior, and Immunity 91, 65-73 (2021). https://doi.org:https://doi.org/10.1016/j.bbi.2020.08.021
7 Williams, S. R. et al. 1H-MRS neurometabolite profiles and motor development in school-aged children who are HIV-exposed uninfected: a birth cohort study. Frontiers in Neuroscience 17 (2023). https://doi.org:10.3389/fnins.2023.1251575
8 Chen, B. et al. Resting state functional networks in 1-to-3-year-old typically developing children. Developmental Cognitive Neuroscience 51, 100991 (2021). https://doi.org:https://doi.org/10.1016/j.dcn.2021.100991
9 Chen, L. et al. A 4D infant brain volumetric atlas based on the UNC/UMN baby connectome project (BCP) cohort. Neuroimage 253, 119097 (2022). https://doi.org:10.1016/j.neuroimage.2022.119097
10 Beckmann, C. F. & Smith, S. M. Probabilistic independent component analysis for functional magnetic resonance imaging. IEEE Trans Med Imaging 23, 137-152 (2004). https://doi.org:10.1109/tmi.2003.822821
Figures
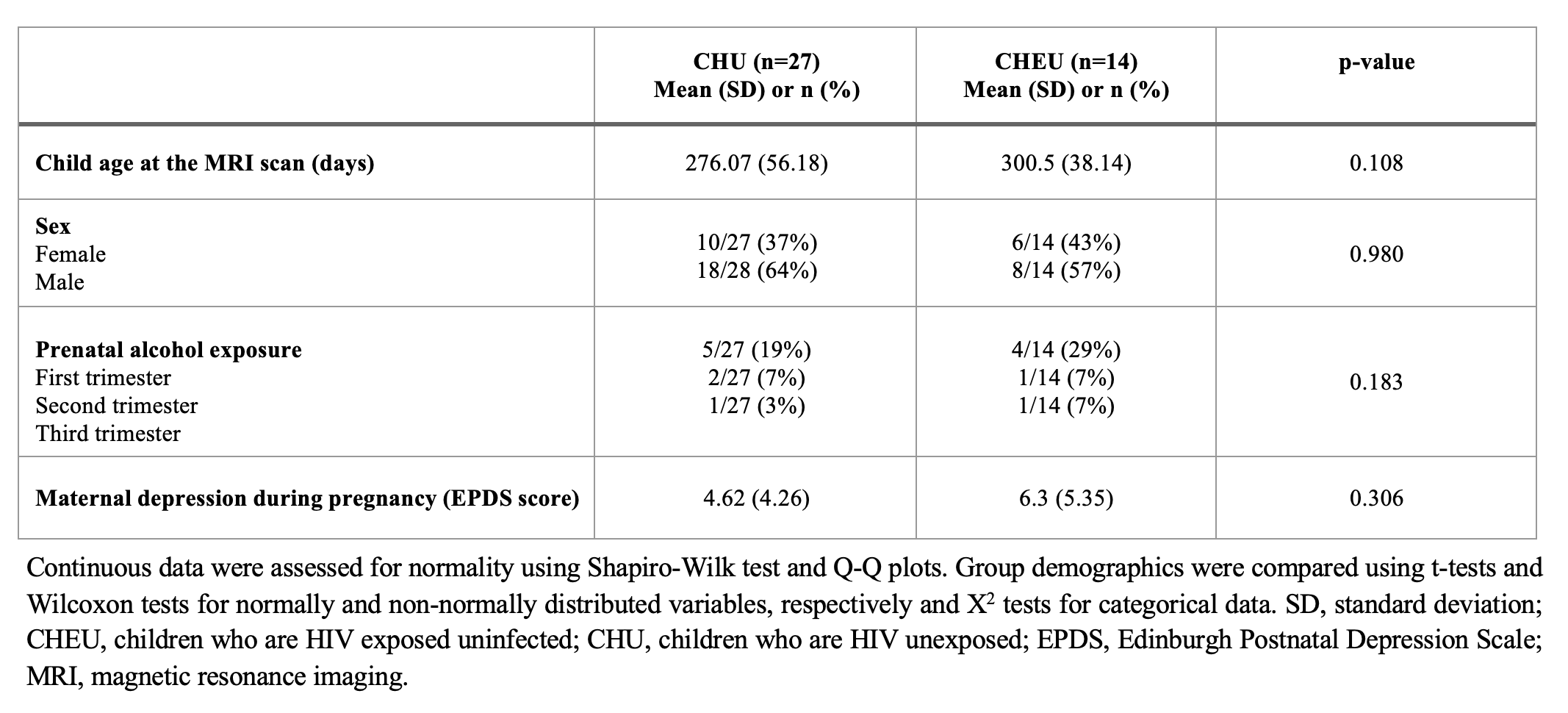
Table 1 | Sample demographics according to HIV exposure.
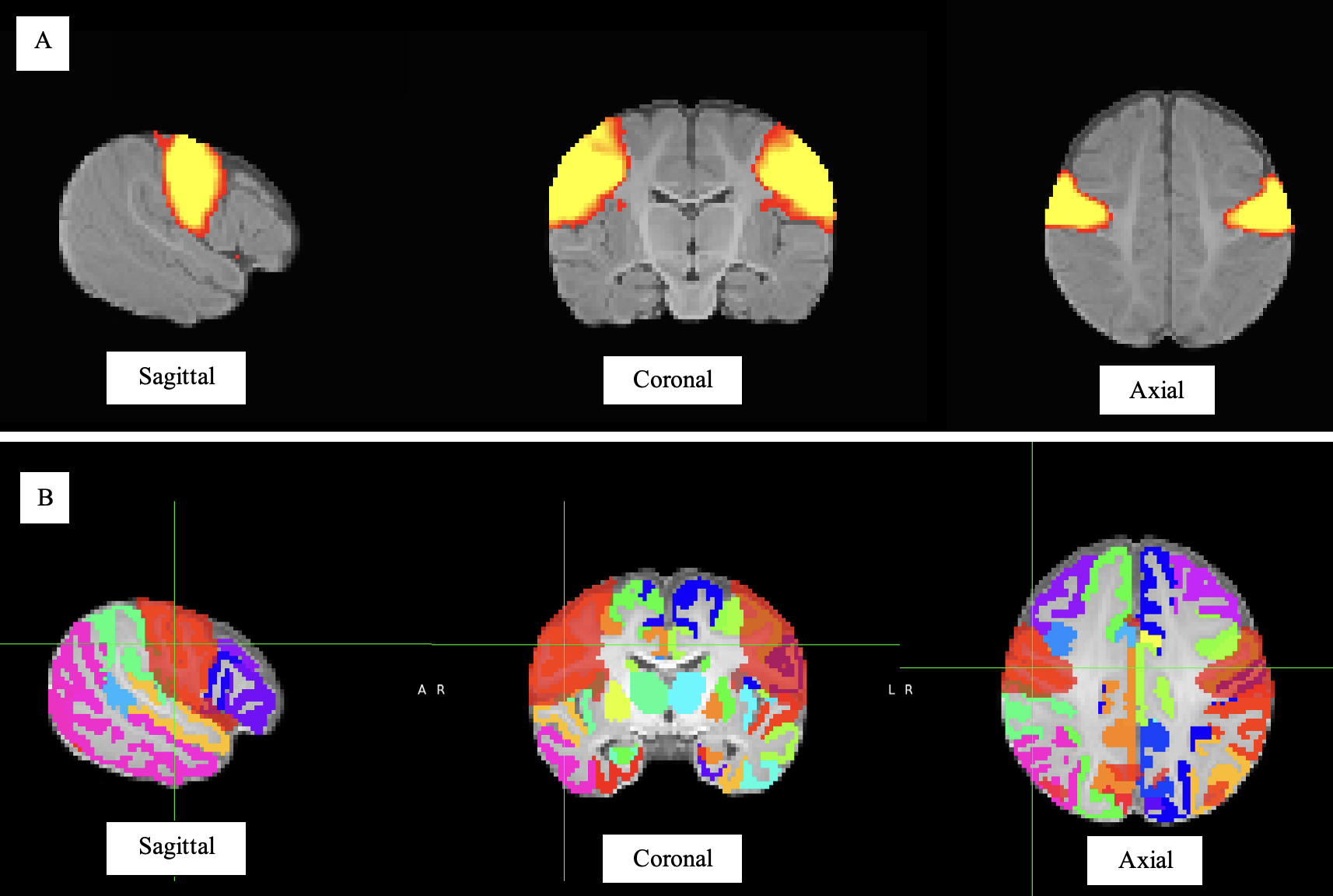
Figure 1 | Group ICA estimated Motor RSN. A) Motor RSN at a Z score > 0.3. B) Brain atlas areas falling within the motor RSN, where the motor RSN is indicated as a translucent red overlaying the brain ROIs on the atlas. Sagittal, coronal and axial views are shown. ICA, Independent component analysis; RSN, resting state network
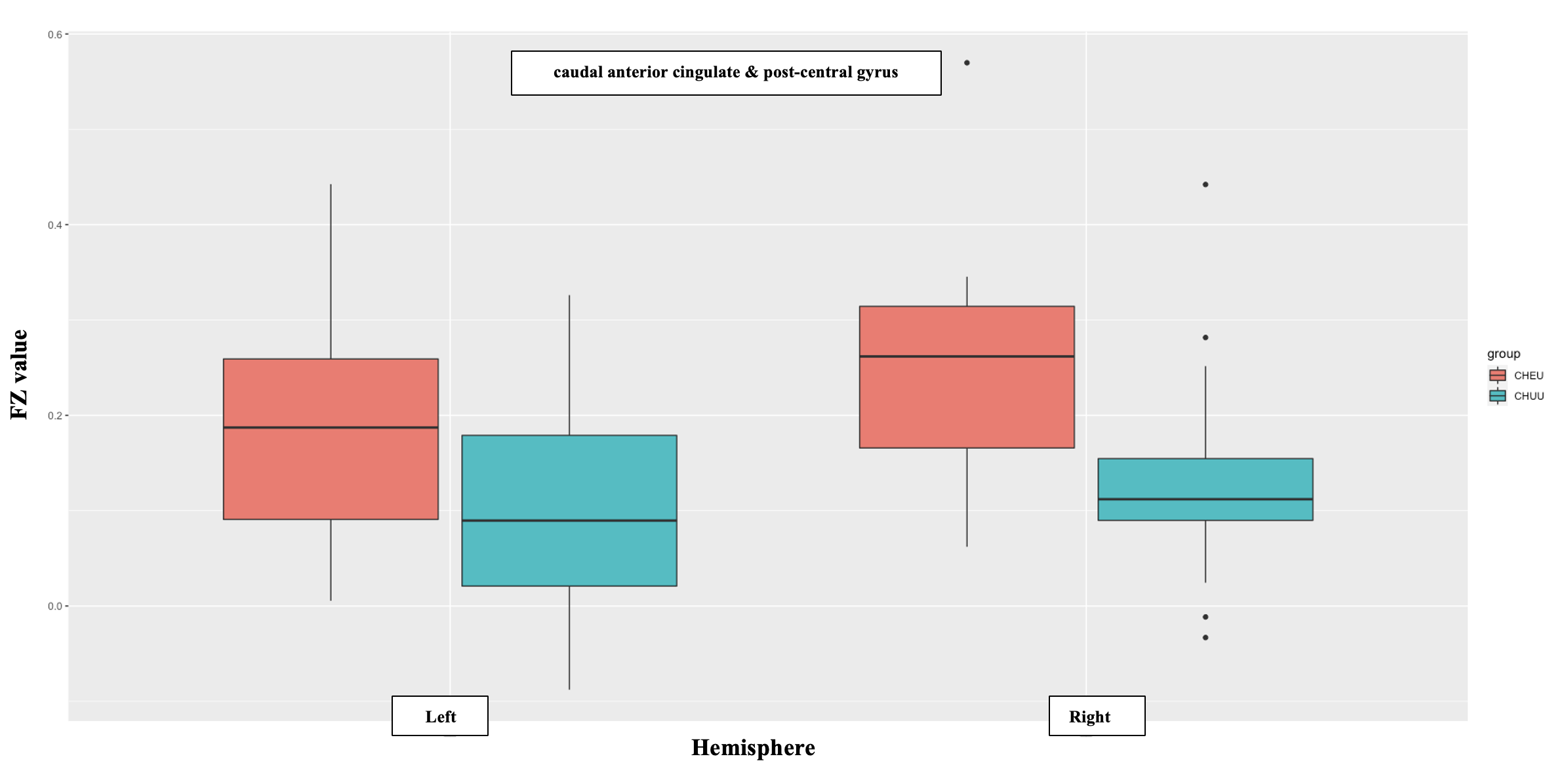
Figure 2 | Plots (showing median and IQR) of bilateral functional connectivity between the caudal anterior cingulate and the post-central gyrus in CHEU and CHU. FZ, Fourier-transformed; ROI, region-of-interest; CHEU, children who are HIV-exposed uninfected; CHU, children who are HIV-unexposed.
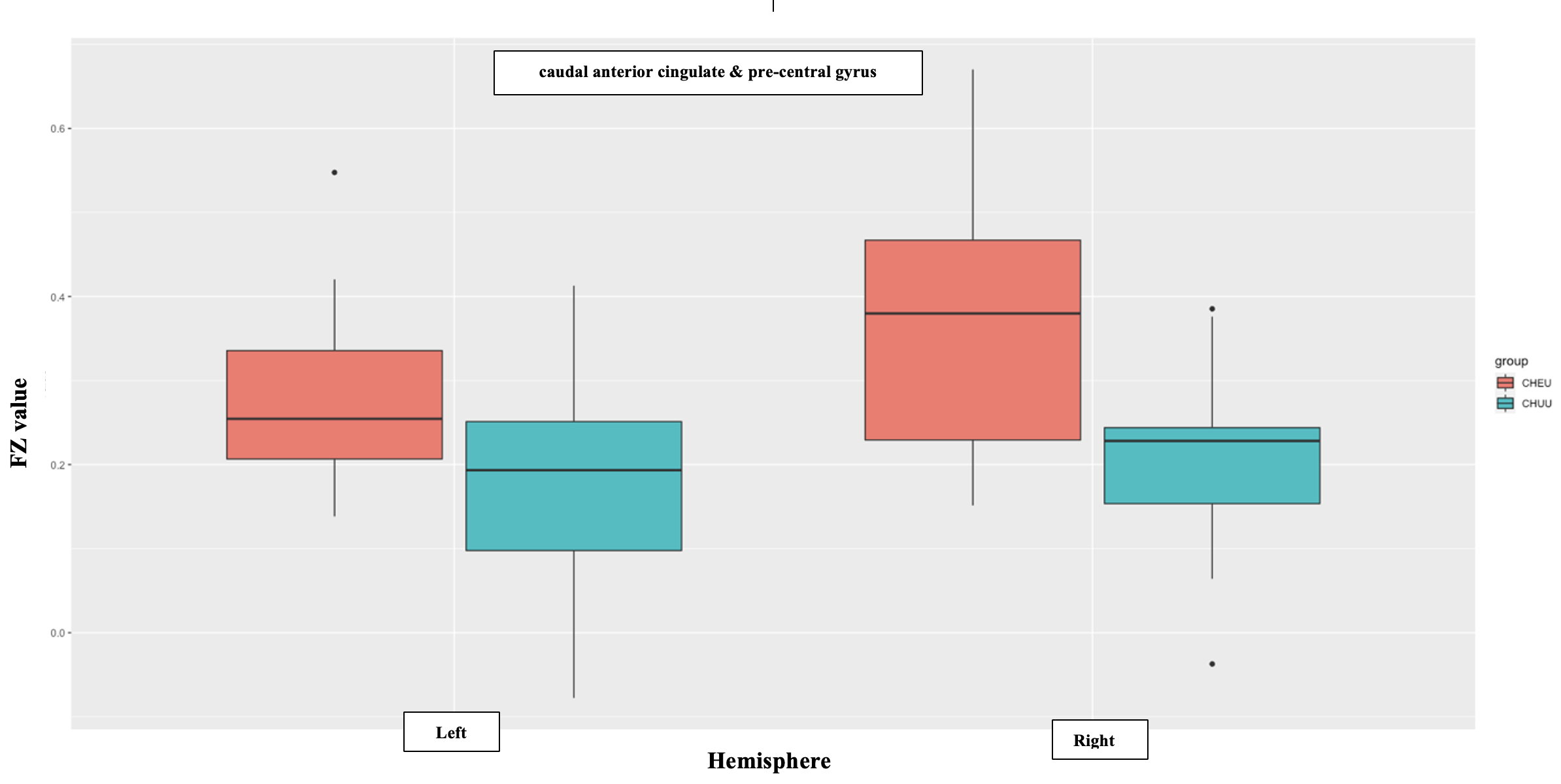
Figure 3 | Plots (showing median and IQR) of bilateral functional connectivity between the caudal anterior cingulate and the pre-central gyrus in CHEU and CHU. FZ, Fourier-transformed; ROI, region-of-interest; CHEU, children who are HIV-exposed uninfected; CHU, children who are HIV-unexposed.
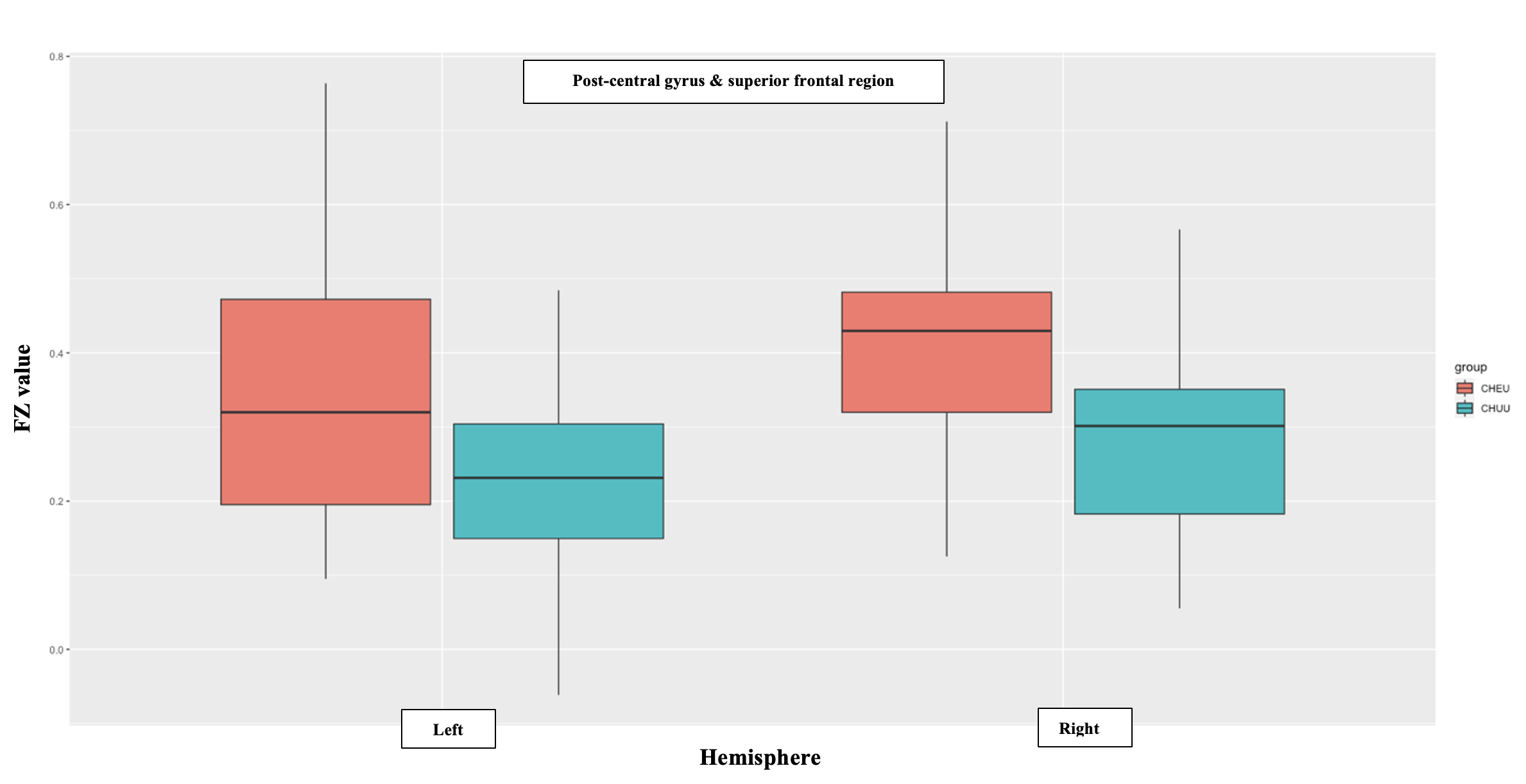
Figure 4| Plots (showing median and IQR) of bilateral functional connectivity between the post-central gyrus & superior frontal region in CHEU and CHU. FZ, Fourier-transformed; ROI, region-of-interest; CHEU, children who are HIV-exposed uninfected; CHU, children who are HIV-unexposed.